The normal optic disc is sharply demarcated, lies in the plain of the fundus, and is well perfused. It normally appears pink, in contrast to the whiteness of optic nerve atrophy. On fluorescein angiography, the capillaries visible in the optic disc fill as in a normal angiogram. Hyperfluorescence of the optic disc is a sign of pathology, and the examiner should then look for an abnormal change. There are a number of harmless anomalies that must be distinguished from abnormal changes.
Definition of Optic Disc Edema
- structures appear blurred
- hyperemia, i.e., erythema
- elevation above the plain of the retina
 Blurred Appearance, Hyperemia, and Protrusion—Optic Disc Edema
Blurred Appearance, Hyperemia, and Protrusion—Optic Disc Edema
Like disorders of the retina, pathologic changes of the optic disc can be diagnosed on the basis of appearance. The term optic disc edema refers to swelling of the optic nerve at its entry point into the eyeball. The tissue of the optic disc appears blurred and hyperemic, and it protrudes into the interior of the eye. If this protrusion of the optic disc is pronounced and exceeds three diopters or one millimeter, it is then referred to as papilledema. Until the optic disc elevation exceeds 1 mm, both papilledema and optic disc edema appear identically. There are many different causes of swelling of the optic disc that require different treatments. Proper diagnosis is therefore very important.
Causes of swelling of the optic disc:
- anomalies
- congenital malformations
- inflammatory edema
- ischemic edema
- edema due to increased intracranial pressure.
 Bilateral Blurring of the Optic Disc with Hyperemia and Prominence
Bilateral Blurring of the Optic Disc with Hyperemia and Prominence
Causes of blurred and hyperemic optic discs:
- bilateral
- papilledema
- arterial hypertension
- idiopathic-increased cerebrospinal fluid pressure
- tobacco-alcohol amblyopia
- Leber hereditary optic neuropathy
- amiodarone therapy
- pseudopapillitis in hyperopia
- papilledema
- unilateral
- anterior ischemic optic neuropathy (AION)
- optic neuritis
- tumors
- optic disc drusen
- other disorders such as central retinal vein occlusion
- hypotension syndrome
- hyperopic optic disc, unilateral and bilateral.
- hypotension syndrome
- anterior ischemic optic neuropathy (AION)
Papilledema with Increased Intracranial Pressure
Pathogenesis and Symptoms of Papilledema
The optic nerve sheath connects the optic disc with the subarachnoid space. Therefore, increased intracranial pressure acts on the optic nerve to produce visible changes in the optic disc. The tissue pressure causes protrusion of the optic disc, giving it a characteristic appearance. The optic disc is then ill defined and hyperemic. Findings on the optic disc include engorged vessels and capillaries that are not normally visible. The prominence is measured in diopters on direct ophthalmoscopy or in millimeters on ultrasound. When measuring with direct ophthalmoscopy, the examiner compares the setting at which the adjacent retina appears sharply focused to that in which the apex of the prominence is in focus. The examiner counts the number of diopters required to “climb up” the protrusion of the optic disc and bring it into focus. The prominence can measure up to 10 diopters.
Increased intracranial pressure generally leads to papilledema in both eyes (except in total optic nerve atrophy). The protrusion can be significant, giving the optic disc the appearance of a mushroom. The vasculature is almost invariably prominent and tortuous, and the veins are often engorged well into the retina.
Signs of Papilledema
- usually bilateral (exception:total optic nerve atrophy)
- optic disc blurred and hyperemic disc margin and blood vessels obscured
- elevation <1 mm,
- veins engorged
- spontaneous pulsation of veins absent
Acute Papilledema
- radial bleeding in the nerve fiber layer
- cotton-wool spots
- visual acuity remains good for a long time
- enlarged blind spot
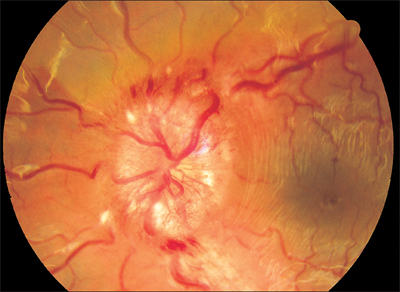
Fig. 6.1 Papilledema, ill-defined, hyperemic, and with elevation of 6 diopters in a 12-year-old girl with a brain tumor. Identical findings were seen in both eyes.
Clinical Picture of Papilledema
Papilledema does not initially impair vision. An enlarged blind spot is the only abnormality in the visual field. If the papilledema persists for several weeks, retinal edema and hard exudates often occur in the peripapillary areas of the retina. They extend into the macula, often in association with retinal folds. These changes then lead to diminished visual acuity.

Chronic papilledema causes permanent damage to the optic nerve and alters its appearance after a few weeks. The optic disc remains blurred but turns pale and increasingly white. Optic nerve atrophy occurs. The prominence subsides once intracranial pressure returns to normal; however, the visual field defects are irreversible.
Bilateral papilledema is an ophthalmologic emergency that requires immediate neurologic examination and treatment if indicated.
Treatment: prompt neurosurgical treatment; Elimination of the cause of increased intracranial pressure is indicated.
Signs of chronic Papilledema
- disc elevation like champagne cork
- retina edema surrounding disc
- hard exsudates, gliosis, drusen
- retinal wrinkles in makula
- decrease in visual acuity
- optic nerveatrophy with persistent intracranial pressure
- optic disc turns pole
Papilledema Is an Emergency
- immediate neurologic examination
- immediate CT or MRI examination of the brain
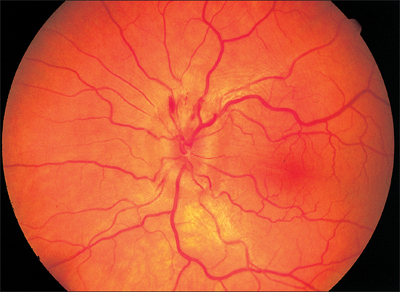
Fig. 6.3 Optic disc edema in a 42-year-old man with arterial hypertension. Optic disc findings are identical in both eyes. Systemic diagnosis was made on the basis of hypertensive retinopathy. Elevation of the optic disc is 2 diopters.
Bilateral Blurring and Hyperemia of the Optic Disc in Arterial Hypertension
Optic Disc Edema in Arterial Hypertension
- invariably bilateral
- constricted retinal arterioles
- capillary ectasia
- cotton-wool spots
- hard exudates
- measure patient’s blood pressure immediately
- when in doubt, diagnostic studies as in papilledema are indicated
Chronic arterial hypertension, especially with high diastolic values, can result in bilateral optic disc edema with significant prominence. This means that papilledema requires more than just neurologic examination. Meticulous evaluation of the retinal arterioles is necessary if the optic disc edema is to be correctly interpreted as the initial symptom of hypertensive retinopathy. The arterial hypertension then requires examination and treatment by an internist.
Treatment: management of the arterial hypertension by an internist.
Bilateral Papilledema with Idiopathic Intracranial Hypertension
Signs and Symptoms in Idiopathic Intracranial Hypertension
- often overweight women age 20-40
- bilateral papilledema
- clinical course lasting several years
- no neurologic deficits
- transientvisual obscurations for a few seconds
- often tinnitus
- sixth nerve palsy
- concentric narrowing of visual field
- decrease in visual acuity
- blindness in both eyes
Bilateral papilledema can result from idiopathic increased cerebrospinal fluid pressure in a condition referred to as pseudotumor cerebri. Patients suffer headache, nausea, vomiting transient obscuration of vision, and as disease progresses increasing defects in the periphery of the visual fields. Arterial blood pressure is normal, except for occasional sixth nerve palsy, neurologic symptoms are absent, and there is no evidence of a cerebral mass. Even a lumbar puncture will reveal elevated cerebrospinal fluid pressure only, when measured immediately after puncture, the so-called opening pressure.
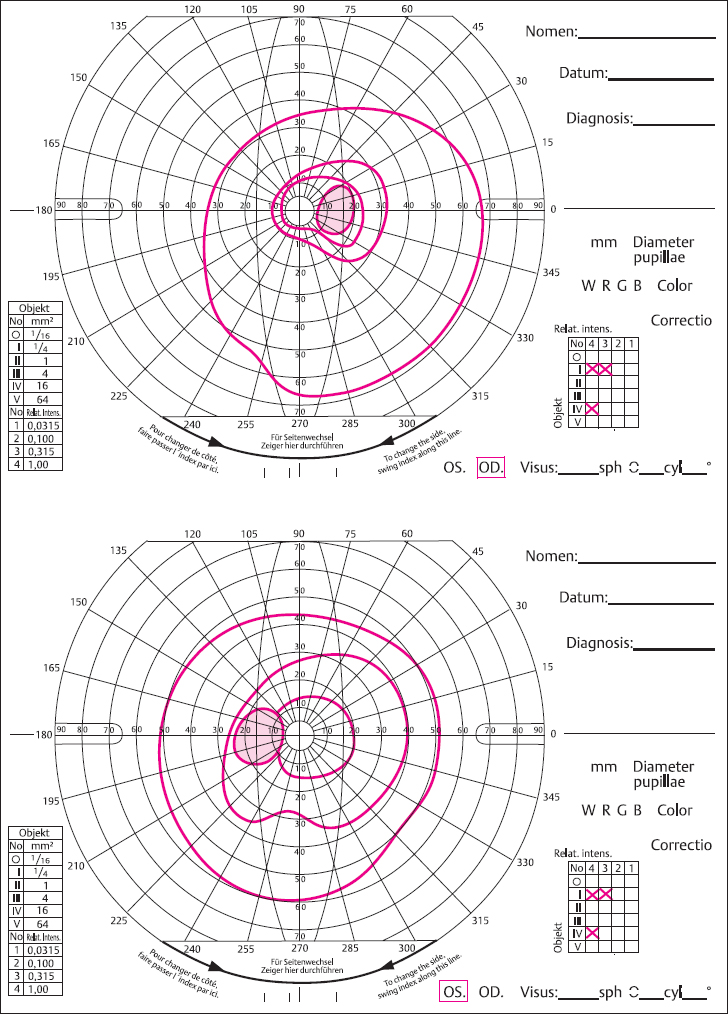
Fig. 6.4 a and b Idiopathic intracranial hypertension elevated (OS = left eye, OD = right eye). a Concentric narrowing of both visual fields. Bilateral papilledema with elevation of 5 diopters.
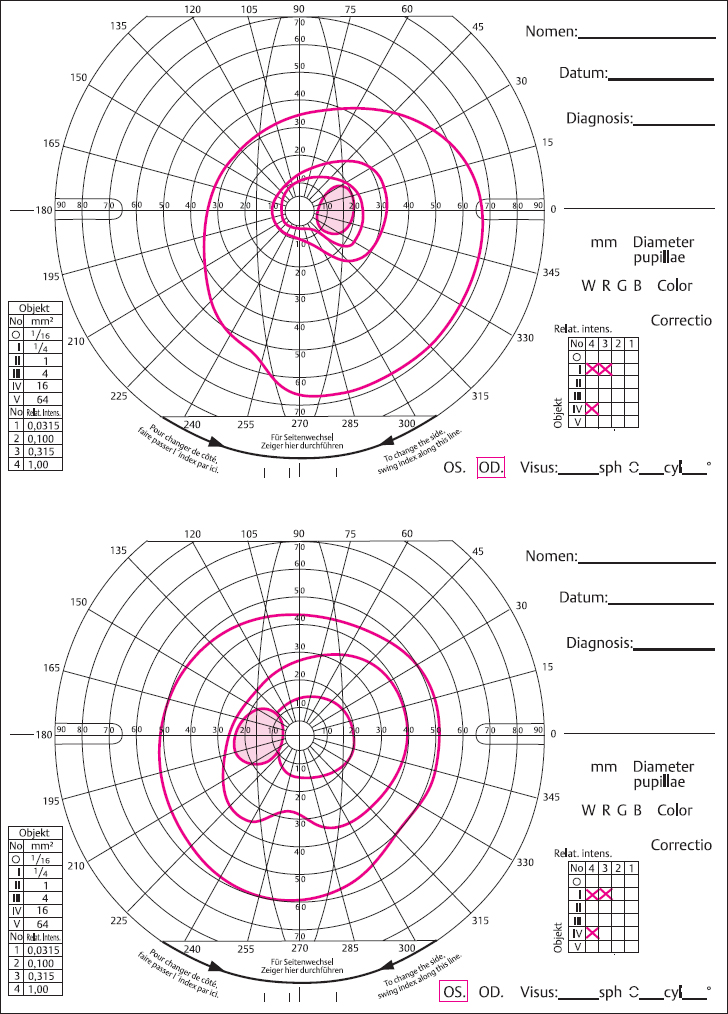
Fig. 6.4 b Visual fields in the same patient five weeks later.
Signs of MRI
- optic nerve sheath dilated
- elevation of optic dis
- posterior flattening of globe
- ventricles often narrow
- observe sinus veins
- consider MR venography
Differential Diagnosis of Idiopathic Intracranial Hypertension after Exclusion of Intracranial Mass
- optic disc drusen
- arterial hypertension
- pseudopapillitis in hyperopia
- sinus vein thrombosis
- dural arteriovenous malformations
- obstructive sleep apnea
Diagnostics in papilledema without a brain tumor:
- principal sign: bilateral chronic papilledema
- suspicion of idiopathic intracranial hypertension (increased cerebrospinal fluid pressure)
- history of recent weigh increase
- examine visual field with automatic threshold perimetry
- ocular motility: sixth nerve palsy
- neurologic examination
- emergency MRI to rule out intracranial mass
- consider differential diagnosis of sinus venous thrombosis
- if suspicion of vascular abnormality, MR-angiography, and MR-venography
- measurement of cerebrospinal fluid opening pressure, >200mmH2O is pathologic
- if visual field defects found, urge patients to consider surgical treatment.
Treatment: prompt therapy to reduce intracranial hypertension by high doses of acetazolamide, weight loss, decompression of the optic nerve sheath via a longitudinal retrobulbar incision. If intracranial pressure remains elevated, lumboperintoneal or ventriculoperitoneal shunt operation.
Bilateral Optic Disc Edema in Acute Nutritional Optic Neuropathy—Tobacco-Alcohol Amblyopia
Nutritional Optic Neuropathy— Tobacco–Alcohol Amblyopia
- bilateral
- optic disc edema initially present
- decrease in visual acuity
- cecocentral scotoma
- increasing visual field defects
- vitamin B1 deficiency
- later pale optic disc
- optic nerve atrophy
Tobacco-alcohol amblyopia is a toxic bilateral optic neuropathy attributed to abuse of ethyl alcohol and tobacco. It occurs when large quantities of alcohol are consumed in conjunction with an excess of tobacco over a prolonged period (at least several months). Presumably, alcohol and the cyanide contained in the tobacco smoke combine to cause chronic intoxication. Often persons who consume excessive amounts of alcohol and tobacco are also undernourished, in which case deficiencies of thiamine (vitamin Bl) and cobalamin (vitamin B12) may also play a part in the pathogenesis of this disorder.
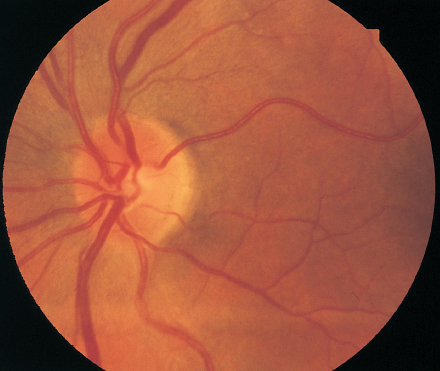
Fig. 6.5 Tobacco-alcohol amblyopia in a 57-year-old male alcoholic. Both optic discs are ill-defined and hyperemicwith elevation measuring 2-3 diopters. Visual acuity in the right eye is 20/100, in the left eye 20/400.
The functional impairments begin in both eyes as diminished visual acuity. A cecocentral scotoma is present. In the first few weeks, both optic discs appear blurred and hyperemic. No significant prominence is detectable. The visual field defects increase in size and the optic disc gradually turns pale during the course of the disorder. Optic nerve atrophy develops, and findings include a particularly excavated, pale, gray optic disc. The visual impairments and visual field defects are irreversible.

Fig. 6.6 Right optic disc in a 22-year-old man with Leber hereditary optic neuropathy. Both optic discs are pale with a reddish shimmer and ill-defined margins.
Leber Hereditary Optic Neuropathy (LHON) with Bilateral Blurring and Hyperemia of the Optic Disc
Signs of Leber Hereditary Optic Neuropathy
- manifestation at age 10-30
- optic discs initially exhibit telangiectasia, microangiopathy, hyperemia, and blurred appearance
- visual acuity decreases to 20/100-20/200
- cecocentral scotoma
- temporal pallor after three to six months
- occasional spontaneous remission
- later bilateral optic nerve atrophy
The disorder largely follows a sex-linked hereditary pattern. It manifests itself in 85% of all patients in young men and in 15% in women between the ages of 10-30. Children of diseased men are clinically normal. Women can be carriers. Clinically healthy women from pedigrees that include diseased persons pass the disorder on to all their male offspring and to 8-15% of their female children. The disorder is inherited as a result of defects of mitochondrial deoxyribonucleic acid identified by molecular biology techniques. This means that the mutation is apparently transmitted in the cytoplasm of the maternal ovum. The mitochondrial transmission of the mutation causing the disorder entails a certain probability that the maternal ovum contains and can pass on normal mitochondria in addition to mutated mitochondria. Referred to as heteroplasmia, this configuration of the maternal gametes appears to influence the severity of the disorder and the probability of recovering visual acuity. For this reason, genetic analysis in the families or diseased individuals may be expected to provide valuable prognostic information.
Inheritance of Leber hereditary optic neuropathy (Jacobi and coworkers 2001):
- point mutations in mitochondrial DNA
- in 7-30% of all patients in codon 3460, milder clinical courses
- in 50-76% of all patients in codon 11778, severe clinical courses
- in 10-31 % of all patients in codon 14484, better end-stage visual acuity
- normal and diseased women transmit the mutation to all male offspring and 8-15% of female children
- ratio of males to females who develop disease:
- 3460 mutation 2:1
- 11778 mutation 2.5:1
- 14484 mutation 5.7:1
- 3460 mutation 2:1
- heteroplasmia in families with Leber hereditary optic neuropathy
- with 3460 mutation, 40%
- with 11778 mutation, 6%
- with 14484 mutation, 36%.
- with 3460 mutation, 40%
Smoking is now recognized as a risk factor for the manifestation, severity, and end stage of Leber hereditary optic neuropathy. This is presumably due to the increased level of serum cyanide. Leber hereditary optic neuropathy usually occurs in both eyes in rapid succession. It begins with optic disc edema. Within a few weeks, visual acuity decreases sharply. Central or cecocentral scotomas are detectable in the visual fields. The optic discs then turn pale, initially on the temporal aspect and later entirely. The central visual field defects can increase in size. Both eyes are typically involved. Final values of 20/20-20/100 have been reported in those cases in which visual acuity recovered.
This disorder may initially be misdiagnosed as bilateral optic neuritis. However, the absence of neurologic or toxic symptoms leads to the correct diagnosis, which can often be confirmed on the basis of family history.
Treatment: there is no known effective treatment. However, patients should avoid toxic influences such as smoking. Vitamins Bl, B12, and B6 and zinc chelates can delay progression of the disease.
Blurring and Hyperemia of the Optic Disc in Hyperopia— Pseudopapillitis
Pseudopapillitis
Hyperopia is often encountered in small eyes with a short axial length of less than 21 mm. Especially in more severe hyperopia, the optic disc can appear reddish and prominent. The prominence is slight and hardly measures more than one diopter. With these findings, visual acuity, visual field, and function of the visual system are normal.
When in doubt, perimetry testing to exclude a neuro-ophthalmologic disorder should be performed in addition to evaluation of visual acuity and refraction.
Treatment: none.

Fig. 6.7 Optic disc in hyperopia (so called pseudopapillitis). Both optic discs are hyperemic, ill-defined, and smaller than normal with elevation measuring 1 diopter.
Blurred, Pale Yellowish Optic Discs—Optic Disc Drusen
Optic Disc Drusen
- ill-defined optic disc
- occasionally hyperemic
- deposits resembling grains of sago visible under retrograde illumination
- visual field defects
- visual acuity rarely reduced
- ultrasound or CT confirms diagnosis
Findings are often bilateral and include sparkling, yellow-gray, translucent deposits resembling grains of sago on the margins of the ill-defined optic discs. These changes may be mistaken for an optic disc edema progressing to optic nerve atrophy. These are drusen. They occur idiopathically or in conjunction with congenital diseases, although they may also occur unilaterally secondary to acquired neuritis or chorioretinitis. They can increase in size and cause compressive atrophy that leads to visual field defects. Often the visual fields are concentrically constricted, and the blind spot is enlarged.
For this reason, the patient should undergo neurologic examination and CT studies should be obtained. These latter studies confirm the diagnosis because drusen are visualized as sharply defined, high contrast, granular structures. They can produce a sharp echo on ultrasound images. Drusen exhibit the phenomenon of autofluorescence. Without fluorescein injection, they exhibit a luminous, yellow appearance in blue light.
Treatment: none.
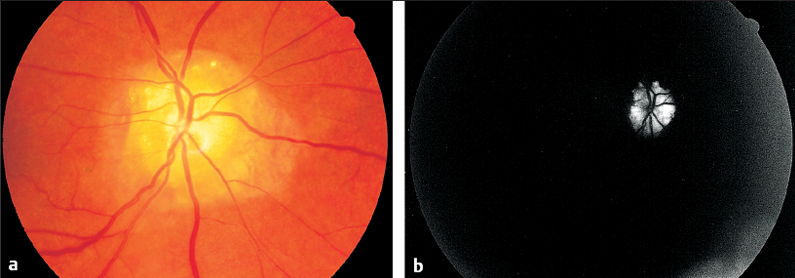
Fig. 6.8a and b Optic disc drusen.
a Ill-defined, large, bright, white drusen deposits. Bilateral findings.
b Autofluorescence.
Blurred, Hyperemic Optic Discs under Amiodarone Therapy
Changes in the Optic Disc under Amiodarone
In patients taking amiodarone for treatment of tachyarrhythmia, bilateral optic neuropathy is observed in addition to the well-documented whirl shaped corneal deposits. The onset of this optic neuropathy is insidious, and it gradually leads to irreversible visual field defects and diminished visual acuity. The optic disc appears blurred and hyperemic. The process ceases when amiodarone therapy is discontinued. Long-term amiodarone therapy leads to optic nerve atrophy.
Treatment: discontinue amiodarone therapy.
| Principal Signs | Important diagnostic studies | |
| Hyperopia >5 diopters Pseudopapillitis | Rarely >1 mm prominence No functional impairment | Visual field, refraction CT and MRI if indicated |
| Classic papilledema with increased cerebrospinal fluid (CSF) pressure | Prominence up to 4mm, radial bleeding may be present | Immediately: CT or MRI; look for brain tumor |
| Arterial hypertension | Constricted arterioles, hypertensive retinopathy | Measure blood pressure, kidney diagnostics |
| Idiopathic intracranial hypertension pseudo-tumor cerebri | Overweight women, age 20-40; transient obscurations, visual field loss high CSF pressure | Visual field, CSF opening pressure; emergency MRI; MR-angiography |
| Acute nutritional optic neuropathy tobacco-alcohol amblyopia | History, bilateral decreased visual acuity, vitamin B1 (thiamine) deficiency | Visual field, measure vitamin B1 in blood |
| Leber hereditary optic neuropathy | Bilaterally decreased visual acuity, history | Genetic analysis of families, follow up further course of disease |
 Unilateral Blurring of the Optic Disc with Hyperemia, Prominence, and Impaired Vision
Unilateral Blurring of the Optic Disc with Hyperemia, Prominence, and Impaired Vision
Three disorders exhibiting these symptoms must be differentiated from each other:
- anterior ischemic optic neuropathy (AION), which is attributable to arteriosclerosis
- arteritic anterior ischemic optic neuropathy (less common), usually referred to as temporal arteritis
- papillitis.
Arteriosclerotic optic neuropathy is common. Temporal arteritis is less common but involves characteristic symptoms. Papillitis is often difficult to distinguish from anterior ischemic optic neuropathy, especially in its arteriosclerotic form. Because each of these disorders requires a different treatment, it is important to promptly distinguish them from one another.
Anterior Ischemic Optic Neuropathy (AION) in Arteriosclerosis
Signs and Symptoms of Anterior Ischemic Optic Neuropathy in Arteriosclerosis (AION)
Synonyms:
- ischemic optic neuropathy
- nonarteritic anterior ischemic optic neuropathy.
This disease of the optic nerve usually occurs in older patients; the average age is 65. It is associated with a sudden decrease in visual acuity. Visual acuity drops to between 20/60 and 20/200, rarely lower. The visual field exhibits defects in the superior and inferior halves with a conspicuous horizontal limitation. Defects affecting an entire quadrant can also occur.
The pupil responds as in amblyopia. The optic disc is blurred, hyperemic, and slightly prominent (1-2 diopters). Initially, it is not easy to distinguish anterior ischemic optic neuropathy from optic neuritis. Fluorescein angiography shows exudation of fluorescein dye from the optic disc and deranged retinal microcirculation with prolongation of arteriovenous passage time from 1.5 to 2.6 seconds. However, it does not provide a sufficient basis for a differential diagnosis. The ischemic lesion affects the minor branches of the vessels supplying the optic nerve that arise from the central retinal artery and the circle of Zinn. The latter is supplied by the network of short ciliary vessels. Arteriosclerotic changes in the vessels of this region presumably figure prominently in the etiology of the disorder.
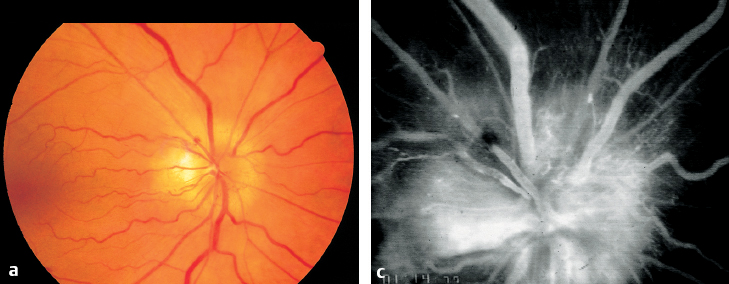
Fig. 6.9a-c Optic disc of a 50-year-old man with arteriosclerotic anterior ischemic optic neuropathy (AION).
a Ill-defined and hyperemic with elevation measuring 2 diopters.
c Fluorescein angiography demonstrating irregular hyperfluorescence.
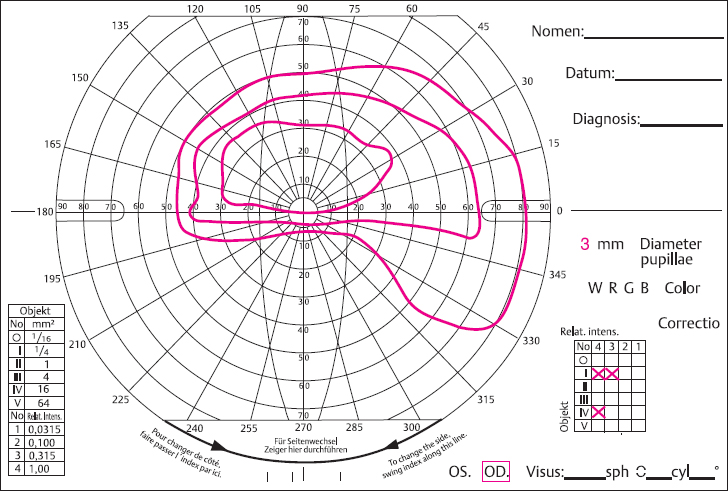
Fig. 6.9b Visual field: the horizontal limitation of the scotoma is indicative of the diagnosis.
Risk factors in arteriosclerotic anterior ischemic optic neuropathy:
- advanced age (50-80 years)
- arterial hypertension (55% of all patients)
- diabetes mellitus without retinopathy (23% of all patients)
- hypercholesterolemia (36% of all patients).
The chances that the optic nerve will recover under therapy are slight. Within the first 12-24 hours, there is hope of recovering at least certain areas of the visual field. Central acuity often cannot be restored. Often the fellow eye will develop the disorder with identical symptoms within a few weeks or months.
Treatment: immediate hemodilution is indicated. If arteritic anterior ischemic optic neuropathy cannot be ruled out, intravenous corticosteroids are initially indicated as well.
Temporal Arteritis (Giant Cell Arteritis)—Arteritic Anterior Ischemic Optic Neuropathy—Horton disease
Signs and Symptoms of Anterior Ischemic Optic Neuropathy (AION) in Temporal Arteritis
- patients usually over 65
- decrease in visual acuity within a period of hours
- nearly total loss of visual field
- temporal headache
- pale optic disc edema
- constricted retinal arterioles
- poor prognosis, imminent blindness
- temporal artery pulseless
- very high erythrocyte sedimentation rate (ESR)
- history of pain when chewing and shoulder pain associated with polymyalgia rheumatica
- temporal artery biopsy shows giant cells
This disorder is attributable to giant cell arteritis. As in arteriosclerotic anterior ischemic optic neuropathy, it usually affects older persons above the age of 65. Arteritic anterior ischemic optic neuropathy progresses far more rapidly than the arteriosclerotic type. Left untreated, it causes blindness within hours or days. Visual acuity decreases to the point where the patient can only perceive hand motion within a few hours. Patients suffer from severe headaches, especially in the temples. The optic disc appears edematous and is usually already pale. The retinal arteries are constricted. Often central retinal artery occlusion will be present with an ischemic edema.
The temporal artery is palpably thickened and lacks a pulse. The erythrocyte sedimentation rate is greatly increased. The prognosis for visual acuity is extremely poor.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


