Reoperation of the Extraocular Muscles
John S. Davis
Albert W. Biglan
No matter how much is known about a problem that causes strabismus, or how well strabismus is evaluated, or how precisely the corrective procedure is done, with time, either early in the postoperative period or months or years after the procedure, satisfactory ocular alignment may deteriorate, and reoperation of the extraocular muscles may be required. Reoperation may be necessary to re-establish ocular alignment, to eliminate diplopia, to re-establish binocularity, or to provide improved self-image, self-esteem, and cosmesis.
The exact effect of strabismus surgery for each individual patient is difficult to predict. For any type of strabismus procedure that is performed, there will be an expected number of patients who will experience overcorrection, and this should be matched by an equal number of patients who experience undercorrection.1 Conceptually, results of strabismus surgery should fit a Gaussian distribution (Fig. 1). If enough procedures are performed, surgeons will have patients with undercorrected and overcorrected strabismus through no fault of the surgeon.
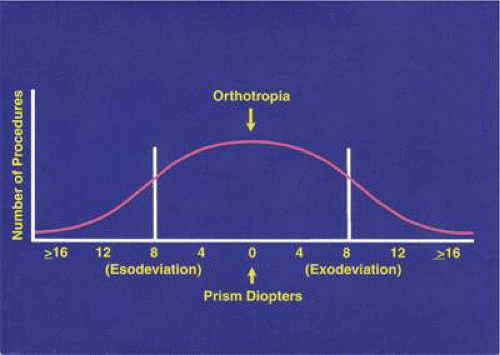 Fig. 1. A Gaussian distribution curve for correction of horizontal strabismus surgery. In most situations, a result of ±8 Δ of residual deviation is considered acceptable. |
In 1961, Cooper,2 in an article addressing the management of secondary exotropia, listed other causes for unsatisfactory results. Some of these contributing causes are poor surgical planning; faulty, inaccurate, or incomplete diagnosis; little-understood innervational factors; faulty technique; and unsuspected or undiscovered anatomic abnormalities.
Before surgery is performed for strabismus, the goals of surgical realignment of the eyes should be agreed upon by the surgeon and the patient. If the initial attempt to accomplish these goals results in unsatisfactory alignment, or a satisfactory alignment of the visual axes is obtained but later deteriorates, the surgeon is still committed to the initial agreement. Failure to achieve a desired result or loss of satisfactory ocular alignment is disappointing to both the patient and the ophthalmologist. Once indications are met for additional surgery, the ophthalmologist should swallow his or her pride, apply objective analysis to the problem, and recommend appropriate corrective procedures. Avoidance or delay in this decision may undermine the doctor-patient relationship and may compromise the patient’s prognosis. One cause for delay in reintervention is the failure to adequately understand the cause (or complexity) of the strabismus problem. If a surgeon feels uncomfortable analyzing a problem, or a technically difficult procedure is required, referral to an ophthalmologist who has better understanding of the condition or possesses skills necessary to correct the defect in alignment is the best course of action.
The surgeon and family must have realistic expectations of the results of strabismus surgery. Some clinical presentations will have excellent prognosis for both alignment and binocularity. Other conditions, such as those with restriction, paresis/paralysis, neurologic defects, or poor vision, may not have as good a prognosis. In these latter situations, a perfect result may be too much to expect, and the surgeon should emphasize this. After analysis of the problem, realistic goals of surgery should be set, and the goals should be discussed with the patient or parents. The possibility and likelihood of postoperative nonsurgical interventions and additional procedures should be discussed.
INDICATIONS FOR SURGERY
The indications for reoperation will usually reflect similar indications for the initial procedure. Nonsurgical methods of managing the problem (e.g., glasses, occlusion, prisms, time) should be considered before surgery is recommended. In addition to failure of nonsurgical methods, indications will also be influenced by the age of the patient, the level of sensory development, and the cause of strabismus. Indications include placement of the eyes in a position where binocular vision can develop, elimination of diplopia, correction of an abnormal head posture, and improvement in cosmesis and self-image.
Although it is the surgeon’s responsibility to achieve a mechanical solution to a given strabismus problem, this should be undertaken only with a full understanding of the sensory status to achieve the optimal functional benefit from the procedure. The level of maturation or plasticity of the visual system, the presence of fusional control of ocular alignment, and the presence of sensory adaptations or diplopia are some factors that influence outcome. One may distinguish between situations in which the surgeon is attempting to create a favorable alignment to facilitate development of binocularity (e.g., infantile esotropia) from conditions wherein the goal of surgery is to re-establish a previously normal binocular sensory state (e.g., diplopia related to an acquired sixth nerve palsy in an adult).
Reintervention to correct strabismus is indicated if a technical problem occurred immediately after the initial procedure. A muscle that has become disinserted or is “lost” postoperatively requires immediate exploration and correction of the problem (Figs. 2 and 3). A similar situation may occur when a previously operated muscle retracts (“slips”) inside the muscle capsule (Fig. 4). The slipped muscle will appear paretic, and early surgical intervention should be considered. The clinical pictures of these technical failures are very similar. There is poor function of the affected rectus muscle, and the induced strabismus will be noncomitant. Operations may be performed on the incorrect eye muscles or eye (Fig. 5). If this occurs, reoperation should not be delayed.
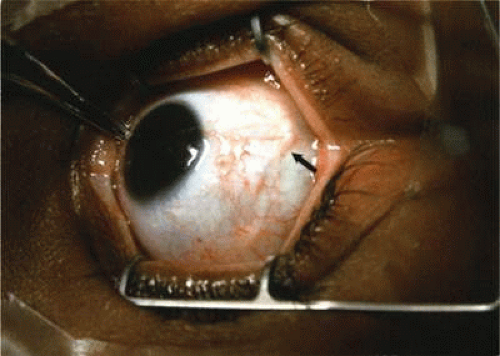 Fig. 2. This 8-year-old patient had her lateral rectus recessed 4 days before referral. Twenty-five Δ of esotropia and absent abduction were noted. The insertion was “empty” in appearance, and an untied suture could be visualized underneath the conjunctiva (arrow). |
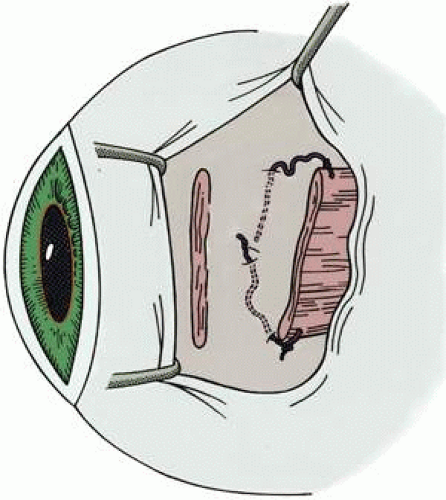 Fig. 3. This diagram demonstrates the findings of surgical exploration of the patient in Figure 2. |
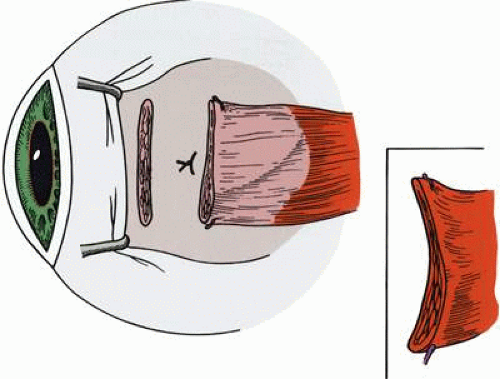 Fig. 4. Failure to incorporate a portion or the entire tendon of the muscle when sutures are placed near the insertion can permit a portion or all of the muscle to slip posteriorly and produce an exaggerated recession effect. On exploration, the muscle capsule will be present but the tendon/muscle will be retracted within the muscle capsule. |
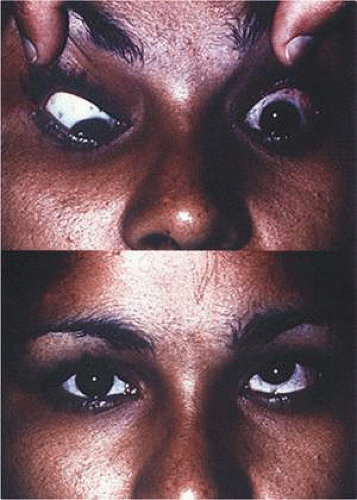 Fig. 5. This patient was referred for correction of a left hypertropia following strabismus surgery (lower). When the patient looks down (upper), there is poor infraduction. Exploration confirmed that the left inferior rectus had been recessed instead of the left medial rectus. (Courtesy of John Simon, M.D.) |
More commonly, reoperation is required when an unexpected unsatisfactory result is encountered in the absence of an obvious technical problem. This includes the occurrence of overcorrections and undercorrections. A general guideline for recommending correction of horizontal strabismus is the presence of diplopia or the presence of a residual deviation of 12 to 15 Δ (prism diopters) or greater. Because fusional control of vertical deviations is generally less than fusional control of horizontal deviations, patients with diplopia and vertical deviations greater than 5 Δ are candidates for reoperation. A horizontal rectus muscle that has been inadvertently offset vertically when reattached to the globe may induce an unexpected hypertropia.
Unexpected results may occur from failure to recognize a problem before the initial procedure. Examples include masked bilateral superior oblique palsy, undiagnosed A or V patterns, and lateral incomitance in exotropia. They also may occur months or years after procedures that were accompanied by an exuberant healing response due to excessive bleeding, heavy use of cautery, excessive use of blunt dissection with cotton-tipped applicators, or when the integrity of the orbital fat has been violated, all of which can cause fibrotic restriction.3 Failure to adequately balance the forces of the extraocular muscles due to, for example, excessive recession or resection of a rectus muscle may also result in the creation of incomitance, unsatisfactory distance-near disparity, and overcorrections and undercorrections.4,5 Other undesirable results after strabismus operations include residual head postures or tilts, and creation of ocular torsion.
Re-emergence of the original problem is another indication for reoperation. This may be due to insufficient fusional control of small degrees of residual misalignment in conditions such as infantile esotropia. It may also occur when strabismus is associated with decreased vision in one eye and fusional control is absent. The presence of a paretic muscle or muscles (e.g., third, fourth, or sixth cranial nerve palsy) may initially result in a good response to surgical alignment, but the innervation to the muscle/muscles may be so compromised that the alignment will later deteriorate and additional intervention will be necessary. The presence of scar around the extraocular muscles or in the subconjunctival tissue may cause recurrence of the original misalignment by mechanical restriction. Tendon-scar remodeling is associated with late overcorrection (Fig. 6) This phenomenon is thought to be more common with the use of adjustable sutures, although we have also observed this after conventional nonadjustable strabismus surgery.6
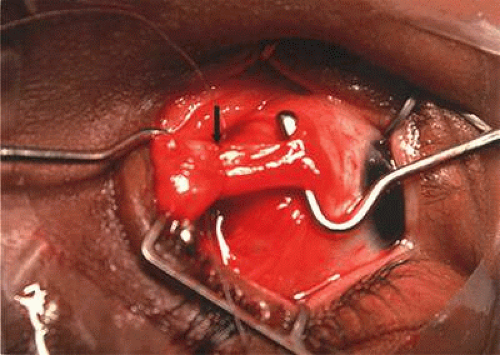 Fig. 6. Tendon-scar remodeling. This patient had late consecutive exotropia. Intact medial rectus (arrow) incorporated in suture; anterior is elongated tendon-scar. |
The presence of an underlying condition that has variable or progressive characteristics may lead to additional strabismus surgery. Conditions such as progressive external ophthalmoplegia, thyroid ophthalmopathy, myasthenia gravis, and ocular myositis will demonstrate variability in the size of the deviation. In these cases, it is important to exercise restraint. Surgery should not be recommended until stability in prism-cover measurements is obtained and any inflammatory component has resolved.
Some reoperations are necessary because a problem, different from the original strabismus, was not be present at the time of the first operation but emerges later as part of the natural history of the original problem. The occurrence of dissociated vertical deviation and overaction of the inferior oblique muscles after correction of infantile esotropia are two examples of this. Emergence of a contralateral superior oblique palsy, i.e., unmasking a bilateral superior oblique palsy, after the first operation, is another example.7
In unusual situations, the initial operation may be the first step in a planned staged procedure. This may occur in a condition that requires correction of a complex cyclovertical muscle problem, such as third cranial nerve palsy. In such cases, reoperation is anticipated from the beginning.
In cases where repair of the strabismus is principally cosmetic, it is important that the surgeon not be satisfied with an appearance that is unsatisfactory to the patient or parent(s). Visual appearance is subjective, and care should be taken to listen to the patient or parent’s observations.
CONTRAINDICATIONS
When a patient has a residual deviation after a strabismus procedure, or develops a new problem, there will be situations in which the surgeon will recognize the problem but advise the patient to delay correction or even to avoid additional operations. Contraindications to strabismus surgery may be absolute or relative.
Absolute contraindications include any procedure that carries a significant risk of loss of vision. For example, if there is a significant risk of anterior segment ischemia, or if ischemia occurred in the patient previously, and alterations in surgical technique will not reduce this risk, surgery is inadvisable. If correction of a problem requires surgery on the sound eye of a patient with monocular blindness, and the patient cannot accept the remote risk of loss of vision, surgery is contraindicated (Fig. 7). Reoperation should not be attempted in situations wherein the surgeon is unable to understand the causes of the motility problem or is unable to formulate a surgical plan that has a reasonable chance for successfully achieving the desired alignment. Surgical risks and morbidity are also probably not justifiable in some cases where the patient has a very limited life expectancy. As for any surgery, unacceptable anesthetic risk is a strict contraindication to reoperation.
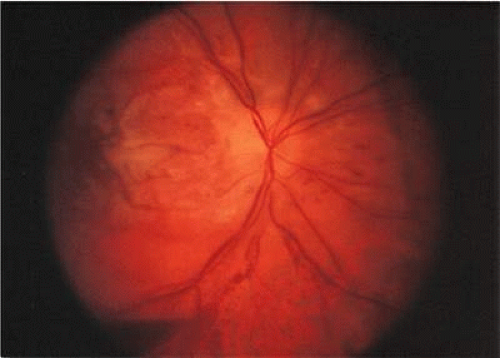 Fig. 7. Loss of vision after strabismus surgery is very uncommon. This 45-year-old woman had received orbital radiation prior to her strabismus surgery. The surgery was performed with retrobulbar anesthesia. Four days after the operation, vision was decreased from 20/20 to light perception. It is presumed that there was injection of the anesthetic into or around the optic nerve that caused compromise of the central retinal artery. The fundus photograph was taken 4 days after the procedure. |
Relative contraindications for surgery also exist. Early overcorrection of some forms of strabismus is not a reason for surgical reintervention. Examples of this include consecutive esodeviation after surgery for intermittent exotropia, where nonsurgical measures (e.g., prisms, occlusion, abduction exercises) and additional time will frequently lead to an acceptable result.8 Similarly, a muscle that has had a large recession may initially appear paretic. This muscle will usually “take up slack” over time and regain a more normal function. Reintervention should be delayed in conditions that are unstable or variable, or when adequate measurements cannot be obtained.
The surgeon should be cautious when the patient has unreasonable expectations regarding results after surgery. Helveston1 has stated that a patient needing a reoperation will have a 30% chance of needing another operation to obtain a satisfactory result. Refusal of the patient to accept the possibility of the need for further procedures or therapeutic measures is a relative contraindication to surgery.
PREOPERATIVE ASSESSMENT
Whenever possible, efforts should be made to obtain information from the patient’s history and from clinical records regarding the original diagnosis, preoperative measurements, and previous surgical procedures. In lieu of this information, some information can be obtained on examination. For example, slit lamp examination may disclose conjunctival scarring, which may suggest which muscles have had prior surgery (Fig. 8).
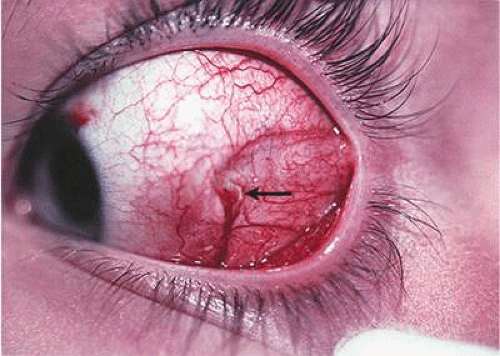 Fig. 8. Conjunctival scarring over the lateral rectus muscle and the history of correction of an exotropia suggest that the lateral rectus muscle had been recessed. |
Analysis of the patient’s sensorimotor development and consideration of factors such as identification of the preferred eye, evaluation of restriction, and the balance of force between the agonist/antagonist and yoke muscles will assist in developing a successful surgical strategy to correct the strabismus.1,2,4,5,9,10,11,12 The goal of evaluation of the sensory system is to determine the level of sensory fusion that can be expected when the deviation is corrected. The presence of fusional control may effectively reduce symptoms of diplopia in the presence of a small residual deviation. In some patients, postoperative diplopia can be predicted. Diplopia may be anticipated in patients who have had an overcorrection of longstanding intermittent exotropia.8,12 In patients who are visually mature (over 8 years of age), diplopia can be expected if an overcorrected eye position causes images to fall outside of a pre-existing suppression scotoma. Prisms may be used preoperatively to evaluate this possibility. Age of the patient, chronicity of the deviation, and etiology of the original strabismus problem are all factors that will help to predict those patients who will be at risk for diplopia. Tests of binocularity, such as the Worth four dot test and Bagolini lenses, and tests to measure stereoacuity will indicate the potential for binocular cooperation in patients with intermittent deviations. In general, young children with strabismus usually have an ability to develop suppression and secondary adaptations such as anomalous retinal correspondence. In adults with acquired deviations, there is usually an inability of the sensory system to develop suppression, resulting in diplopia. In some instances, such as in closed head injury, or in long-standing unilateral visual loss that is rehabilitated (e.g., cataract removal), there may be central disruption of fusion wherein seemingly perfect realignment of the visual axes results in constant diplopia that cannot be fused by the patient.13 Disturbing and persistent diplopia may occur in patients who have orthotropia on cover testing but also have macular heterotropia related to a retinal detachment procedure or to preretinal membranes that distort the normal relationship of the fovea to the peripheral retina.
When diplopia is present, it can be documented by performing binocular visual fields using a Goldmann perimeter (Fig. 9). This technique can be used before and after surgery to outline and quantitate the area of single binocular vision and diplopia.14,15 Binocular perimetry is also useful in explaining goals of surgery to the patient. For example, in patients who have a sixth cranial nerve palsy, it can be demonstrated that the area of single binocular vision will be shifted toward primary position, and that in eccentric gaze positions diplopia may persist.
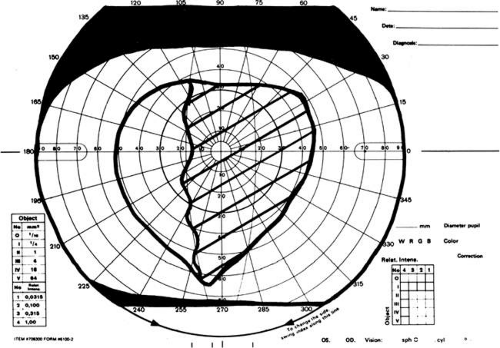 Fig. 9. Binocular perimetry on a patient with a right sixth cranial nerve palsy. Diplopia is present in the right field of vision. |
One of the most important components in assessing a patient’s oculomotor system is accurate measurement of the deviation. Meticulous prism and cover testing techniques should be done in the diagnostic positions of gaze. When gathering this information, one must ensure that refractive errors are corrected and that accommodation is controlled. If measurements are variable or tend to increase with prolonged prism and cover test, occlusion of the nondominant eye for a half hour will suspend fusion, and measurements obtained after this time will more accurately reflect the balance of forces influencing the ocular alignment. Another useful technique is the use of prisms using Halberg clips or in a trial frame. This can help determine whether the patient can fuse when the deviation is corrected optically and also can establish a “target angle” for surgical repair strategy.
Preoperatively, the surgeon should specifically evaluate for the presence of muscle paresis and restriction. These may be suggested by the presence of a primary and secondary deviation.16 The primary deviation refers to the size of deviation when the nonparetic (or nonrestricted) eye is forced to take up fixation. The secondary deviation, which is different in size from the primary, is measured with the paretic (or restricted) eye fixating. The secondary deviation tends to be larger because the abnormal eye is fixating “under duress” and by Hering’s law causes a larger degree of innervation to the yoke of a paretic muscle or the yoke of the antagonist of a restricted muscle. Limited ocular rotations and the presence of end-point nystagmus also occur in eyes in which there is paresis or restriction.
In the case of paretic and restricted muscles, there may also be a difference in the amount of deviation measured, depending on which eye is chosen for placement of the prism. If the prism is placed in front of the eye with the paretic or restricted muscle, it will tend to measure less than when the prism is placed over the nonparetic or nonrestricted eye.
Evaluation of saccadic eye movement will also help to differentiate restrictions from paresis. Paretic muscles will show decreased saccadic velocity, whereas eyes that have restriction will have normal saccadic movements until the leash effect of the restriction is encountered. Although this can be quantitated with electro-oculogram tracings, an experienced ophthalmologist can gain similar information through observation.
Paresis and restriction can usually be differentiated by forced duction testing. In cases where there is a paretic muscle, there will be absence of mechanical restriction on forced duction testing, and force generation testing will show reduced muscle strength. When forced duction testing is performed, it is important to make sure that the patient is relaxing the muscle being evaluated for mechanical restriction. The patient should be encouraged to look as far away as possible from the field of action of the muscle. If this is not done, the patient may “splint” or hold the eye in a position of fixation that will simulate mechanical restriction when in fact none is present.
The presence of ocular torsion may be evaluated subjectively (Maddox double rod test) and objectively (indirect ophthalmoscopy).17,18 The patient’s deviation should also be evaluated for distance-near disparity, wherein there is a significant difference in the size of the deviation at distance and near. Stability of a deviation can be ensured by comparing measurements of the deviation with measurements obtained on previous examinations. For patients who have ocular deviations that have variable measurements or some degree of ptosis, a Tensilon test should be considered to evaluate for ocular myasthenia.
If the clinical findings suggest a slipped muscle or the presence of a restrictive band, magnetic resonance imaging (MRI) of the orbit with coronal and sagittal cuts may be performed. The surgeon should review studies with a radiologist experienced with orbital pathology.
If nystagmus with a null point is present, a trial of prisms can be used to normalize the head position and to quantitate the amount of anomalous head turn correction needed. This may be done by holding loose prisms in front of the eyes or by using Fresnel prisms.
Ocular fixation preference may have significance regarding which eye and muscles should have surgery. If there is a strong fixation preference and the fixating eye is found to have a paretic muscle, causing a secondary deviation, the amount of surgery should be performed based on the amount of the secondary deviation, assuming that the primary problem of the paresis cannot be corrected or that the surgery is confined to the fellow nondominant eye.
The final step in assessment of the patient is selection of the anesthetic that is best suited for the patient and determination of whether there is an acceptable risk for using that anesthetic. Most reoperations require moderate to extensive tissue dissection, and this is expected to be painful. In these situations, a general anesthetic or a long-acting retrobulbar anesthetic should be considered.
If the use of adjustable sutures is contemplated, it is important to establish that the patient can cooperate for postoperative adjustment. This can be assessed by performing a forced duction test or a “cotton swab test” in the office prior to surgery. This test requires placement of a cotton swab on the conjunctiva of the topically anesthetized eye and movement of the eye. Patients who can tolerate this test are usually good candidates for an adjustable suture procedure.
It is important that the patient have realistic expectations about the anticipated surgery and that the surgeon and patient understand, and are in agreement with, the goals, risks, and anticipated outcome of the procedure. It is important to be aware of the level of frustration and perhaps anger that exists in patients who have had unsuccessful strabismus surgery.
PREOPERATIVE NONSURGICAL INTERVENTIONS
Before a strabismus reoperation is recommended, it is necessary to consider all practical nonsurgical measures that may correct the problem. Optical means should be tried to improve the focus of the retinal image. For small degrees of exotropia, minus lenses may be used to stimulate convergence. For esotropia, plus lenses can be used to relax accommodation. Similarly, in young children with undercorrected infantile esotropia, miotics such as echothiophate 0.125% (phospholine iodide) instilled daily may have some use in reducing accommodative convergence. Prisms can be used temporarily to restore single binocular vision and to promote fusion. As fusional control of a residual deviation improves, the power of the prism can be reduced or eliminated.
Ocular rotation exercises can be used to increase the field of action of a muscle whose antagonist is tight or inelastic after a large resection or advancement. For example, if a recess-resect procedure was used to correct an exodeviation and the medial rectus (resected muscle) is tight, abduction exercises may improve lateral movement of the eye. This combined with occlusion of the dominant eye and correction of any residual hyperopia may be especially useful in patients who show an overcorrection (consecutive esotropia) after surgery for intermittent exotropia.
In children younger than 8 years of age, recognition and treatment of amblyopia prior to surgery is generally indicated.
Reoperation is indicated when nonsurgical measurements have been tried and have failed to rectify the problem, or when nonsurgical measures are not realistically expected to be effective.
Once the decision is made to perform surgery, prisms should be removed from the patient’s optical correction prior to the procedure so that refractive errors can be corrected immediately after the procedure. Patients will benefit by prompt simultaneous stimulation of the fovea of each eye in the early postoperative period, a period when the fusion reflex will help to favorably prejudice the alignment so that the healing process will take place with the eye in optimal alignment.
NONINCISIONAL SURGICAL INTERVENTION (CHEMOSURGERY)
In selected patients, correction of the residual ocular misalignment may be achieved by injection of botulinum A toxin (Botox) into one or more extraocular muscles. This drug can be very useful in patients who refuse conventional incisional surgery or refuse to undergo general anesthesia. Treatment with botulinum A toxin is worthwhile in cooperative patients with small overcorrections or undercorrections (see elsewhere in these volumes). This potent neurotoxin is also used to augment transposition surgery for sixth cranial nerve palsy by injecting the toxin into the antagonist medial rectus muscle in conjunction with a transposition procedure.19,20 The effectiveness of botulinum toxin will depend on the dose of toxin, the administration technique, and the degree of function of the ipsilateral antagonistic muscle. The goal of treatment is to produce an overcorrection of the position of the eye in a direction that is away from the injected muscle. This is considered to be essential to produce the desirable changes in the antagonist muscle during the period of chemodenervation.
Botulinum A toxin is usually not useful for large-angle deviations or problems in which there is significant mechanical restriction.19
TIMING OF INTERVENTION
The timing of the reoperation will depend on the circumstances that were responsible for the initial failure. If the need for reoperation is obvious, such as a slipped or lost muscle, immediate intervention is appropriate. It is best to reoperate early, usually within days to 1 week, before the healing response is well established. When exploration is performed within a week of the original procedure, bleeding is reduced, tissue planes can still be identified, and the sutures in the muscle tendons are still present. The presence of a previously placed muscle suture will be of great assistance in helping to find a muscle that has slipped.
For situations in which there is a small but unacceptable undercorrection or overcorrection, or a new undesirable secondary problem is induced, such as hypertropia, or when the healing response may correct the problem, we advise waiting at least 6 to 8 weeks after the initial procedure before reintervention. Effects of the surgical trauma, such as inflammation, edema, suture dissolution, and tightness of a resected or tucked muscle, will have subsided. The optical distortion caused by tearing and changes in refractive error, as well as the patient’s discomfort, tend to improve during this period. This 6- to 8-week period also allows the surgeon an opportunity to use nonsurgical interventions to ameliorate the problem. In addition to these general recommendations, patient considerations such as diplopia, occupation, distance traveled, and vacations may enter into the decision for timing of the reoperations. In visually immature children, the goal of preserving binocularity or permitting binocularity to develop would arbitrate against excessive delay when an inadequate result from surgery is encountered.
In situations where botulinum A toxin has been used, it may be necessary to wait 3 to 4 months after an injection. This is the period of time necessary for a chemonervated muscle to recover its function. Complete recovery can be confirmed by comparing prism and cover measurements on sequential examinations.
ESOTROPIA
There are three acceptable methods to correct residual esotropia. The medial recti may be rerecessed,21,22,23 a medial rectus marginal myotomy may be combined with a resection of the lateral rectus, or both lateral recti may be resected.24,25,26,27 These procedures have similar success rates.24 If the medial recti are in a recessed position (i.e., near the arc of contact of the medial rectus with the globe), caution should be used in considering further recession. In such cases, resection of the lateral recti is the preferred procedure.26
Undercorrection of infantile esotropia occurs commonly. Increased amounts of medial rectus recessions have been advocated to improve the rate of undercorrection.28 If an esotropia greater than 15 Δ persists after 6 to 8 weeks, and it is not improved by alternate occlusion or correction of a hypermetropic refractive error, reoperation should be considered. Because the achievement of bifoveal fixation in infantile esotropia is unlikely,29 smaller deviations compatible with development of a monofixation syndrome30,31 or satisfactory cosmesis are acceptable results.
For older children with esotropia, indications for reoperation are the same as those used for the first procedure. For example, if surgery was recommended for a patient with nonaccommodative esotropia to eliminate a significant deviation, and this was not accomplished, then the same indication will apply for the reoperation. Success of the initial procedure has been improved by using prism adaptation in acquired esotropia and by using augmented amounts of surgery for this condition.32
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


