CHAPTER 51 Primary Sinus Surgery
The maxillary sinus has been the focus of surgical attention since the 17th century. An approach through the anterior maxillary wall was described as early as 1675 by Molinetti.1 Other methods were also described, but none of these was satisfactory until Caldwell, Spicer, and Luc added a counter-opening into the nose in the 1890s.1,2 The Caldwell-Luc procedure remained popular as the primary choice of treatment in chronic rhinosinusitis (CRS) through the early 20th century. Although Hirschmann conducted the first endoscopic examination of the nose with a modified cystoscope in 1901,3 the modern era of endoscopic sinus surgery (ESS) evolved with the development of Hopkins rods in the 1950s. Messerklinger5 pioneered the study of the endoscopic anatomy and pathophysiology of the paranasal sinuses, publishing his experience with ESS in 1978.4,6 He highlighted the role of the ostiomeatal complex (OMC) in the pathophysiology of rhinosinusitis and directed attention to it during surgery. His resident, Stammberger,4,6–10 was instrumental in popularizing this technique outside Germany and Austria.3 Kennedy7 is credited with the introduction of ESS to the United States in 1985.3 Primary surgery for CRS is now performed almost exclusively endoscopically. Endoscopic approaches also now dominate the surgical treatment of many other sinonasal disorders. Understanding of the anatomy and pathophysiology of each disease process is necessary before one can embark on surgery.
Anatomy
Identification of anatomic landmarks and recognition of variations are imperative to maximize the benefit and limit the complications of ESS.11 This chapter offers a concise review of the relevant anatomy. Although this review focuses on the endoscopic anatomy, the surgeon must be familiar with external landmarks and the three-dimensional orientation. Standardized nomenclature based on the recommendations of the Anatomic Terminology Group at the International Conference on Sinus Disease is used in this chapter.12
Ostiomeatal Complex
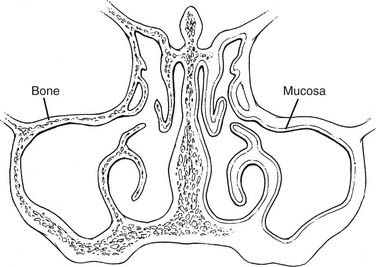
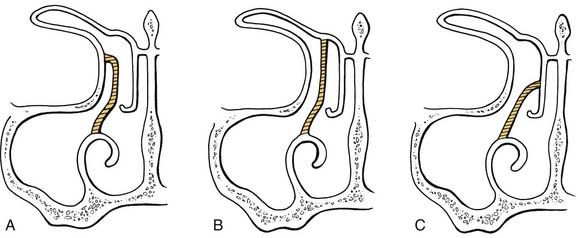
The OMC is a functional entity of the anterior ethmoidal complex representing the final common pathway for drainage and ventilation of the ethmoid, maxillary, and frontal sinuses. Its exact boundaries are not defined. It comprises the uncinate process, the ethmoid infundibulum, anterior ethmoid cells, and the ostia of the anterior ethmoid, maxillary and frontal sinuses (Fig. 51-1). The uncinate process lies in the sagittal plane and runs from anterior-superior to postero-inferior. Laterally, the uncinate process covers the infundibulum, which is the three-dimensional space where the anterior sinuses drain. The hiatus semilunaris inferior, commonly referred to as the hiatus semilunaris, is a two-dimensional space between the uncinate process and the ethmoid bulla. Superiorly, the uncinate process may attach either to the lamina papyracea, the skull base, or the middle turbinate (Fig. 51-2).11 Because this attachment causes variations in frontal sinus drainage, its preoperative identification is important.
Maxillary Sinus
The natural ostium of the maxillary sinus drains into the infundibulum and is found just below the orbital floor in the medial wall of the sinus. It usually lies halfway between the anterior and posterior walls.13 It is located in the superior third of the infundibulum in 10%, the middle third in 25%, and the inferior third in 65% of cases.14 The natural ostium is elliptical; accessory ostia are round and are present in 10% of patients.13
Sphenoid Sinus
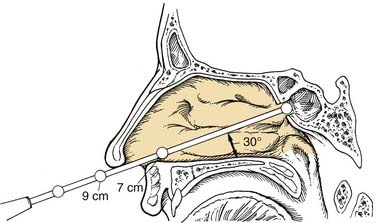
The sphenoid sinus is the most posterior paranasal sinus. Its natural ostium opens into the sphenoethmoid recess. This recess lies posterior to the superior turbinate, and anterior to the anterior wall of the sphenoid. The sphenoid ostium is located approximately halfway up the anterior wall of the sinus. It is medial to the posterior end of the superior turbinate in 83% of cases.15 The ostium lies at a distance of 6.2 to 8.0 cm (average, 7.1 cm) from the nasal spine, at an angle of 30 to 34 degrees with the floor (Fig. 51-3).15–18 The surgeon must identify the natural ostium to safely enter this sinus. The sphenoid is surrounded by several critical structures, such as the ICA, the optic nerve, and the skull base. Septations in the sphenoid frequently have attachments to the ICA.
Frontal Sinus
The frontal sinus drains into the middle meatus through the frontal recess. The frontal recess is located at the junction of the frontal sinus and the most anterosuperior part of the ethmoid sinus. The medial wall of the frontal recess is made by the anterior-most part of the middle turbinate, and its lateral wall is the lamina papyracea.12 The anterior wall of the frontal recess is the posterior wall of the agger nasi cell. The recess is hourglass shaped, with the narrowest part at the frontal ostium. The ostium of the frontal sinus can drain anterior to the uncinate process or, more commonly, posterior to the uncinate process, usually in the ethmoid infundibulum.19 The frontal or frontoethmoid cells lie superior to the agger nasi cells and can show variable pneumatization. Kuhn20 identified the following four pneumatization patterns:
Cells posterior to the frontal sinus, pneumatizing superior to the orbit, are termed supraorbital ethmoid cells.20
Anterior Skull Base
The anterior skull base is formed by the cribriform plate medially. The fovea ethmoidalis extends laterally from the cribriform plate to form the roof of the ethmoid sinuses. The fovea ethmoidalis may lie higher than the cribriform plate. The lateral lamella of the cribriform plate joins the fovea ethmoidalis and is considerably thinner than the lateral part of the ethmoid roof. Keros21 classified the skull base into three types according to the depth of the olfactory groove: type 1, 1 to 3 mm; type 2, 4 to 7 mm; and type 3, 8 to 16 mm. Because the lateral lamella forms most of the steeply inclined ethmoid roof in a type 3 configuration, patients with this configuration are especially vulnerable to penetration of the anterior skull base during ESS. The anterior skull base is highest anteriorly and slopes downwards posteriorly.22 This fact is important to remember during opening of the sphenoid sinus through the posterior ethmoids. Dissection must be directed inferiorly and medially.
Anatomic Variations
Anatomic variations include structures such as a concha bullosa, agger nasi cells, infraorbital (Haller) cells, sphenoethmoid (Onodi) cells, and paradoxic middle turbinates. Concha bullosa is the term used for an aerated middle turbinate or a cell found within the middle turbinate. These structures appear as a widened area of the middle turbinate, and they may obstruct the OMC. In the absence of a history of sinusitis, the incidental finding of widened middle turbinate during endoscopy or concha bullosa on CT does not mandate further investigation.23 Most patients with such variations remain asymptomatic. In a review of 172 coronal sinus CT scans, a concha bullosa was found in 28% of patients with sinus disease and in 26% of patients without sinus disease.24
Indications for Primary Sinus Surgery
As with the indications, there is no absolute contraindication to using the endoscopic approach. The decision to use an external or an endoscopic approach depends on the amount of exposure needed as well as the surgeon’s training and experience. Box 51-1 lists the sinonasal disease processes for which surgery is indicated. In the past, most of these processes have been treated with an external approach, but ESS is increasingly being used for them.
Recurrent Acute Rhinosinusitis
Surgery is indicated for patients with four or more episodes of acute rhinosinusitis annually that are refractory to medical therapy.25 Disease must be documented endoscopically or on CT scan while the patient is symptomatic before any surgical intervention is undertaken.
Acute Complications of Rhinosinusitis
Acute complications, both orbital and intracranial, that are unresponsive to medical therapy require immediate surgical intervention. Traditionally, external procedures have been used because nasal edema and inflammation can compromise endoscopic exposure. However, in experienced hands, ESS is safe and effective.26
Mucoceles
Mucoceles are epithelium-lined, mucus-containing sacs that completely fill a paranasal sinus. They are expansile and cause bony erosion. They must be removed or drained to prevent intracranial and orbital complications. Mucoceles are more commonly found in the frontal and ethmoidal sinuses, although isolated sphenoid mucoceles have been reported.27,28 In the past, open approaches have been used to completely remove the lining of the mucocele. However, this practice can be dangerous because mucoceles can erode through the skull base or through the lamina papyracea into the orbit. Endoscopic management with marsupialization is safe in this situation, because complete removal of the cyst lining is not required. Although technically more challenging, this latter approach is very effective, with recurrence rates near 0%.29 A review of 108 mucoceles managed endoscopically found that 60 mucoceles had eroded the skull base, and 31 had significant intracranial extension.29 This review reported one recurrence and one postoperative CSF leak.
Intractable Epistaxis
Uncontrolled posterior epistaxis can be controlled with endoscopic assistance in identification of the bleeding vessel30; this subject is described in Chapter 45.
Cerebrospinal Fluid Rhinorrhea and Anterior Meningoencephaloceles
Endoscopic repair is now standard for CSF rhinorrhea, with success rates higher than 90%.31 Meningoencephaloceles may also be repaired endoscopically.32 They are both described in detail in Chapter 54.
Noninvasive Fungal Rhinosinusitis
Allergic fungal rhinosinusitis and noninvasive fungal balls are usually treated endoscopically. A large antrostomy or ostioplasty is created. The fungal debris is irrigated and removed. See Chapter 48 for details.
Invasive Fungal Rhinosinusitis
Invasive fungal rhinosinusitis is almost exclusively a disease of the severely immunocompromised. All insensate mucosa and dead tissue must be débrided till healthy, bleeding tissue is encountered. An open approach may be required in extensive disease. The prognosis remains grim in spite of optimal débridement by any approach, as patients have multi-systemic comorbidities. See Chapter 48 for details.
Removal of Foreign Bodies
Endoscopy is helpful in visualization of foreign bodies and aids in their atraumatic removal.
Choanal Atresia Repair
Endonasal endoscopic approaches can be used to treat choanal atresia.33 Schraff and colleagues34 state that unilateral choanal atresia in children with the CHARGE association (coloboma [ocular], hearing deficit, choanal atresia, retardation of growth, genital defects [boys only], and endocardial cushion defect) can be managed successfully with a transnasal approach. However, patients with bilateral atresia should undergo primary transpalatal repairs owing to the high failure rate for the transnasal approach.34 To improve success rates, some writers advocate postoperative stenting, but others condemn it.35 Postoperative dilatation and mitomycin C therapy have been used.35 Endoscopic repair with use of an image guidance system may improve the success rate.36
Headache and Facial Pain
The role of surgery for treatment of headaches is controversial. Levine and associates37 described a multidisciplinary consensual approach on diagnosis and treatment of “sinus headache.” They stated that a stable pattern of recurrent headaches with headache as the presenting complaint is most likely migraine. Recurrent self-limited headaches associated with rhinogenic symptoms are also most likely migraine. Prominent rhinogenic symptoms with headache as one of several complaints should be evaluated for otolaryngologic pathology. Headache with associated fever and purulent nasal discharge is likely rhinogenic in origin, best assessed by nasal endoscopy and sinus CT.37 Moretz and Kountakis38 studied the effect of ESS on subjective headache scores in patients diagnosed with CRS. In a retrospective analysis of 201 patients, they compared headache scores preoperatively and 2 years postoperatively. An overall decrease in mean headache scores was noted at the 2-year follow-up.
For patients with normal CT findings and no rhinogenic cause of headache, the role of sinus surgery is debated. Becker and Cunning39 believe that limited ESS may cure headaches in patients with headaches that are frontal, retro-orbital, or both, in whom mild mucosal edema is found on endoscopy and sinus CT findings are normal. Parsons and Batra,40 and Clerico and associates41 hold that the finding of contact points on CT and/or endoscopy is a prerequisite for surgery. They also emphasize that the presence of contact points is not pathognomonic, because many patients with contact points have no headache. Clerico and associates41 state that it is important to “prove” the correlation of the contact point with headaches by noting the response to medical therapy or a diagnostic anesthetic block. Surgery should be offered only if patients have a clear reduction in headache in response to intranasal decongestants and anesthetic sprays, or obvious findings on endoscopy, CT, or both. In a retrospective series of 34 patients, Parsons and Batra40 reported a reduction in the intensity and frequency of headaches (91% and 85%, respectively) in patients who underwent ESS to relieve the contact points identified on CT. However, others are less optimistic. Stankiewicz42 states that surgery should be resorted to only after both thorough neurologic and radiographic evaluation and failure of medical therapy. A directed, targeted endoscopic sinus, septal, or turbinate operation should be used only if relief from medications point to a specific anatomic problem or if specific physical or radiographic data indicate a problem site. Even with these prerequisites, surgery has variable results, may be unsuccessful, and may worsen the headache. Long-term results may be poor, and a follow-up of at least a year is necessary to confirm a successful outcome.42
Tumors
Benign and malignant tumors of the nasal and paranasal cavities may be resected endoscopically or with endoscopy-assisted approaches.43–48 See Chapters 49 and 83 for a detailed description.
Expanded Utilization of Transnasal Endoscopic Sinus Approaches
The nose and the paranasal sinuses are being utilized as a pathway to approaching territories in the anterior and middle skull base, the intracranial cavity, and other regions in the skull. The endoscopic transnasal approach has gained widespread popularity for resection of pituitary tumors.49,50 Expanded approaches to the infratemporal fossa clivus, anterior and middle cranial fossa, and petrous apex have been described.51–55 These procedures are performed by a combined team of neurosurgeons and otolaryngologists and with the use of image guidance. Endoscopic transnasal approaches are also being applied to orbital procedures.56–61 The endoscopic dacryocystorhinostomy procedure is gaining popularity.56,57 Transnasal orbital decompression for Graves’ ophthalmopathy, optic canal decompression, and endoscopic transnasal strabismus surgery have also been described.58–61
Endoscopic Sinus Surgery for Rhinosinusitis
Pathophysiology of Chronic Rhinosinusitis
The nose and paranasal sinuses are lined by pseudostratified ciliated columnar epithelium with goblet cells. Functional cilia and normal mucus production are necessary to clear the sinuses of inhaled particulate matter and bacteria. Normal mucociliary transport is also needed to maintain ostiomeatal patency.62 The cilia of the maxillary and frontal sinuses transport mucus in specific patterns only toward the natural ostia, despite the presence of accessory ostia.63 Rhinosinusitis is usually preceded by a viral upper respiratory infection that impedes mucociliary clearance, causing blockage of the natural sinus ostia. The ensuing series of events create a milieu that is conducive to bacterial proliferation. This bacterial infection then perpetuates further mucosal thickening and worsens blockage.62 Allergies, likewise, can cause mucosal inflammation and edema. Anatomic obstruction of the ostia can be caused by septal deviations, concha bullosa, paradoxic middle turbinate, infraorbital cells, agger nasi cells, and nasal polyps. Cystic fibrosis, ciliary dyskinesia, and immunodeficiencies can impair mucociliary clearance and predispose to CRS.
The Principles of Functional Endoscopic Sinus Surgery
Minimally invasive sinus technique (MIST)64 is a targeted endoscopic intervention introduced in 1994. Its goals are similar to that of FESS with some differences that aim to standardize the procedure.
Preoperative Assessment
History
A thorough history is key. Specific review of CRS symptoms such as facial pain, congestion, nasal obstruction, drainage, and hyposmia is made. A detailed history of prior medical therapy for CRS is critical in determining whether the patient needs surgery. Current optimal medical therapy includes at least a 4-week course of antibiotics, nasal decongestants, topical nasal steroids, and, possibly, systemic steroids.65 One could make a strong argument that if CRS is an inflammatory disease, oral steroids should be part of the treatment protocol. Also, in the absence of any purulence, the role of antibiotics is currently questioned by many writers.65,66 Patients must have experienced failure of such treatment to be considered candidates for surgery. History of associated diseases and their treatment is obtained. These include allergy, asthma, polyps, aspirin sensitivity, and rhinitis medicamentosa. Exposure to smoking and environmental irritants is explored. Smoking causes mucosal inflammation and is associated with worse outcomes after ESS. Patients are counseled on the possibility of a poorer surgical outcome if they continue to smoke and are advised to stop smoking.67 The patient’s response to medical therapy, previous operations, and preexisting comorbidities influence their candidacy for surgery.
Examination
Office examination comprises a complete head and neck examination, a basic ocular examination, anterior rhinoscopy, and nasal endoscopy. Anterior rhinoscopy detects any significant septal deviation that may cause problems with nasal endoscopy. The condition of the mucosa, drainage, masses, and polyps are grossly visualized. Next, nasal endoscopy is conducted in a systematic fashion with a rigid or flexible endoscope. With rigid scopes, the examination is divided into three passes.68 The nasal floor, nasolacrimal duct, and nasopharynx are examined on the first pass. The second pass is carried out at a 30-degree angle with the nasal floor to examine the middle meatus, OMC, and sphenoethmoid recess. Lastly, the scope is directed superiorly toward the frontal recess. The character of the mucosa, appearance of the sinus drainage pathways, and the presence of anatomic variations, structural abnormalities, purulent drainage, and polyps is noted.
Radiographic Assessment
CT is more sensitive and specific for CRS than plain radiography.69 CRS is diagnosed on the basis of history and physical findings. CT scans are ordered either in patients with symptoms of rhinosinusitis but without examination findings or for planning of surgery for CRS. In all cases, care must be taken in interpreting “positive” CT findings and correlating them with symptoms. Prospective studies have shown that symptoms of rhinosinusitis frequently do not correlate with CT findings70 and that incidental sinus opacifications can be found on up to 27% of sinus CT scans.71 The severity of rhinosinusitis on preoperative CT scan does not predict the severity of symptoms as assessed by the Sinonasal Outcome Test-20 (SNOT-20) inventory in patients undergoing FESS.72 Further, CT scores fail to predict the amount of symptomatic improvement after FESS.72 In one prospective series, 146 adult patients undergoing ESS were evaluated with CT and the rhinosinusitis symptom inventory (RSI) preoperatively and at a minimum of 12 months postoperatively.73 The preoperative CT scans were staged according to three systems: Lund-Mackay, Kennedy, and Harvard. No significant correlation of CT stage with symptom domains was demonstrated.
Patients with CRS must be treated medically before a sinus CT is ordered. The CT should be obtained 3 to 4 weeks after therapy to evaluate the effect of treatment.74 If the CT scan then reveals evidence of persistent inflammation, surgery may be indicated. CT is performed to assess sinonasal anatomy and disease pattern so as to guide surgery.
Most sinus CT evaluations include coronal and axial views, with 2- to 5-mm intervals. Coronal views show the ostiomeatal unit and the relationship of the brain and orbit with the paranasal sinuses. These views are most useful in planning surgery. Axial CT views complement coronal views and must be obtained for planning of surgery for severe disease in the posterior ethmoid and sphenoid sinuses. Many institutions offer “screening sinus CT,” which includes a limited number of coronal views in the bone window. Screening sinus CT has been shown to be useful for the evaluation of sinusitis, but coronal CT with a maximum of 5-mm slices to avoid loss of information through skipped areas is needed for full appreciation of the anatomy of a surgical candidate.75 Modern CT scanners can perform 0.5-mm slices without prolonging scanning time.
The CT scans are carefully reviewed before surgery and must be available for review during the procedure to enable evaluation of the extent of disease and to assist with operative planning (Table 51-1). Meyers and Valvassori22 reviewed 400 preoperative CT scans with attention to anatomic variations. They found six specific variations that may predispose a surgeon to inadvertent penetration of the orbit or the anterior cranial cavity. These variations are (1) lamina papyracea lying medial to the maxillary ostium; (2) maxillary sinus hypoplasia; (3) fovea ethmoidalis abnormalities such as low or sloping fovea; (4) lamina papyracea dehiscence; (5) sphenoid sinus wall variations such as septa attached to the carotid, or dehiscence of the carotid or optic nerve; and (6) sphenoethmoidal cells. Hyperpneumatization of the frontal sinus, or presence of a frontal cell, may be associated with a deep fovea ethmoidalis.76 Blockage of any of the sinus drainage pathways can usually be identified from the presence of retained fluids within the sinuses. The cause of the blockage can also frequently be determined from the presence of thickened mucosa, polyps, or anatomic abnormalities. Calcifications or hyperintense signals can be evidence of fungus or tumors.
Table 51-1 Key Points to Be Reviewed on Preoperative Computed Tomography Scan Prior to Endoscopic Sinus Surgery
| Disease | |
| Bony integrity (erosion/expansion/dehiscence) | |
| Skull base | |
| Maxillary sinus | |
| Ethmoid sinus | |
| Sphenoid sinus | |
| Frontal sinus | Extent of pneumatization (deeper fovea ethmoidalis noted on side with a frontal cell and/or hyperpneumatized frontal sinus)93 |
| Miscellaneous |
Intraoperative Considerations
Image-Guided Navigation Systems
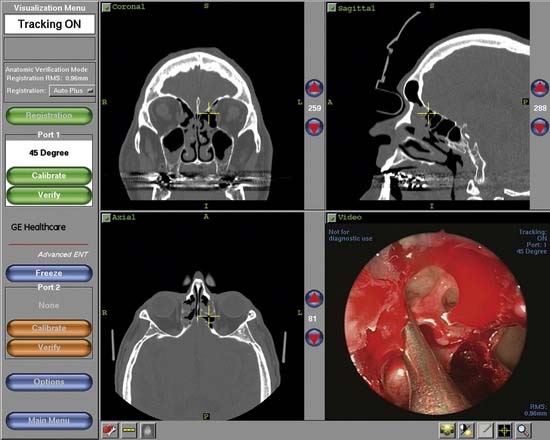
An inherent problem with endoscopic surgery is the two-dimensional view afforded by the use of the single lens. Navigational systems were developed to help reduce the risks of ESS. These systems use thin-cut CT scans that are reformatted in various planes to create a three-dimensional configuration. This three-dimensional view is then correlated with actual patient anatomy intraoperatively with the help of a computer (Fig. 51-4). The surgeon can place a probe on any structure to get a real time, three-dimensional view of the position of the probe. These computer-assisted navigation systems, which can be extremely helpful for difficult cases and for revision surgery, are gaining in popularity. Metson77 showed a 70.6% increase in the number of procedures using image guidance and a 92.8% increase in the number of surgeons using it in the first 2 years that this technology became available.
However, navigation systems are aids to the endoscopic sinus surgeon; they do not substitute for thorough understanding of the surgical anatomy. Even under ideal circumstances, they are associated with some degree of inaccuracy or error.77,78 Accuracy to within 2 to 3 mm is acceptable for image guidance systems, making them most useful in confirming identity of large compartments (posterior ethmoid versus sphenoid sinus) rather than distinguishing between millimeter increments such as in the skull base. Potential sources of error include variables during CT scanning, fiducial (reference device) or headset shift, soft tissue effects during surface registration, and operator-dependent errors during registration. Also, navigation systems are not needed for every case of ESS. There is an associated increase in operative time and cost. Depending on the system used and the medical facility charges, operating time and hospital cost may be significantly higher with use of a navigation system.77,78
As the use of image guidance systems becomes more popular, there is a question whether it is now the standard of care.79 The American Academy of Otolaryngology–Head and Neck Surgery80endorses use of these systems in the following example situations: (1) revision sinus surgery; (2) distorted sinus anatomy of developmental, postoperative, or traumatic origin; (3) extensive sinonasal polyposis; (4) pathology involving the frontal, posterior ethmoid, and sphenoid sinuses; (5) disease abutting the skull base, orbit, optic nerve or ICA; (6) CSF rhinorrhea or conditions in which there is a skull base defect; and (7) benign and malignant sinonasal neoplasms. Tabaee and colleagues,81 comparing 60 patients undergoing image-guided surgery with 179 patients undergoing ESS without image guidance, found no statistically significant difference in the incidences of major intraoperative complications, major postoperative complications, revision procedures, and postoperative SNOT-20 symptom scores.81 However, a higher incidence of intraoperative CSF leak was noted in the group undergoing surgery without image guidance—2.2%, vs. 0% in the image-guided surgery group. Javer and Genoway82 report that though the long-term effect of image-guided surgery as measured by patient quality of life (QOL) remains unknown, there appears to be a significant trend indicating greater QOL improvement in the short term over non–computer-assisted FESS techniques.82
Intraoperative Computed Tomography Scans
The major disadvantage of image-guided surgery is that the CT scans are obtained before the procedure and may not reflect the intraoperative disease process. Attempts have been made to overcome this drawback. Brown and associates83 reported that near–real time image-guided sinus surgery using intraoperative fluoroscopic CT is feasible.83 Jackman and colleagues84 described the use of intraoperative CT scanning in 20 subjects undergoing ESS. In their study, intraoperative CT scans were obtained successfully in less than 40 seconds and could be loaded into the image guidance system within minutes. New information obtained from these intraoperative scans led to performance of additional surgery in 30% of their patients. Suzuki and coworkers85 reported use of real-time magnetic resonance imaging guidance in ESS through the use of an optical tracking system during ESS.
Choice of Anesthesia
Local Anesthesia
ESS using purely local anesthesia can be performed. The biggest drawback of local anesthesia is poor sedation. A talented, interested, and experienced anesthesiologist is required for good sedation. Without this key medical colleague, general anesthesia should be used. Sedation with local anesthesia calms patients, stabilizes blood pressure, and minimizes bleeding. ESS with use of local anesthesia may, in theory, improve safety because awake patients can report manipulation of the orbital periosteum or dura. Local anesthesia works well for young patients undergoing primary sinus surgery that lasts less than 2 hours. If the patient becomes unstable during surgery, bleeding should be quickly controlled, intravenous sedation should be stopped, the procedure should be halted, and general anesthesia should be administered. In a retrospective review of 177 patients, Fedok and associates86 compared complication rates and recovery times in patients undergoing elective septoplasty or ESS using local anesthesia with sedation with rates in patients undergoing the same procedure using general anesthesia. Total operative and recovery times were shorter in patients receiving local anesthesia with sedation. The frequency of emesis, epistaxis, and nausea was less in the local anesthesia group. Three patients who received general anesthesia required unplanned admissions. An older, retrospective review of 232 patients showed a slightly higher complication rate for local anesthesia with sedation than for general anesthesa.87 Another study found no appreciable difference between local with sedation and general anesthesia in terms of postoperative pain, nausea, vomiting, and overall tolerance of ESS.88
General Anesthesia
The principal advantages of general anesthesia are independence from patient cooperation and the control of the airway. Reasons to choose general anesthesia include patient anxiety, operation in a child, and anticipation of a long procedure.88 General anesthesia is also indicated if computer-assisted navigation systems are used, because any patient movement may disrupt the reference device. Even if general anesthesia is used, topical nasal decongestant sprays and local injections are still helpful for vasoconstriction and postoperative pain.
In a prospective randomized controlled trial with 56 patients, Wormald and colleagues89 reported that total intravenous anesthesia (propofol with remifentanil) may be superior to inhalational anesthesia (sevoflurane with fentanyl) in providing a better surgical field, especially for patients with polyposis, allergic fungal rhinosinusitis, and higher Lund-Mackay scores. These findings are supported by Ahn and coworkers,90 who report lower blood loss and better surgical field with propofol-remifentanil intravenous anesthesia than with sevoflurane-remifentanil anesthesia in a prospective randomized controlled trial involving 40 patients. However, Beule and associates91 report that under conditions of balanced circulatory parameters, equal blood loss and endoscopic vision can be achieved with the two tested anesthetic regimens. In a prospective randomized controlled trial of 46 patients (22 sedated with sevoflurane/fentanyl, 24 sedated with propofol/fentanyl), these researchers found no difference in total blood loss, blood loss per minute, or endoscopic vision. Platelet function was significantly impaired 45 minutes after onset of surgery in both groups but was more pronounced after propofol anesthesia.



