Blunt Trauma
Andrew Lam
William E. Benson
John B. Jeffers
This chapter concentrates on posterior segment injuries caused by blunt trauma. Anterior segment injuries, surgical management of penetrating injuries, sports injuries, and injuries in the workplace are covered elsewhere in the textbook.
EPIDEMIOLOGY
There are approximately 2.5 million new eye injuries in the United States each year.1 Males are more than four times more likely than females to have ocular injuries and young individuals are more likely than older ones. Blunt objects account for the largest percentage of eye injuries (30%), followed by sharp objects (18%), vehicle crashes (9%), gunshots, nails, BB guns (6% each), fireworks and falls (4% each).1,2,3 The most common objects to strike the eye are rocks, fists, baseballs, lumber, and fishing weights. In recent years, there has been greater awareness of injuries secondary to bungee cords, paintballs, and airbags.4,5,6,7,8,9 There are many other rare causes.10,11,12 Assault and motor vehicle injuries are usually the most severe and are the most likely to result in enucleation.13 The lifetime prevalence of ocular injuries is similar in black and white men, but black men are more likely to sustain a blinding injury.14
THE NECESSITY OF EYE PROTECTION
It is always sad when anyone loses vision from any cause. In the case of sports and occupational injuries, it is doubly sad, because many of them could have been prevented if appropriate, properly fitted, task-specific eye protection had been worn.15,16 Sports injuries account for approximately 100,000 eye injuries per year and approximately 10% to 40% of all eye injuries.17 They are so common because millions of Americans play sports but few wear the appropriate eye protection. The number of serious boxing injuries could probably be reduced if boxers wore proper head gear and thumb-tied gloves.18,19 Similarly, participants in other popular sports, such as squash and racquetball should wear appropriate eye protection.20,21 In Canada, a strict requirement for eye protection has almost totally eliminated blinding injuries in amateur ice hockey, racquetball, and squash players who wear appropriate equipment.22
EVALUATION
In every case of blunt trauma to the eye and orbit it is essential to perform a complete ophthalmic examination. One of the oddities of blunt trauma is that an injury that causes minimal signs of damage to one part of the eye can cause a significant injury in another part of the eye. For example, a blow to the eye can cause no iritis or hyphema while causing a giant tear, choroidal rupture, or blowout fracture. Only by ruling out all possible injuries can the examiner be confident that none are missed. The examiner should strongly consider an examination under anesthesia in uncooperative children suspected of being severely injured.
Immediate measurement of visual acuity is important for future decision making and for medico-legal and prognostic purposes. If a Snellen chart is not available, the ability to count fingers or to read a newspaper gives some indication of visual function. The examiner should document the size of the print and the distance at which it is read. A careful assessment of the pupils can be very helpful, because an afferent pupillary defect (APD) is an important predictor of visual outcome.23 In many cases sphincter tears or iritis make this difficult, but the examiner can detect severe retinal or optic nerve damage by using the swinging flashlight test to demonstrate an APD. The pupil in the fellow eye constricts when the light is moved to it from the traumatized one.
It is especially important to rule out retinal tears, commotio retinae, choroidal ruptures, and optic nerve involvement. If hyphema is present, however, the fundus examination must be done very gently to avoid precipitating a secondary hemorrhage. Scleral depression and gonioscopy should be avoided for at least 2 to 3 weeks. If a complete fundus examination is difficult because of opaque media, ultrasonography should be repeated every 2 to 3 weeks until it is certain that there is no retinal detachment. All patients must be followed until the ora serrata can be seen for 360 degrees.
One further admonition is in order. The examiner must examine the uninjured eye as well. Patients who suffer blunt trauma in one eye may well have suffered previous blunt trauma in the fellow eye and may be unaware of vision-threatening conditions such as glaucoma or retinal detachment.
MECHANISMS OF OCULAR DAMAGE
Blunt trauma causes ocular damage by the coup mechanism, by the contrecoup mechanism, or by ocular compression.
COUP AND CONTRECOUP
Courville24,25 introduced the concept of coup and contrecoup injury to explain brain damage caused by blunt trauma to the head. Coup refers to local trauma at the site of impact. Contrecoup refers to injuries at the opposite side of the skull caused by shock waves that traverse the brain. Foci of brain damage are found along the path of the shock waves, especially at interfaces of tissues of different density. The greatest difference in density is between the brain and the skull, and it is here that the most severe damage occurs. Wolter later used these concepts to explain eye injuries.26 Examples of coup injuries are corneal abrasions, subconjunctival hemorrhages, choroidal hemorrhages, and retinal necrosis (Fig. 1). The best example of a contrecoup injury is commotio retinae (Fig. 2). These injuries are discussed later in this chapter.
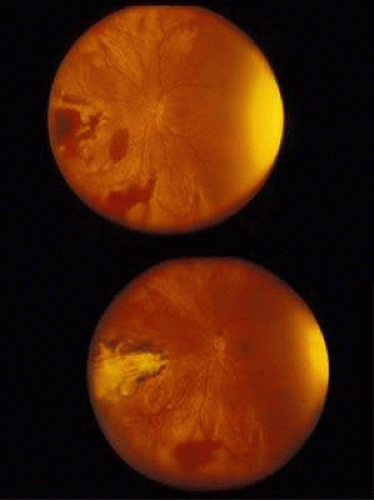 FIG. 1. A: Coup injury. At the site of impact of a stick, subretinal and vitreous hemorrhage are present. B: Three months later, most of the hemorrhage has cleared, revealing choroidal and pigment epithelial necrosis. |
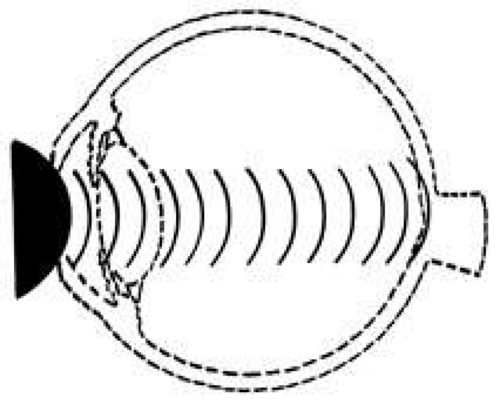 FIG. 2. Contrecoup injury. When a blunt object strikes the eye, shock waves traverse the eye to strike the posterior pole. |
ANTERIOR–POSTERIOR COMPRESSION AND EQUATORIAL EXPANSION
The volume of a closed space cannot be changed. Therefore, when the eye is compressed along its anterior–posterior axis, it must either expand in its equatorial plane (Fig. 3) or rupture. Using high-speed photography, Delori and associates27 studied blunt trauma in enucleated pig eyes. The cornea was indented 8.5 mm, reducing the original anterior–posterior axis by 41% and bringing the posterior surface of the cornea into contact with the iris and the lens. The equatorial plane was expanded to 128% of its original length. Specific examples of damage caused by this severe stretching of the ocular tissues are discussed later.
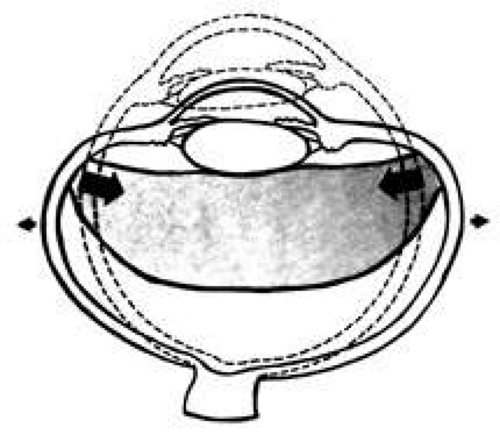 FIG. 3. When the eye is compressed along its anterior-posterior axis, it expands in its equatorial plane (small arrows), causing severe traction at the vitreous base (large arrows). |
ANTERIOR SEGMENT INJURIES
CORNEA
Abrasions of the corneal epithelium are common but because they heal rapidly, they are of little consequence. Endothelial damage can be more serious. A local concussion (coup effect) can rupture endothelial cells and loosen the intercellular tight junctions. They can also be damaged by being crushed against the iris and the lens. The transient corneal edema usually clears, but endothelial damage can be permanent. Follow-up studies of patients with traumatic hyphema show endothelial cell loss that correlates with the severity of the initial injury.28,29
When a total hyphema is present, the damaged corneal endothelium may permit hemoglobin to enter the corneal stroma. Usually, high intraocular pressure is required to cause corneal bloodstaining, but cases have been reported in which the intraocular pressure was normal.30 Corneal transplantation is rarely necessary as the bloodstaining nearly always clears spontaneously, but this may require a considerable period of time. The central cornea clears last. Adults can wait for clearing, but in young children, amblyopia can develop.
When the cornea is abruptly forced backward by severe blunt trauma, it presses the iris against the lens, preventing the escape of aqueous into the posterior chamber. If enough force is applied, the entrapped aqueous dissects into the ciliary body, resulting in a recessed angle (Fig. 4). This tearing of the ciliary body is responsible for approximately 90% of the hyphemas seen after blunt trauma.31,32 Other causes of hemorrhage include separation of the iris from the ciliary body (iridodialysis) and sphincter tears. Ultrasound biomicroscopy can be useful in diagnosing dissection of the ciliary body or iridodialysis (Fig. 5).33,34,35
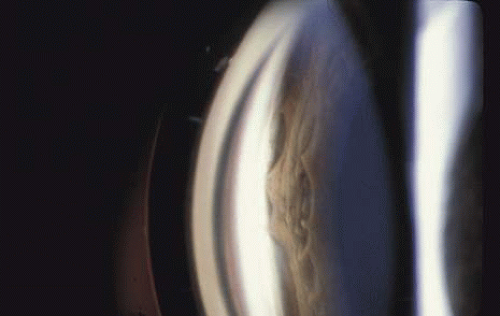 FIG. 4. Angle recession after blunt trauma. |
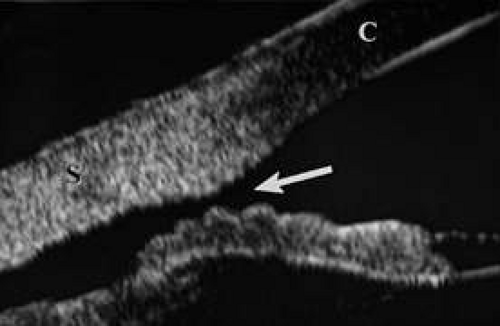 FIG. 5. Ultrasound biomicroscopy image of cyclodialysis (arrow). “C” identifies the cornea, “S” identifies the sclera. |
GLAUCOMA
Acutely, the intraocular pressure may be normal, increased, or decreased. Aqueous outflow may be decreased because of angle recession, inflammatory trabeculitis, or hyphema. On the other hand, ciliary body injury tends to decrease aqueous inflow. The intraocular pressure depends on the balance of these factors. In patients who have large hyphemas, the pressure may rise abruptly. Therefore, it must be checked at regular intervals. It is especially important to monitor the intraocular pressure in hyphema patients who have sickle cell disease, be it homozygous or heterozygous. Unlike normal erythrocytes, sickled erythrocytes cannot pass through the trabecular meshwork and tend to occlude it, raising intraocular pressure. This, in turn, can cause central retinal artery obstruction even if the pressure is only in the high twenties or low thirties. Prompt paracentesis followed by surgical evacuation can restore vision.39
Late glaucoma can also develop, even years after the initial injury. Autopsy studies have found three ways by which the trabecular meshwork can be obstructed: proliferation of corneal endothelial cells and Descemet’s membrane, proliferation of fibroblasts, and peripheral anterior synechiae (presumably from inflammation or from organization of blood in the angle for more than 7 days).40 Other possibilities are direct damage to the trabecular meshwork and damage to the ciliary muscle with reduced traction on the scleral spur. The risk is greatest in patients who have severe anterior segment damage such as cataract, angle recession, iris damage and displacement of the lens.41 Nine percent of patients with angle recession develop permanent glaucoma.42 If trabeculectomy is required, some authors recommend antimetabolites because the failure rate in patients with angle recession is greater than it is in patients with typical open angle glaucoma.43
LENS
When the lens is struck by the cornea or by a strong shock wave, a transient anterior subcapsular cataract, known as a rosette cataract, may develop (Fig. 6). Repeated trauma, as in boxers, often causes posterior subcapsular cataract. Blunt trauma can also result in rupture of the anterior or posterior capsule.44,45 In severe cases, iridodonesis or a bead of vitreous in the anterior chamber signals a subluxed lens. Dislocation may also occur (Fig. 7). It is important to remember that ocular trauma is common, but lens dislocation is rare. Therefore, in patients with a dislocated lens, the clinician should always rule out predisposing causes such as Marfan’s syndrome, homocystinuria and syphilis. In rare cases the lens itself can rupture and cause phacolytic glaucoma.
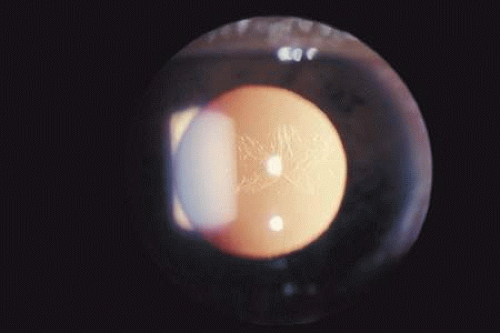 FIG. 6. An anterior subcapsular rosette cataract. |
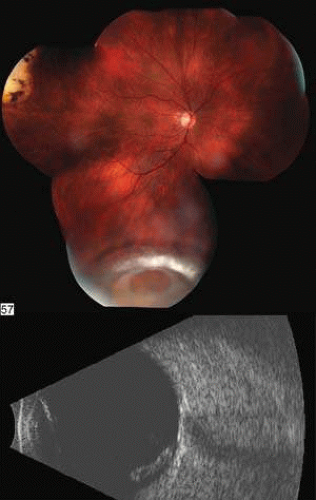 FIG. 7. A: Posterior dislocation of an intraocular lens. B: B-scan of intraocular lens lying on the retina inferiorly. |
UVEA
Blunt trauma can lead to persistent uveitis. If traumatic uveitis is suspected, the ophthalmologist must carefully examine the fundus for posterior signs of trauma.48
HYPHEMA
The management of traumatic hyphema remains somewhat controversial. The goals are to prevent peripheral anterior synechiae, severe acute glaucoma, and corneal blood staining. Although these can be the result of the initial hyphema, the risk increases dramatically with secondary hemorrhage which is most likely to occur 1 to 2 days after the injury. The risk is greatest in patients who present with large hyphemas and in African Americans, particularly if there is a history of sickle cell disease.49 The reported incidence of secondary hemorrhage ranges from 0% to 38%.39
Medical Management
Currently, at the Wills Eye Hospital, most microhyphemas and many hyphemas are treated on an outpatient basis. It is appropriate to consider hospitalization for patients who are noncompliant, are at high risk of rebleeding, or have other severe injuries. Hospitalization can also be considered for children if child abuse is suspected or aggressive treatment is advised to prevent amblyopia. If treated as an outpatient, hyphema patients follow-up daily for 3 days. Microhyphema patients follow-up on the third day after initial trauma.50,51
The authors have long abandoned traditional strict bed rest but still encourage limited activity. The head of the bed should be elevated to encourage the blood to collect inferiorly, out of the visual axis. Eye-patching is avoided so that patients can immediately report decreased vision, which is often the first symptom of a secondary hemorrhage. The eye is protected with an eye shield.
The authors dilate the pupil with atropine to reduce pain and to facilitate later fundus examination. Atropine may also reduce the risk of secondary hemorrhage by stabilizing the blood–ocular barrier. Topical corticosteroids are used to increase comfort and decrease inflammation.52,53,54 It has been reported that systemic corticosteroids markedly reduce the incidence of secondary hemorrhages,52,53,54 but two prospective double-blind studies found no beneficial effects.55,56
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


