Ophthalmoscopic Structure of Fundus Vessels
Retinal Blood Vessels
- terminal arteries and veins
- directly visible
Dimensions
- arterioles
- venules
- precapillary vessels
- capillaries normally not visible
Choroidal Vessels
- shimmer through pigment epithelium
- short arterial trunks
- network of capillaries with formation of lobules
- drainage via vortex veins
Ophthalmoscopic Visualization of Blood Vessels
- visible column of blood indicating vascular lumen
- arterioles exhibit bright reflex
- vessel walls are not normally visible
- pathological changes produce irregular reflexes and wall contours
The retinal arterioles appear as bright red bands with a longitudinal, centered gold reflex. The venules are homogeneously dark red, and their reflex is not as pronounced as that of the arterioles. Only the column of blood is visible in normal vessels; the wall of the vessel is visible only if pathologically altered. The bright reflex of the arterioles provides a visual impression of the vessel wall. Choroidal vessels are only visible where the retinal pigment epithelium (pigmented layer) is thin or exhibits defects. In such cases, the examiner will see the homogenous, red “carpet” of the choriocapillaris. If that structure is atrophic, the network of larger choroidal vessels becomes visible. Choroidal arteries and veins are indistinguishable from one another.
| Arterioles | Venules | |
| Course on fundus | Tor tuous Straight | Tor tuous Straight |
| Vessel width or caliber | Wide–narrow (relative to venules) Uniform–variable width | Congested/ wide–narrow Uniform–variable width Varying caliber |
| Reflex on arterioles | Wide–narrow Bright–dull Variable width–irregular | |
| Arteriolar branching | Acute angles Obtuse angles Horseshoe-shaped | |
| Terminal vascular bed | Minimally visualized, narrow, well filled |
 Variants in the Course of the Retinal Vessels
Variants in the Course of the Retinal Vessels
 Cilioretinal Artery
Cilioretinal Artery
Often a medium to large vessel will be seen to arise separately from the margin of the optic disc (usually temporally) instead of from the trunk of the central vessels. Its reflex identifies it as an arteriole. This vessel supplies a circumscribed area of the retina independently of the central retinal artery branches. Its early filling on angiography, before the retinal arterioles, is evidence of its origin from the choroid or ciliary vessels. This anatomic variant becomes clinically significant in occlusions of the central retinal artery because the area of the retina it supplies remains intact (Chapter 3).
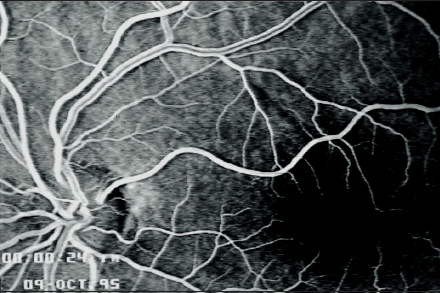
Fig. 4.1 Cilioretinal artery.
 Atypical Branching of the Retinal Arterioles
Atypical Branching of the Retinal Arterioles
Such vascular configurations are conspicuous. For example, superior and inferior arterioles may be seen to arise from a common trunk at the optic disc to form the temporal vascular arcades.
Telangiectasia
- red dots on the retina
- fluorescein angiography: slight exudation
 Retinal Vessels in Macular Aplasia
Retinal Vessels in Macular Aplasia
Hereditary aniridia is often associated with congenital malformation of the posterior pole of the eye in which the macular structure is absent. Therefore, there is no avascular zone in the central fundus. Accordingly, the perimacular vessels converge further.
 Abnormal Vessels in the Retina
Abnormal Vessels in the Retina
 Telangiectasia
Telangiectasia
These vessels appear in the retina as red spots. On fluorescein angiography, such vessels may exhibit exudation, which makes it difficult to distinguish them from abnormal neovascularization. They should be interpreted as congenital variants only in children. Later in life, both local retinal ischemia with hard exudates and neovascularization may develop from such congenital malformations of the minor vessels.
Treatment: laser photocoagulation may be performed if bleeding is imminent or larger hard exudates occur.
Leber Miliary Aneurysms
- irregular size of vascular ectasia
- hard exudates in their vicinity
- fluorescein angiography: veins and aneurysms highly permeable for fluorescein dye
 Multiple Leber Miliary Aneurysms
Multiple Leber Miliary Aneurysms
Treatment: as above.
Solitary Retinal Macroaneurysms
- saccular dilatations of varying size in the major vascular arcades
- envelope of connective tissue occasionally present (differential diagnosis: hemangioma)
 Solitary Retinal Macroaneurysms
Solitary Retinal Macroaneurysms
These appear as circumscribed vascular convolutions or saccular dilatations, often along the major vascular arcades. They attain sizes ranging between the diameter of an arteriole and the diameter of the optic disc. They are occasionally enveloped in connective tissue, assuming the form of a hemangioma. Aneurysms of the retinal vessels become clinically significant where they give rise to bleeding into the vitreous body. Then they are discovered only after the bleeding has been reabsorbed or on vitrectomy.
Treatment: 1aser photocoagulation or cryotherapy. Local radiation therapy with ruthenium 106 (106Ru), rhodium 106 (106Rh), or iodine 125 (125I); or proton beam therapy may be required for larger hemangiomas.

Fig. 4.2a and b Intraretinal angioma (cavernous retinal hemangioma). a Ophthalmoscopic findings.
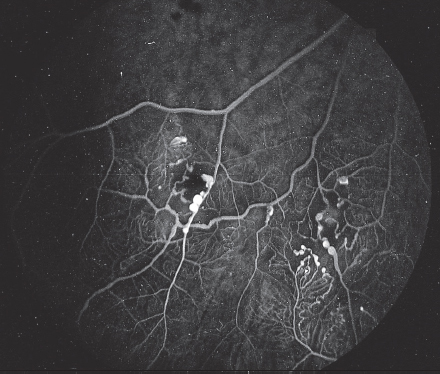
Fig. 4.2b Fluorescein angiography.
Angiomatosis Retinae (Von HippelLindau Disease)
- Prevalence: 1:40000 individuals
- manifestation at age 10–50
- vascular tumors on the fundus
- gray–red saccular dilatations
- vascular convolutions
- fibrotic, highly vascularized tissue
 Angiomatosis Retinae (Von Hippel–Lindau Disease)
Angiomatosis Retinae (Von Hippel–Lindau Disease)
Heridity of angiomatosis retinae:
- autosomal dominant inheritance
- over 300 reported mutations of the VHL gene
- mutations in three exons
- missense, nonsense, deletions, and abnormal splicing.
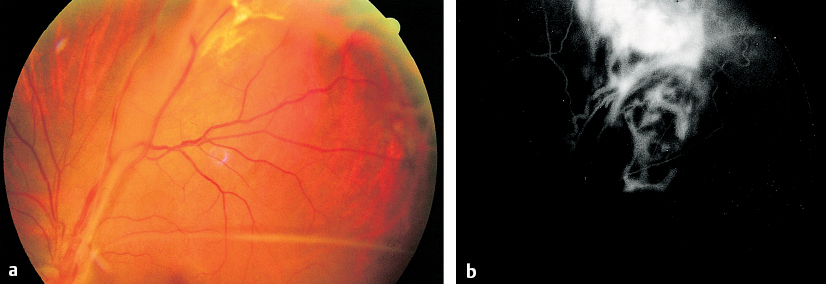
Fig. 4.3a and b Angiomatosis retinae. (von Hippel–Lindau disease) a Large vessel in the superior periphery supplying the tumor. b Fluorescein angiography.
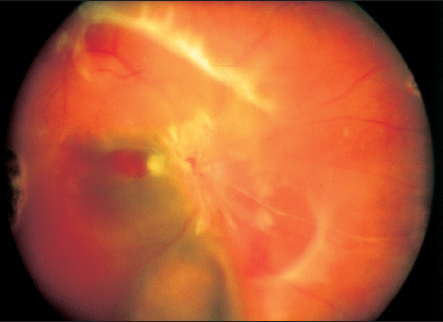
Fig. 4.4 Final-stage of angiomatosis retinae (von Hippel–Lindau disease). Fibrotic angiomas on the optic disc. Both eyes of this 28-year-old woman are blind.
Complications of angiomatosis retinae:
- vitreous hemorrhage
- tractional retinal detachment
- blindness at age 10–20
- precautionary examinations beginning at age five in genetic carriers
- other tumors are often present
- hemangiomas often also present in the cerebellum
- renal carcinomas
- pheochromocytomas.
- hemangiomas often also present in the cerebellum
Treatment: see p. 129.
 Rarefied and Elongated Vessels
Rarefied and Elongated Vessels
The walls of the central retinal artery are highly muscular and readily respond to stimuli with spastic constriction. As elsewhere in the body, arteriosclerosis in the retina and choroid is characterized by fibrotic hyaline degeneration of the vascular wall, particularly in the media. This constricts the lumen of the vessel. Often, age-related changes in the fundus are not clearly distinguishable from arteriosclerosis. In such cases, one must consider the patient’s age and possible systemic disorders.
Arteriosclerosis of the Retinal Vessels (Organic Pathological Vascular Changes) Arterioles
- straight course
- terminal vascular bed thinned
- irregular reflexes
- changes in caliber
Venules
- changes in caliber
- arteriovenous crossing signs
- Gunn, Salus, and Guist signs
Retinal Parenchyma
- poor reflexes
- dull, “dry” fundus
- drusen
Age-Related Involution on the Fundus
- reduced turgescence of the retina
- rarefaction of the retinal vessels
- choroidal sclerosis
- consider patient’s age to help differentiate from arteriosclerosis
- consider possible systemic disease
 Wide and Irregular Reflexes on Retinal Arterioles in Arteriosclerosis
Wide and Irregular Reflexes on Retinal Arterioles in Arteriosclerosis
In arteriosclerosis as well as with increasing age, the fundus loses its youthful shine. It appears dull and less reflective. Retinal turgor decreases, and the foveal reflex is often absent. Retinal vessels, which are visible through the column of blood they contain, appear thinner and elongated. The terminal vascular bed is less visible, and the vascular system appears rarefied.
Morphologic or organic changes in the vascular walls appear as irregular, usually constrictive marginal contours of the column of blood and irregular, usually widened reflexes on the arterioles.
Often the terminal branches of the venules exhibit increased tortuosity (Guist sign). Hyaline changes at arteriovenous crossings where the vessels share a common adventitia often lead to deformation of the venule, which appears visibly compressed. So-called crossing signs are visible where venules pass beneath arterioles; the contours of the venule narrow to a point, and widen on the other side of the crossing until original caliber is reached. This visual phenomenon is referred to as Gunn sign and is regarded as a symptom of retinal vascular arteriosclerosis. The crossing sign described by Salus, in which the venule crosses over the arteriole in a horseshoe shape, is also regarded as a sign of retinal arteriosclerosis.
Treatment: refer to family physician or internist.
 Choroidal Sclerosis with Bright Vascular Bands and Thin Columns of Blood
Choroidal Sclerosis with Bright Vascular Bands and Thin Columns of Blood
Signs in Ischemic Ophthalmopathy
- thin, minimally filled arterioles
- distended, tortuous venules
- ill-defined, pale optic disc
- linear and focal hemorrhages in the periphery
- cataract progressing to dense, white lens opacification
- frequently due to carotid artery stenosis
 Thin Vessels, Minimal Microvasculature, and Pale Fundus in Ischemic Ophthalmopathy
Thin Vessels, Minimal Microvasculature, and Pale Fundus in Ischemic Ophthalmopathy
In occlusion of the internal carotid artery, the resulting ischemia in the area supplied by the ophthalmic artery can lead to a well-defined clinical syndrome. Thin, minimally filled arterioles and distended, tortuous veins are visible on the fundus. These findings are often accompanied by linear and focal hemorrhages in the periphery. The optic disc is ill defined but usually pale. A cataract soon develops that progresses to a dense, white lens opacification within a few months. The rubeosis iridis present at this stage is a sign of the underlying disorder. Stenosis of the carotid artery can be diagnosed by Doppler ultrasound. These studies demonstrate the location and severity of the carotid stenosis as well as allowing estimation of its impact on hemodynamics.
Treatment: neovascularization is treated by laser photocoagulation or cryotherapy. Angioplasty or vascular surgery may be considered in the presence of carotid artery stenosis.
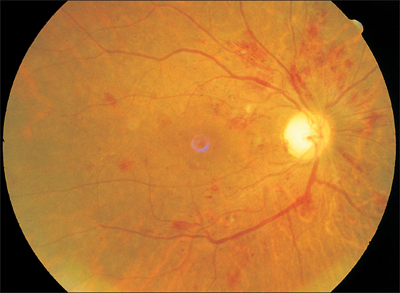
Fig. 4.5 Ischemic ophthalmopathy with pale fundus, rarefied vessels, and hemorrhages.
 Thin Vessels, Pale Fundus, and Occasional Retinal Bleeding in Anemia
Thin Vessels, Pale Fundus, and Occasional Retinal Bleeding in Anemia
These are signs of generalized anemia and should be taken into consideration in any evaluation of retinal vessels.
 Narrowed Arterioles and Congested Veins
Narrowed Arterioles and Congested Veins
Retinal Vessels in Arterial Hypertension—Hypertension due to Vascular Resistance
- vasoconstrictive narrowing of arterioles
- venules often distended
- clinical examples: toxemia of pregnancy, acute glomerulonephritis, pheochromocytoma
Hypervolemic Hypertension
- arterioles distended and tortuous
- caliber normal or widened
- venules distended and tortuous
- clinical examples: early stages of essential hypertension, stenosis of aortic isthmus
 Pathophysiology of the Retinal Vessels in Arterial Hypertension
Pathophysiology of the Retinal Vessels in Arterial Hypertension
Franz Volhard coined the phrase ‘the retina is a mirror of the kidney.’ Clinical experience has shown that the state of the retinal arterioles and parenchyma is an indicator of changes in the kidney, the brain, and the rest of the body.
Patterns of Retinal Vasculature Juvenile Vessels
- smooth, narrow column of blood
- arterioles exhibit bright reflexes
- tortuous vessels
Arteriosclerotic Vessels Identifiable by Changes in Vascular Wall
- straight course
- wide, bright reflexes
- irregular reflexes
- changes in caliber
Longstanding Arterial Hypertension
- vascular changes consistent with
- arteriosclerosis
- capillary ectasia
Fluorescein Angiography
- defects in the capillary network
- areas of nonperfusion
 Changes in the Retinal Vessels in Arterial Hypertension
Changes in the Retinal Vessels in Arterial Hypertension
The normal caliber of the arterioles in the fundus is two-thirds that of the venules. In the presence of arterial hypertension, the venules are often distended and tortuous, which can make it difficult to accurately gauge the caliber of the arterioles relative to the accompanying venules. However, arteriolar caliber is a decisive criterion for the evaluation of arterial hypertension. Generalized vascular constriction is recognizable by a narrowed column of blood. This limited caliber is not necessarily equally apparent in every portion of the vessel. A thinner column of blood without any further structural vascular changes is found particularly in young patients whose high blood pressure has not yet been present for a long time. Constriction in adolescent vessels and in the early stages of arterial hypertension occurs as a result of contraction of the muscles of the vessel (vasospasm). Decreased vascular caliber in the absence of visible structural changes should therefore be interpreted as vasospasm.
 Distinguishing Arteriosclerosis from Hypertension
Distinguishing Arteriosclerosis from Hypertension
Longstanding arterial hypertension over a period of months to years leads to structural vascular changes similar or identical to those in arteriosclerosis. Arterial hypertension is generally regarded as an important causative factor in arteriosclerosis.
Arterial hypertension in the elderly occurs in the presence of preexisting sclerotic changes in the retina. One simultaneously finds arteriosclerotic and hypertensive vascular changes. It is often difficult to distinguish fundus changes due to hypertension from those due to arteriosclerosis.
Findings in chronic hypertension include not only narrowed caliber of the arterioles but also wide, bright reflexes on the arteries. Irregular reflexes should be interpreted as structural arteriosclerotic changes. Hypertension is presumably the predominant factor if the caliber of the arterioles is narrower than one would expect in light of the existing structural changes in the vascular wall.
Hypertensive Fundus
- fundus appears well perfused and shiny
- capillary ectasia in green light
- hyperemia of the optic disc
- isolated minor hemorrhages
 Hypertensive Fundus
Hypertensive Fundus

Fig. 4.6 A 57-year-old man with essential hypertension. The image shows wide, bright reflexes on the arterioles and distended venules.
In arterial hypertension, the fundus is well perfused, glistening, and moist. The vasculature tends to be tortuous.
In addition to arterioles with limited caliber and bright reflexes, patients with hypertension develop capillary ectasia on the optic disc and in the vascular arcades. Capillaries are not normally visible. These distended capillaries suddenly appear in green light and occasionally will be seen to form networks.
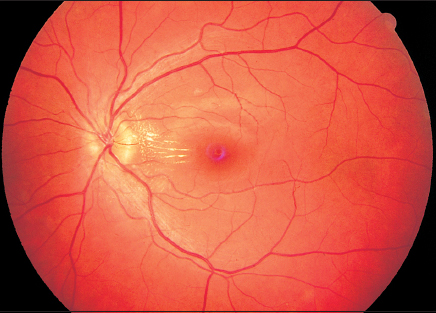
Fig. 4.7 A 23-year-old man with acute glomerulonephritis. Arterioles are narrowed, the optic disc appears ill-defined and hyperemic—hypertensive retinopathy.
Next, the margins of the optic disc become blurred and its parenchyma becomes somewhat hyperemic. These changes are clearly distinguishable from the sharply defined, usually pale optic disc in arteriosclerosis.
Other parenchymal changes include minor retinal bleeding, specifically spot hemorrhages in the middle layers of the retina. Often, linear hemorrhages will be observed in the nerve fiber layer.
Treatment: management of the arterial hypertension.
 Bleeding, Cotton-Wool Spots, Hard Exudates, and Retinal Edema
Bleeding, Cotton-Wool Spots, Hard Exudates, and Retinal Edema
 Hypertensive Retinopathy
Hypertensive Retinopathy
Severe parenchymal changes in the retina in arterial hypertension often manifest themselves in the vascular arcades as cotton-wool spots or soft exudates (p. 27) and as hard exudates or areas of fatty deposits (p. 22).
In arterial hypertension, the hard exudates often appear like focal calcifications around the macula, forming a macular star. Severe hypertensive retinopathy may be characterized by edema in the central retina and optic disc edema, which may be as pronounced as papilledema. As hypertensive retinopathy is invariably bilateral, a differential diagnosis should consider a cerebral mass or primary elevated cerebrospinal fluid pressure (cerebral pseudotumor). Often patients are subjected to extensive examinations in an attempt to confirm the latter diagnosis before the physician considers measuring blood pressure.
Hypertensive Retinopathy
- invariably bilateral
- cotton-wool spots (soft exudates)
- hard exudates (fatty deposits)
- macular star
- retinal edema
- retinal hemorrhages
- optic disc edema
- consider differential diagnosis of bilateral papilledema
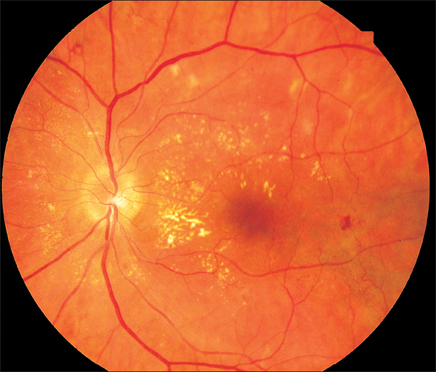
Fig. 4.8 Hypertensive retinopathy in a 38-year-old man showing narrowed arterioles, hard exudates, an incomplete macular star, and optic disc edema.
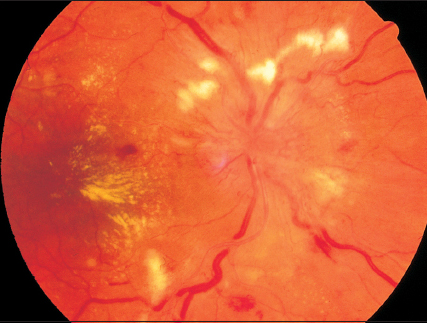
Fig. 4.9 Hypertensive retinopathy in a 45-year-old woman showing hard exudates, cotton-wool spots, hemorrhages, narrowed and stenotic arterioles, optic disc edema, and a surrounding retinal edema.
 Classification of Fundus Changes in Arterial Hypertension
Classification of Fundus Changes in Arterial Hypertension
To facilitate the interpretation of fundus findings, classification systems are used that divide hypertension into grades of severity. We prefer the Neubauer system, which is based on the earlier classifications of the ophthalmologist Thiel and the internist Volhard, and that of the American study group Keith, Wagener, and Barker.
Clinical diagnoses in hypertensive retinopathy:
- glomerulonephritis
- chronic renal insufficiency
- decompensated arterial hypertension
- toxemia of pregnancy
- pheochromocytoma.
Treatment : management of the arterial hypertension.
Stage I. Labile hypertension:
- normal or widened arteriolar caliber
- brighter reflexes on arterioles
- vascular distension and tortuosity
- no parenchymal changes
- arteriosclerosis of variable severity
- hypervolemic hypertension.
Stage II. Longstanding hypertension with elevated diastolic blood pressure:
- arterioles: generalized narrowing in caliber
- circumscribed areas of narrowed caliber
- increased and irregular reflexes
- paramacular venules distended and tortuous—sign of venous stasis
- precapillary vessels narrowed
- isolated capillaries visible (capillary ectasia) in central retina and on the optic disc
- hyperemia of the optic discs
- fine retinal hemorrhages
- occlusion of the central retinal vein frequently present.
Stage III. Malignant hypertension:
- generalized narrowing of the arterioles
- arterioles appear thin and threadlike in places
- vascular stenosis
- segmental or rosarylike constrictions
- bright and irregular reflexes
- Siegrist streaks and obliterated vessels
- capillary ectasia
- normal venules or venostasis
- cotton-wool spots
- hard exudates
- macular star
- retinal hemorrhages
- optic disc edema.
Stage IV. Severe uremic stage of malignant hypertension:
Retinopathy in Pregnancy
- bilateral
- optic disc edema
- arterioles, on the whole, are narrowed
- vasospasms
- cotton-wool spots
- exudate adjacent to retinal vessels
- retinal edema
 Stenoses of the Arterioles, Cotton-Wool Spots, and Retinal Edema in Retinopathy in Pregnancy
Stenoses of the Arterioles, Cotton-Wool Spots, and Retinal Edema in Retinopathy in Pregnancy
Some women develop arterial hypertension in the second half of pregnancy that can increase threateningly and even progress to eclampsia toward the end of pregnancy. Often the affected patients have a history of prior renal disease such as glomerulonephritis or pyelonephritis. Their diastolic blood pressure may exceed 100mmHg. Increased quantities of protein are excreted in the urine. Blood creatinine and urea levels are elevated.
Toxemia of pregnancy:
- headache
- nausea
- diastolic blood pressure exceeding 100 mmHg
- proteinuria
- elevated retention values
- visual impairments
- seizures.
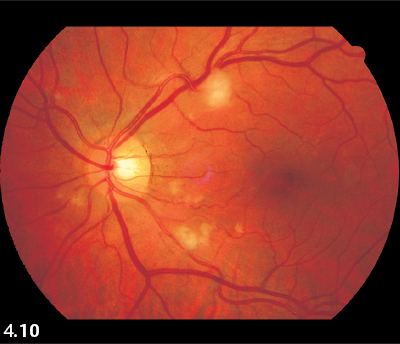
Fig. 4.10 Retinopathy in pregnancy in a 36-year-old woman. Narrowed arterioles, stenoses, and cotton-wool spots.
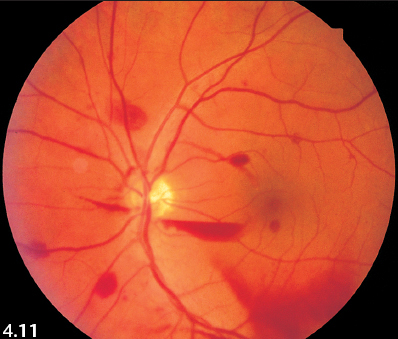
Fig. 4.11 Retinopathy in pregnancy in a 34-year-old woman. Vasospastic arterioles, retinal and preretinal hemorrhages.
The severe acute increase in blood pressure manifests itself as headache and nausea. Patients also complain of visual impairments.
Fundus findings in both eyes include optic disc edema and retinal edemas. These retinal edemas lie at the posterior pole of the eye and include the macula. Cotton-wool spots are found disseminated over the fundus, especially in the vascular arcades. Ill-defined veils are seen along the major vessels. These may be interpreted as paravenous exudations. Occasionally, minor retinal hemorrhages will also occur. The decisive finding that confirms the diagnosis is the caliber of the arterioles. The vessels in general are constricted and in many places exhibit genuine stenoses. The youthful vascular system of the pregnant patient lacks organic changes in the vascular walls. Therefore, the stenoses in the arterioles should be interpreted as vasospasms. Retinal findings are indicative of corresponding changes in the brain, which are presumably responsible for the eclamptic seizures.
Treatment: delivery of the child.
Purtscher Retinopathy (Traumatic Retinal Angiopathy)
- congestion and changes in caliber of the retinal venules
- hemorrhages
- cotton-wool spots
 Purtscher Retinopathy (Traumatic Retinal Angiopathy)
Purtscher Retinopathy (Traumatic Retinal Angiopathy)
Fig. 4.12 Purtscher retinopathy (traumatic retinal angiopathy) secondary to compressional trauma to the chest in a 52-year-old construction worker.
 Capillary Aneurysms, Hard Exudates, Bleeding, and Neovascularization
Capillary Aneurysms, Hard Exudates, Bleeding, and Neovascularization
Pathogenesis of Diabetic Retinopathy
- glycosylation of proteins
- hyperglycemia
- increase in intracellular sorbitol
- increased occurrence of AGEs (advanced glycation end products)
- increased oxidative stress
- increased activity of protein kinase C (PKC)
Pathogenesis of Diabetic Retinopathy
The chronic hyperglycemia in diabetes mellitus leads to glycosylation processes that cause vascular changes, initially in the capillaries (microangiopathy) and later in the larger vessels throughout the body (macroangiopathy). Major late complications of these changes include diabetic retinopathy, diabetic nephropathy, peripheral and central neuropathy, disturbed wound healing, and cardiovascular disorders. Type I and type II diabetics are equally affected.
Several biochemical mechanisms are involved in the pathogenesis of diabetic retinopathy. Elevated levels of blood glucose lead to a rise in intracellular sorbitol. Because sorbitol is only metabolized slowly, its intracellular concentration increases, causing osmotic cell damage with the formation of advanced glycation end products (AGEs). These AGEs are substances that cannot be further metabolized, and they form deposits in vascular walls and bond to protein molecules. This is the mechanism that causes diabetic microangiopathy. The elevated oxidative stress in the diabetic patient leads to increased quantities of reactive oxygen radicals, which damage the vascular walls, and also activate protein kinase C (PKC). This substance plays an important part in the microangiopathy induced by diabetic hyperglycemia.
Vascular damage—diabetic microangiopathy:
Clinical Findings in Diabetic Retinopathy
- microaneurysms
- cotton-wool spots
- ischemia (areas of nonperfusion)
- fatty degeneration of the retina (hard exudates)
- intraretinal microvascular anomalies (IRMAs)
- vascular proliferations arising from the retinal arcades and extending into the vitreous body
- retinal and vitreous hemorrhages
- rubeosis iridis
- tractional retinal detachment
These biochemical changes increase vascular permeability while simultaneously occluding the capillaries. Diabetic retinopathy is created by increased vascular permeability, which leads to retinal edemas and to diabetic maculopathy in particular. The progressive capillary occlusion causes retinal ischemia and stimulates neovascularization from which proliferative diabetic retinopathy develops. The changes of diabetic retinopathy can occur in the periphery of the fundus or in the central retina as diabetic maculopathy. However, the diabetic retinal changes usually develop more or less simultaneously throughout the fundus.
Diabetic retinopathy is divided into the following stages:
- nonproliferative diabetic retinopathy (NPDR)
- mild form
- moderate form
- severe form
- mild form
- proliferative diabetic retinopathy (PDR)
- diabetic maculopathy.
Nonproliferative Diabetic Retinopathy (NPDR)
Mild Form
- microaneurysms
- retinal hemorrhages
- hard exudates
- cotton-wool spots
Moderate Form
- findings as above but more severe
- venous beading
Severe Form
- all quadrants affected
- 4–2–1 rule
- IRMAs (intraretinal microvascular anomalies)
 Nonproliferative Diabetic Retinopathy (NPDR)
Nonproliferative Diabetic Retinopathy (NPDR)
Nonproliferative diabetic retinopathy (NPDR) is characterized by a combination of increased vascular permeability and leakage of plasma components, hemorrhages, lipid deposits (hard exudates), and progressive vascular occlusion. This latter symptom manifests itself as areas of nonperfusion and microinfarctions (cotton-wool spots) in the retina.

Fig. 4.13 Nonproliferative diabetic retinopathy (NPDR) with capillary aneurysms in a 62-year-old man.

Fig. 4.14a–e Nonproliferative diabetic retinopathy (NPDR) in a 26-year-old man. a Capillary aneurysms appear more clearly in red-free light.
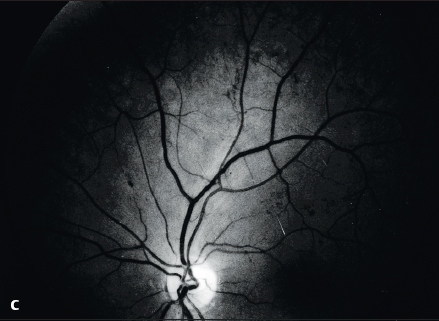
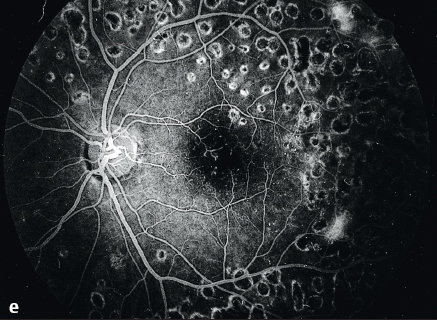
Fig. 4.14c Diabetic retinopathy seen in the same fundus one year later. Intraretinal microvascular anomalies (IRMAs) are now visible superiorly.
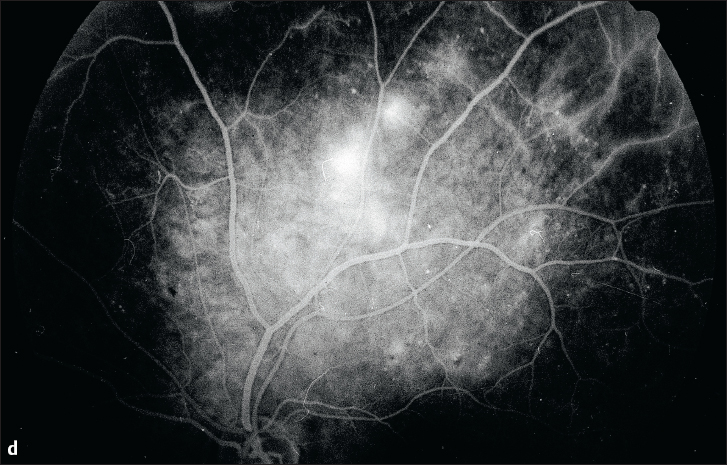
Fig. 4.14d Late phase of fluorescein angiography demonstrating exudation from neovascularization. Transition to proliferative diabetic retinopathy (PDR).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


