Symptoms with Vitreous Opacities and Specific Examinations
Clear refractive media allow direct observation and diagnosis of vitreous disorders in their early stages. Ultrasound studies are indicated if direct visualization of vitreous pathology is not feasible. Dynamic ultrasound studies in particular provide valuable diagnostic information.
If history findings are equivocal, conventional radiography or computed tomography is indicated to rule out an intraocular metallic foreign body. Magnetic resonance imaging (MRI) can detect and localize nonmetallic foreign bodies.
Symptoms with Vitreous Changes
- diffuse fog
- changing visual impairments
- moving shadows
- varying position of opacities
- glare, discomfort
Objective examination of the vitreous body:
- observation under retroillumination
- shadows in the pupil
- slit lamp
- structures in the anterior vitreous body
- mass of tissue posterior to the lens (leukocoria)
- structures in the anterior vitreous body
- 78-diopter lens
- structures in the posterior vitreous body
- three-mirror lens
- preretinal and peripheral structures
- ultrasonography
- sonographic cross-sectional image and echo structure
- computed tomography
- radiographic cross-sectional tomography
- magnetic resonance imaging
- cross-sectional image and tissue structure.
 Leukocoria
Leukocoria
Leukocoria or amaurotic cat’s eye is one characteristic symptom. This refers to a whitish-gray–brown mass that fills the vitreous chamber up to the posterior surface of the lens. It is already visible to the unaided eye or with a flashlight without other optical aids.
Leukocoria (Amaurotic Cat’s Eye)
- whitish, gray-brown mass that fills the entire vitreous chamber posterior to the lens.
- visible with the unaided eye
 Causes of leukocoria:
Causes of leukocoria:
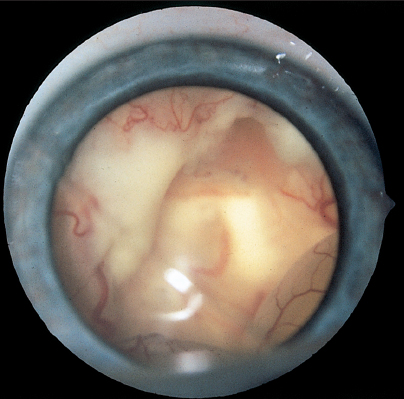
Fig. 5.1 Leukocoria due to an advanced retinoblastoma—amaurotic cat eye
Like retinoblastoma (p. 123), a persistent primary hyperplastic vitreous body is a rare condition that should be considered in the diagnostic workup. During the course of embryonic development, it grows as a thick white strand of tissue between the optic disc and the posterior surface of the lens, forming a white vascularized plate. At first glance, it resembles a congenital cataract. Examination under the slit lamp or operating microscope with the patient under general anesthesia will reveal a thick retrolenticular cord of tissue. It is often connected to the ciliary body. As the eyeball grows, the plate of connective tissue posterior to the lens is unable to expand. The ciliary processes are then pulled inward to form a wreathlike structure around the plate of scar tissue. The view of the fundus is usually obscured. If these masses lay further posterior to the lens, they may not be immediately visible although they will cast a shadow on the pupil under retroillumination.
Treatment: the disorder is treated by vitreoretinal surgery but the prognosis is poor.
Persistent Hyaloid Artery
- strands of connective tissue projecting from the optic disc into the vitreous body
 Blood Vessels in the Vitreous Body
Blood Vessels in the Vitreous Body
 Persistent Hyaloid Artery arising from the Optic Disc
Persistent Hyaloid Artery arising from the Optic Disc
During embryonic development, this blood vessel arises from the optic disc and extends through the vitreous body to the lens. It normally atrophies and disappears before birth. Occasionally, sizeable remnants persist. They appear as strands of connective tissue projecting into the vitreous body from the optic disc.Occasionally remnants of this artery are thicker, contain blood, or are enveloped in connective tissue. They then appear as a compact prepapillary mass. A persistent hyaloid artery can be so thick that stout cords are seen to extend into the vitreous body, occasionally connected to sail-like sheets of connective tissue. These structures can obscure the central retina and fovea centralis, impairing visual acuity. Such cases lead to suppression amblyopia.
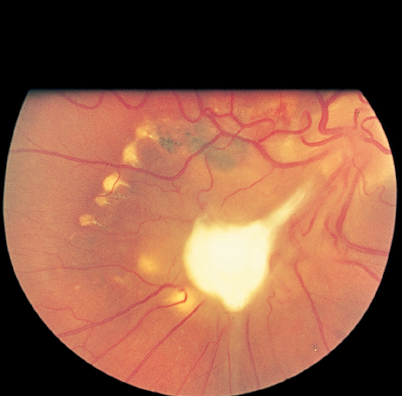
Fig. 5.2 Persistent hyaloid artery extending far into the vitreous body.
Treatment: none.
Proliferative Retinopathy
- neovascularization—lattices and tufts and fans of vessels
- proliferation of connective tissue
- streaks of blood and clots
- shadows under retroillumination
- pupil is black
- diffuse, unstructured opacities
 Active Neovascularization in the Vitreous Body in Proliferative Retinopathy
Active Neovascularization in the Vitreous Body in Proliferative Retinopathy
Pathologic vascularization occurs when ischemic areas of the retina release toxic substances that accumulate in the surrounding retina and adjacent vitreous. Lactate, prostaglandins, and vascular endothelial growth factor (VEGF) are known to stimulate neovascularization. Such newly formed blood vessels are often the source of vitreous hemorrhages. These are only slowly absorbed and in turn lead to proliferation of connective tissue and further neovascularization in the vitreous body.
Vitreous opacities are initially very easy to diagnose: ophthalmoscopic retroillumination reveals shadows that darken the pupil, which is normally brightly illuminated. Examination with the slit lamp, three-mirror lens, or 78-diopter ophthalmoscope will reveal whether the opacity is diffuse, i.e., a uniformly distributed foglike opacity, or cloudlike opacities disseminated between the strands of the vitreous. Gray opacities are usually attributable to old hemorrhages. They are due to the breakdown of blood cells with resulting precipitation of proteins. Opacities resulting from cellular infiltration are often characterized by individual cell bodies that appear light gray or as glistening dots under the slit lamp. Acute hemorrhages appear as red bands, although within a few hours they condense into visible clots. Occasionally one will also find areas of neovascularization and connective tissue proliferation between cloudlike opacities, or the origin of the pathologic vascular proliferations in the vascular structures of the retina or on the optic disc.
In proliferative retinopathy, sail-like opacities extend through the vitreous body and form a solid, organized structure. Cloudlike vitreous hemorrhages accumulate between them, so that the eye becomes completely opaque. The vitreous proliferations shrink as the disorder progresses. Because they are attached to the retina, they pull it away from of its underlying tissue, causing tractional retinal detachment.
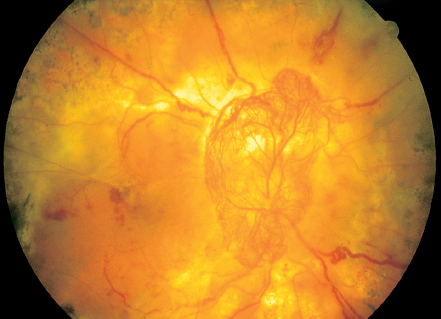
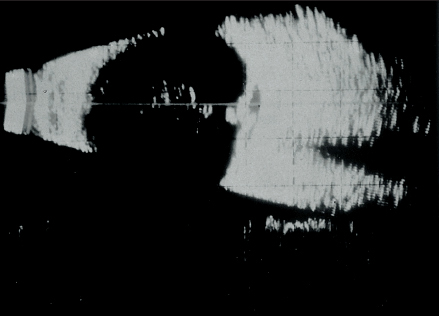
Fig. 5.4 B-mode ultrasound in proliferative diabetic retinopathy. The fine echo line anterior to the optic disc disappears as the ultrasound beam attenuates.
 Ultrasound findings in vitreous opacities include:
Ultrasound findings in vitreous opacities include:
- cloudlike opacities
- vitreous proliferations
- retinal detachments.
Vitreous opacities resulting from proliferative retinopathy are often so dense that ophthalmoscopy is no longer feasible. Ultrasound is a valuable modality in such cases. Diffuse opacities are not detectable with ultrasound. However, the position and size of cloud like opacities of varying density can be diagnosed in the A-mode and B-mode images. Proliferations are seen reliably on ultrasound images. Often it is even possible to identify their origin in the retina. A retinal detachment is readily distinguishable from vitreous opacities and proliferations by the strong and sharply defined echo of the retina. Diagnostic ultrasound thus supplies important information for the planning and prognosis of a vitrectomy.
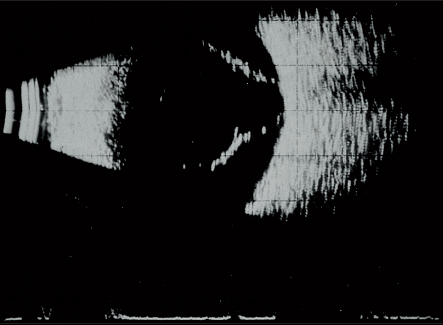
Fig. 5.5 Ultrasound image of total retinal detachment. The retinal echoes remain as the ultrasound beam attenuates.
 Disorders with proliferative retinopathy:
Disorders with proliferative retinopathy:
Treatment: vitreoretinal surgery.
Floaters
- harmless, very fine vitreous condensation densities
- inspect fundus for possible lesions
 Small Opacities in the Vitreous Body
Small Opacities in the Vitreous Body
 —Floaters—Moving Spots against a Bright Background
—Floaters—Moving Spots against a Bright Background
In young persons, the vitreous body with its cortical layer, the internal limiting membrane, is in close contact with the retina. With advancing age, the vitreous body deteriorates. The gel, which contains hyaluronic acid, gradually liquefies. The collagen strands of the vitreous stroma condense and form prominent vitreous fibers. This creates small vitreous densities that often go undetected by slit lamp biomicroscopy. Patients perceive these densities as fine punctate figures or dancing shadows in front of the eye when the gaze is directed at a bright background. They are known as floaters. Although they can be subjectively bothersome, they are harmless as long as they are not associated with any other abnormal retinal changes.
There is no treatment, but none is necessary. If floaters appear or change, the fundus, especially the periphery, should be examined in mydriasis to determine whether lesions are present that could lead to retinal detachment.
Treatment: none. Fundus examination is indicated as a precaution.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


