History
Lines of inquiry in history taking:
family history
- systemic disorders, such as heart attack, stroke, rheumatic disease, infections, diabetes mellitus, and other metabolic disorders, age of parents at death, familial or hereditary disorders
- ophthalmic disorders such as cataract, glaucoma, strabismus, corrective lenses, inflammation, low vision, or blindness
- systemic disorders, such as heart attack, stroke, rheumatic disease, infections, diabetes mellitus, and other metabolic disorders, age of parents at death, familial or hereditary disorders
patient’s medical history
- as above
- inquire about accidents.
- as above
ophthalmological history
- as above
- inquire about injuries
- current history, have patient describe disorders and complaints in chronological order.
- as above
First, the examiner inquires about complaints relating to the eyes. This exchange should be interactive, meaning that the examiner can always use the patient’s answers as the basis for more detailed questions. Naturally, the examiner should not deviate from the systematic approach to history taking. The systemic disorders mentioned in the patient’s medical history often provide important information about an ophthalmic disorder. Experience has shown that patients initially tend to deny any connection when asked about familial disorders, i.e., hereditary disorders of the eyes. Often only the next consultation or a subsequent one reveals important information regarding the family history, which then enables the examiner to draw a family tree.
 Functional Tests
Functional Tests
Meticulous functional testing is essential. This should be preceded by inspection of the anterior eye and objective measurement of refraction. Functional tests provide important information about damage to the retina and the visual system, and supplement the morphologic examinations.
 Visual Acuity
Visual Acuity
Standards for visual acuity:
decimal scale 0.05–1.2
Snellen scale: 5/4–5/50 (meters) or 20/20–20/200 (feet)
- numerator: distance of optotype in meters or feet, both as logarithmic scales
logMAR scale (Minimum Angle of Resolution): linear scale suitable for comparison of poor values with visual acuity less than 5 meters. LogMAR = log10 of the minutes of arc (min arc).
Diagnostic signs in visual acuity testing:
hesitancy in reading: large visual field defect
skipping individual letters: small central defects
plus lens phenomenon: macular edema, specifically in central serous chorioretinopathy.
 Visual Field
Visual Field
Perimetry determines the photosensitivity of individual points on the retina at any specified location on the fundus. At selected points on the retina, the sensitivity threshold for light stimuli is precisely determined with the aid of automatic computer perimetry testing. Usually, white light is used for the examination. Perimetry with blue and yellow contrasts has diagnostic significance in optic nerve disorders, especially in primary open-angle glaucoma. Data from computerized perimetry can also be statistically analyzed which allows nearly objective evaluation of the clinical course of disorders.
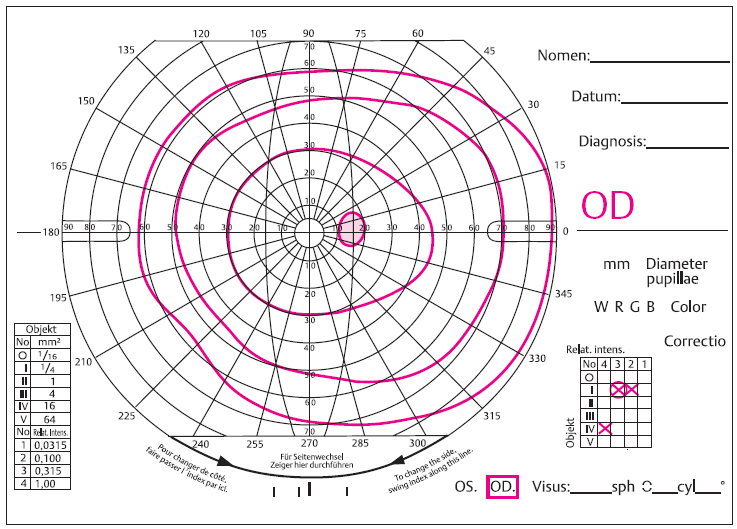
Fig. 2.1 Goldmann visual field. OD = right eye. The fundus is divided into a lattice of angular graduations to precisely localize points on the retina.
Visual field testing is required in the following cases:
glaucoma
optic nerve disorders
suspected neuro-ophthalmologic lesions
dysfunctions that are readily detectable by ophthalmoscopic examination of the fundus
loss of visual acuity of uncertain etiology.
 Color Vision
Color Vision
Pseudoisochromatic plates such as the Ishihara, Velhagen, or Stilling plates are sufficient for the initial clinical examination. The anomaloscope is used to differentiate congenital color vision defects. The Farnsworth tests are often helpful with congenital maculopathies.
Indications for examining color vision:
hereditary color vision defects
optic neuritis
Stargardt disease (red–green)
cone dystrophy (blue–yellow)
dominant hereditary optic nerve atrophy (blue–yellow deficiency)
ethambutol therapy (various color vision defects).
 Contrast Sensitivity
Contrast Sensitivity
Contrast sensitivity deficiencies are examined using checkerboard or striped patterns. Deficiencies are evaluated by psychophysical assessment or by using the pattern visual evoked potentials (VEP) or by electroretinogram (ERG). The examination methods are not standardized and are therefore generally not comparable. Despite this drawback, measurement of contrast sensitivity has already become valuable in diagnosing subtle dysfunctions of the macula and optic nerve.
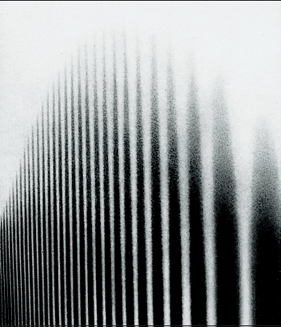
Fig. 2.2 Diagram of contrast sensitivity. The spatial frequency increases from right to left, meaning the width of the black bars decreases. Their contrast decreases from bottom to top. This creates the curve of the contrast sensitivity function at the upper margin of the image (Körner H. Visuelle Auflösungsgrenzen und Fehlsichtigkeit. Hildesheim, Zürich, New York: Georg Olms Verlag; 1995: 261).
Ophthalmoscopic Technique for Clinical Diagnostic Examination
optic disc, macula, and vascular structures
- classic ophthalmoscope
- +78-diopter lens with slit lamp
- classic ophthalmoscope
broad overview of vasculature and periphery
- indirect ophthalmoscope, +20-diopter lens
- +90-diopter lens with slit lamp
- indirect ophthalmoscope, +20-diopter lens
details with microscopic precision, limited overview
- three-mirror lens with slit lamp
 Ophthalmoscopy
Ophthalmoscopy
Pharmacologic mydriasis:
example of an eye-drop mixture
- tropicamide 0.5%
- phenylephrine 5%.
- tropicamide 0.5%
 Direct Ophthalmoscopy
Direct Ophthalmoscopy
Direct ophthalmoscopy is used to evaluate details of the optic disc, fovea centralis, retinal fixation, and retinal vasculature.
 Indirect Ophthalmoscopy
Indirect Ophthalmoscopy
Indirect ophthalmoscopy offers a broader overview of the fundus than the direct method, depending on the refractive power of the employed lens. It readily allows examination of the fundus as far as to the periphery. The convenient monocular indirect ophthalmoscope is equally as effective as binocular ophthalmoscopes mounted on a headband or eyeglass frames. The latter types convey a stereoscopic image and the examiner’s hands are free. The headset allows the examiner to simultaneously indent the eyeball to better visualize peripheral retinal changes or perform surgical procedures, such as buckling operations. Indirect ophthalmoscopy is also frequently used in the operating room as well as for bedside examinations and inspection of the fundus in children.
Size of the fundus images:
indirect ophthalmoscopy
- 14–28-diopter lenses: 20°–40°
- 5–10 disc diameters
- 4–6× magnification
- 14–28-diopter lenses: 20°–40°
direct ophthalmoscopy
- 8°, approximately 2 disc diameters
- 14–16 × magnification.
- 8°, approximately 2 disc diameters
 High Refractive Power Lenses in Conjunction with the Slit Lamp
High Refractive Power Lenses in Conjunction with the Slit Lamp
High refractive power lenses used in conjunction with the slit lamp combine the broad overview of indirect ophthalmoscopy with the high degree of detail of direct ophthalmoscopy.
 Contact Optics with Deflecting Mirrors
Contact Optics with Deflecting Mirrors
These are very important for stereoscopic visualization of details of the central fundus at 10–30 × magnification and for biomicroscopic examination of the periphery.
 Special Considerations when Examining Infants and Newborns
Special Considerations when Examining Infants and Newborns
The pupils of these small patients may be dilated using the same drops as in adults. General anesthesia is often required to immobilize the patients for the examination. Direct or indirect ophthalmoscopy may then be performed as required. Under the operating microscope, a 78 or 90-diopter lens or a three-mirror lens may be used. Under these conditions the eye is easily rotated by inserting a muscle hook into the conjunctival fornix.
 Objective Imaging Studies and Their Evaluation
Objective Imaging Studies and Their Evaluation
 Fundus Photography
Fundus Photography
Photographs or video sequences are used not only to document findings but also to detect certain details. Photographs obtained in green light better visualize blood vessels; nerve fibers appear more clearly in blue light and pigmented structures in red light. Stereoscopic images can also visualize three-dimensional structures.
Image size in photography:
20°: many details are magnified
45°–50°: broader overview, sufficient detail
90°–110°: overview for large lesions, no detail (rarely used).
Advantages of the scanning laser ophthalmoscope:
good images through a narrow pupil
minimal light stress.
 Scanning Laser Ophthalmoscope
Scanning Laser Ophthalmoscope
Scanning laser ophthalmoscopes produce high-contrast images even through narrow pupils. Using various color lasers, this method can visualize particular structures of the retina noninvasively, i.e., without injection of a contrast agent. These structures include nerve fibers, drusen, nevi, and autofluorescent material. This examination technique is currently undergoing further development and continues to provide new knowledge.
Heidelberg Retina Tomograph
The Heidelberg retina tomograph is a special scanning laser ophthalmoscope that produces images of the optic disc and macula layer by layer with confocal optics at high magnification, visualizing these structures as a sequence of “optical slices.” The three-dimensional size of the optic disc excavation can be calculated from the sum of the images. This method can precisely document specific changes in an individual optic disc over time.
Diagnostic significance of the Heidelberg retina tomograph in glaucoma:
measuring the optic disc
assessing an excavation
follow-up of optic disc findings
deducing visual field defects

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


