CHAPTER 105 Reconstruction of the Hypopharynx and Esophagus
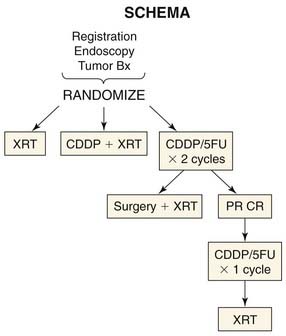
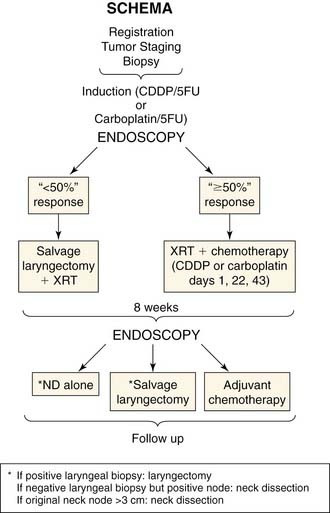
Many technical advances in conservation surgery of the larynx and pharynx have occurred, and new treatment protocols for organ preservation with chemotherapy and radiation have developed. Current management of advanced-stage laryngopharyngeal and esophageal cancers generally involves multiple modalities to optimize outcomes. At present, there is a trend toward reserving surgery as a salvage procedure after failure of other modalities for advanced laryngeal and hypopharyngeal cancers (Fig. 105-1).1–5 The adverse effects of radiation therapy on wound healing have been well documented.6 Salvage surgery in patients exposed to previous radiotherapy and/or chemotherapy is associated with a higher incidence of wound complications, with overall complication rates ranging from 37% to 100%.7 For example, postoperative salivary fistula rates as high as 50% have been reported after surgical salvage for persistent disease after chemoradiation therapy.8 Therefore prior treatment must be taken into consideration when choosing a reconstructive method for patients who undergo salvage surgery. Given the high complication rate with surgical salvage, treatment selection may be a better choice to reduce the incidence of surgical complications.9 Treatment selection makes use of induction chemotherapy to determine the responsiveness of a tumor. If the tumor responds (shrinks) by more than 50% to one or two doses of chemotherapy, then the patient undergoes chemoradiation therapy. If the tumor does not respond, the patient undergoes surgery followed by radiation therapy (Fig. 105-2). The possible advantage of treatment section is customization of therapy and avoidance of surgical salvage with its attendant complications. Reconstruction of the hypopharynx and esophagus is largely being shaped by the current trend toward primary concurrent chemoradiation therapy. The surgeon is most commonly involved in salvage of treatment failure, which is resulting in new approaches that attempt to reduce complications and improve function in this compromised patient group.
Patient Population at Presentation
Most patients who require reconstruction of the hypopharynx and esophagus harbor a malignancy at those sites. At the University of Michigan, patients present for reconstruction of their hypopharynx or cervical esophagus after failure of chemoradiation for advanced-stage squamous cell carcinoma of the larynx, pharynx, or trachea. Primary resection is reserved for patients who present with laryngeal cartilage invasion or those who do not respond to induction chemotherapy. Patients who undergo surgical resection and pharyngeal reconstruction have the highest postsurgical complication rate when compared with any other site in the upper aerodigestive tract.10 Carcinomas of the larynx tend to be less aggressive than carcinomas of the hypopharynx. Hypopharyngeal carcinomas are known to demonstrate aggressive behavior, with a high incidence of submucosal spread, satellite lesions, and subsequent invasion of adjacent structures. Careful assessment of the lungs is also important. A solitary focus of disease in the lung can be resected, but more extensive metastatic disease or mediastinal disease would make the patient incurable and a palliative approach would be taken. This patient population has a high prevalence of tobacco and alcohol abuse and often has related comorbidities such as cardiovascular disease, hypertension, chronic obstructive pulmonary disease, peripheral vascular disease, and nutritional deficiency. Because of these underlying comorbidities and the disease process, treatment of this patient population is more difficult. Trauma from explosive devices or accidents, previous radiation or chemoradiation resulting in stenosis, or chemicals (e.g., lye ingestion injury) is another possible cause for reconstruction of the hypopharynx and esophagus.
Perioperative Counseling
Nursing, social work, speech pathology, dentistry, cessation counseling, nutrition, and appointment scheduling are all part of the pretreatment workup. Because of the many disciplines involved, the treatment and rehabilitation experience can be bewildering for the patient. This has put the nurse clinical coordinator at the core of the patient care experience. It is not uncommon for these patients to have a poor predisease diet that, when coupled with a painful obstructive disease process involving the upper aerodigestive tract, can lead to significant malnutrition. Preoperative counseling with the speech pathologist is an essential part of patient education and shaping expectations. The speech pathologist is often regarded by the patient as the individual who will restore function post treatment. The greatest counseling challenge in this patient group is overcoming poor coping skills.11 The speech pathologist must contend with the patient’s coping mechanisms in order to assist rehabilitation. Psychosocial counseling, which speech pathologists often do on an “ad hoc” basis, has been shown to benefit head and neck cancer patients when compared with controls.12 The speech pathologist must describe the expected long-term functional outcomes, identify the communicative and swallowing strategies that will be necessary, and indicate his or her interest in supporting the patient throughout treatment and rehabilitation. An addicted patient is unlikely to be effectively rehabilitated. Smoking is highly correlated with alcohol intake and depression. Smoking cessation interventions, particularly those that take into consideration alcohol intake and depression, have been shown to be efficacious for this patient population.13 The patient must understand that continuation of addictive behaviors represents the greatest risk to survival and future functioning. It is important to emphasize that there are many different ways to quit smoking, that alcohol is a facilitator, and that nicotine is not a carcinogen. Use of patient volunteers who have completed treatment are an important resource. They provide education and experience with regard to post-treatment recuperation and long-term quality of life to patients who are preparing for treatment.
Preoperative Evaluation
A thorough preoperative evaluation including endoscopy and radiographic studies must be performed to assess the extent of the primary tumor and to detect the presence of regional or distant metastasis. Particular attention must be given to a complete esophagoscopy. The degree of involvement of the cervical esophagus should be assessed carefully, keeping in mind the propensity for submucosal spread and skip lesions. The presence of a tumor in the esophagus must be ruled out because it may necessitate a total esophagectomy. It is generally not possible to preserve the larynx with advanced lesions, although laryngeal-sparing surgery may be an option for a select few patients. Partial laryngeal procedures and the associated reconstructive approaches are discussed in another chapter. The ideal margin for hypopharyngeal lesions is still controversial. Some authors advocate distal margins of up to 3 to 6 cm as long as there is no evidence of disease in the remaining esophagus.14–17 Although routine total esophagectomy had been recommended in the past for management of carcinoma involving the hypopharynx, this approach is no longer the standard of care.18 The esophagus is removed only for adequate margin or direct involvement. If the patient has been previously treated with chemotherapy and radiation therapy, the quality of the cervical skin can be poor. The skin may need to be replaced as part of the reconstructive procedure. It is also important to assess thyroid function preoperatively because the patient can be hypothyroid due to prior radiation. Hypothyroidism causes delayed healing and contributes to postoperative wound complications.
Defect Classification
Pharyngoesophageal defects are classified according to the amount of pharyngeal (partial, near total, and total), oropharyngeal (base of tongue, lateral pharyngeal wall, posterior pharyngeal wall, soft palate), esophageal, and skin involvement. Partial pharyngeal defects are those arising from the extirpation of a larynx that may include some pharyngeal mucosa and can be closed primarily without stenosis or require a small graft to reconstruct less than 50% of the circumference of the pharynx. Near-total pharyngeal defects are defects in which only a thin strip of pharynx (≈1 cm) remains and requires a graft to reconstruct more than 50% of the circumference of the pharynx. Total pharyngeal defects are those in which there is complete absence of a segment of the pharynx. For the purposes of this chapter, we do not discuss partial laryngeal defects or reconstruction of hypopharyngeal defects with an intact larynx because this topic is covered elsewhere. Anecdotally, there have been numerous attempts to reconstruct hypopharyngeal defects with an intact larynx. Interestingly, there are no published case series. Drawing from the author’s experience and discussions with colleagues, there does not seem to be a reliable and reproducible technique. This reconstructive issue needs more investigation. Defects that extend into the oropharynx may need additional reconstructive planning. Particularly those defects that involve the soft palate will require a pharyngoplasty and additional tissue to resurface the palate and tonsil.19 Defects of the tonsil can generally be closed primarily. Associated defects of the tongue base can be partial or total. Partial defects that involve up to 50% of the tongue base do not require reconstruction. Primary closure of these defects is achieved by advancing the tongue base across the defect and suturing it to the resected edge of the oropharynx. This approach results in a sensate, functional tongue base reconstruction. Defects of the entire tongue base are more concerning and may require reconstruction with a graft, particularly if the patient has a near total or total pharyngeal defect and is post chemoradiation therapy. Although it has been suggested that patients who have undergone hemilaryngectomy do not require reconstruction of the base of the tongue, loss of the entire tongue base diminishes the ability of the patient to propel the bolus through the pharyngeal segment and can limit dietary intake to thin liquids. If the resection of the pharynx extends into the mediastinum and a reliable distal anatomosis cannot be sutured, then a visceral transposition is the reconstruction of choice. For a visceral transposition, the patient will undergo a complete esophagectomy, dissection of the mediastinum, and an open abdominal approach. The cervical skin needs to be assessed for tumor involvement and viability. A cervical skin defect in combination with a pharyngeal defect significantly affects reconstructive decision making.
Reconstructive Decision Making
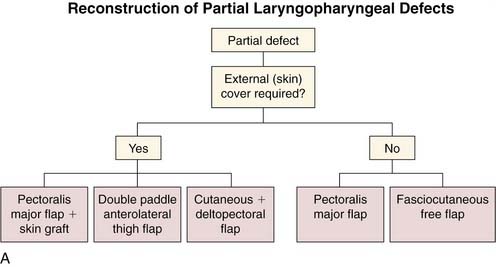
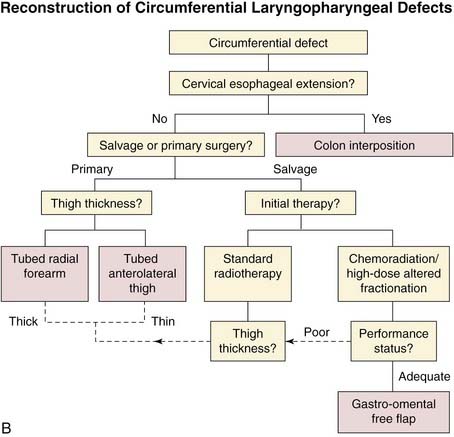
Reconstruction of the hypopharynx and cervical esophagus is associated with a high risk of morbidity and mortality. A wound at this site can expose the carotid and internal jugular vein, which can lead to life-threatening hemorrhages. Wound breakdown of the common wall between the trachea and esophagus usually results in aspiration pneumonia and is associated with a high mortality rate. Hypopharyngeal reconstruction should be designed to make a wound safe and provide a pharyngeal conduit that assists swallowing and speech. If the only priority of the reconstructive surgeon was a safe wound, then exteriorization of the upper aerodigestive tract with a pharyngostome, esophagostome, and tracheostome would ameliorate nearly all of the associated wound complications. The patient is interested in more than a safe wound and wants to return to pretreatment levels of social interaction and occupation. For this reason, reconstructive surgeons reconstruct the pharynx despite the attendant risk and measurable mortality. Fortunately, there are many reconstructive options for hypopharyngeal reconstruction (Fig. 105-3A and B). These options include local and regional cervical skin flaps, deltopectoral flap, pectoralis flap, latissimus flap, gastric transposition, colonic interposition, revascularized fascial flaps, and the gastro-omental flap. The following factors must be considered when choosing a reconstructive option:
Local and Regional Skin Flaps
From 1877 through 1904 Czerny, Mikulicz, and Trotter22,23,24 described the first techniques to restore continuity to the pharynx. These procedures were multiple-stage procedures that used cervical skin flaps for reconstruction. In the 1940s Wookey improved on these techniques when he used a two-stage repair for pharyngoesophageal defects with a laterally based rectangular cervical flap. In the first stage the cervical skin was redraped over the prevertebral fascia and was interposed between the pharyngeal and cervical esophageal stomas to create the posterior wall of the pharyngeal reconstruction.25,26 The approach exteriorized salivary and gastric secretion, protected the vascular sheath, and controlled infection. The continuity of the pharynx and cervical esophagus was returned at a second stage, usually 2 or 3 months later. Rectangular skin flaps with a base along the reconstructed posterior pharyngeal wall were fashioned from the cervical skin, on the right and left sides. These flaps were tubed and closed vertically in the midline to create a skin-lined pharyngoesophageal segment. A skin graft was placed on the reconstructed pharynx and the donor sites of the rotated cervical flaps. All these methods that used local skin flaps required multiple steps and were associated with a high frequency of complications. Although this approach created a safe wound, the functional outcomes of speech and swallowing were compromised because of the difficulty of reconstructing a pharynx that would not fistulize or stenose. The use of radiation increases the complication rate of this reconstructive approach. Although it is important to be aware of this approach, it is largely of historical interest. The concept of a two-layer closure, one for the pharynx and one for neck cervical skin, using local flaps for mature pharyngocutaneous fistula has its conceptual roots in this approach. To improve the success rate of pharyngeal closure, nonradiated tissue with an axial blood supply was necessary.
The description of the deltopectoral flap by Bakamjian in 1965 represented a significant advance over previous methods.27 Unlike local flaps that rely on a random blood supply, this regional chest skin flap is based on a more reliable axial-pattern blood supply through the perforating branches of the internal mammary artery. It provides well-vascularized tissue from a donor site that lies outside of the typical radiation fields used for head and neck cancer. The deltopectoral flap has a consistent vascular supply and can be reliably used without the need for surgical delay of the flap if limited to the area medial to the deltopectoral groove. This donor site continues to evolve. New approaches involve mobilizing the internal mammary artery by removing the costochondral junction to improve the mobility and transposability of the flap.
Like the Wookey approach, the deltopectoral flap is a multistage procedure requiring the initial creation of a controlled fistula. In the case of the deltopectoral flap, it is used to form the pharyngeal tube and the cervical skin is draped over the deltopectoral inset. At the first stage, a medially based skin flap is elevated and tubed to the superior cut edge of the pharyngeal resection. The posterior wall of the inferior cut edge was sutured to the deltopectoral flap, and a controlled fistula was fashioned with the anterior wall of the inferior edge of pharyngeal resection. The flap pedicle was divided at least 6 weeks later, along with closure of the fistula and skin grafting to the donor site. The deltopectoral flap was an improvement, but there remained an unacceptably high rate of fistula formation, flap necrosis, and stenosis. Given these limitations, this approach is not commonly used, although these techniques may still occasionally be useful in certain patients who have failed or are unable to undergo alternative reconstructive approaches. At present, this donor site is most commonly used for the closure of a fistula after hypopharyngeal reconstruction (Fig. 105-4).

Myocutaneous Flaps
The primary use of the myocutaneous flap is for reconstruction of partial pharyngoesophageal defects. A strip of pharyngeal mucosa is left so that a complete tubing of the myocutaneous flap may be avoided.28 However, it may be the only option for patients with poor cardiopulmonary status who cannot tolerate prolonged surgery or the combined violation of thoracic and abdominal cavities. It is also a good option for those who do not have suitable recipient vessels for free tissue transfer because of previous radical surgery. The pectoralis flap may be most useful as a salvage flap for extra soft tissue, for carotid protection as a myofascial flap, or as a reinforcing layer in previously irradiated patients to minimize the chance of fistula formation.29 Voice can be successfully restored in patients reconstructed with pectoralis myocutaneous flaps.30
Many modifications have been proposed to maximize the usefulness of the pectoralis myocutaneous flap for near total or total pharyngoesophageal reconstruction. Due to newer reconstructive techniques, these modifications have less clinical utility. However, they are important to know as alternatives to conventional reconstructive approaches. These modifications include harvest of the flap as a myofascial flap, thereby avoiding the often excessively bulky subcutaneous tissue that makes tubing of the myocutaneous flap difficult. The difficulty with this approach is stenosis. To our knowledge this approach is no longer used. Alternately, the pectoralis flap can be partially tubed 270 degrees around and closed to prevertebral fascia that has been grafted.31 When the pectoralis flap is used for reconstruction of circumferential defects, it is associated with stricture formation at the distal anatomosis. Stricture formation after pharyngoesophageal reconstruction with the pectoralis flap has been reported in 35% of patients.
Some surgeons have suggested that a disadvantage of myocutaneous flaps is a relatively high rate of fistula formation. Fistula formation in hypopharyngeal reconstruction is more likely to be related to the history of prior chemoradiation therapy or use of the myocutaneous flap in a defect that is too large for the primary angiosome. Myocutaneous flaps are ideal for defects limited to the hypopharynx. It can also be useful if there is a combined cervical defect because the muscle can be skin grafted to resurface the cervical skin and the cutaneous portion of the flap can be used to resurface the hypopharynx.32 The pectoralis flap is also useful in chemoradiation patients for the reinforcement of the primary closure to reduce fistula formation. A pectoralis flap is often inadequate at closing a defect extending into the superior-lateral oropharynx or nasopharynx. Other potential disadvantages of the pectoralis flap include the risk of shoulder dysfunction, particularly in patients who have undergone neck dissection.
Gastric Transposition
In 1960 Ong and Lee33 were the first to describe gastric transposition with pharyngogastric reconstruction. They used a transthoracic approach for the single-stage reconstruction after pharyngoesophagectomy. At present, the “gastric pull-up” technique is performed without thoracotomy in favor of blunt esophageal dissection to reduce the high morbidity and mortality associated with simultaneous violation of the thorax and abdomen.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


