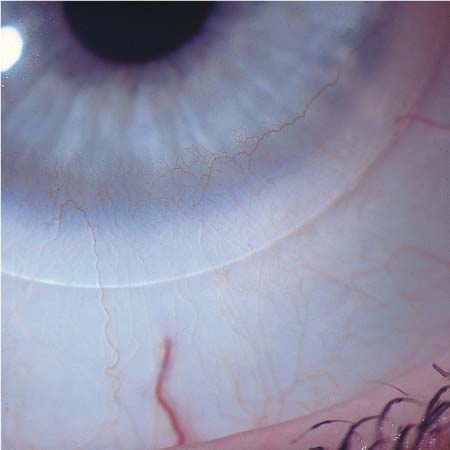
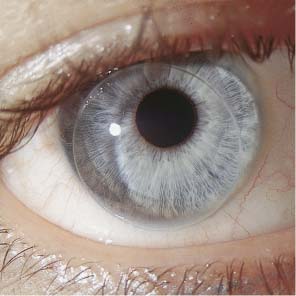
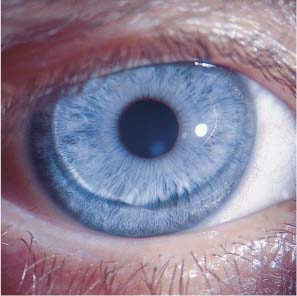
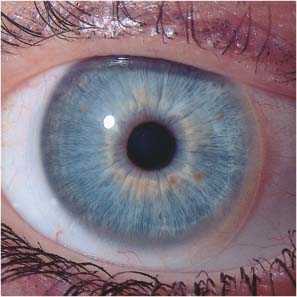
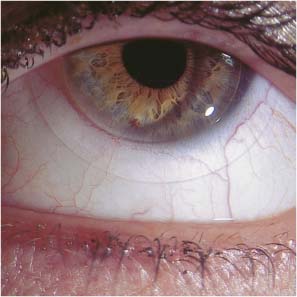
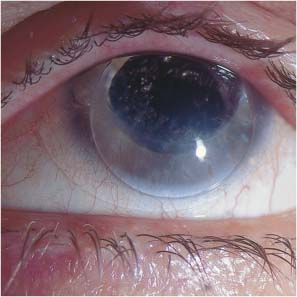
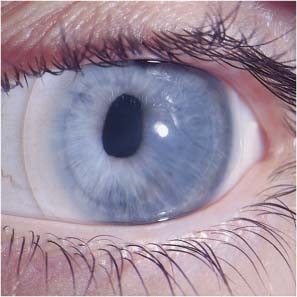
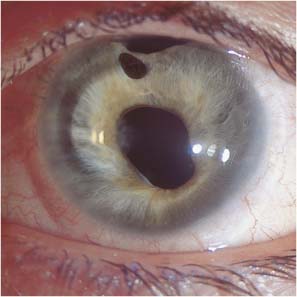
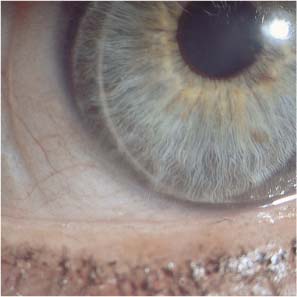
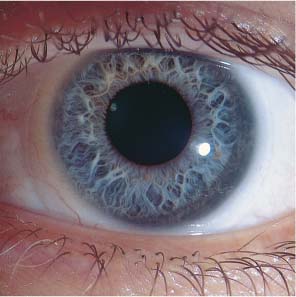
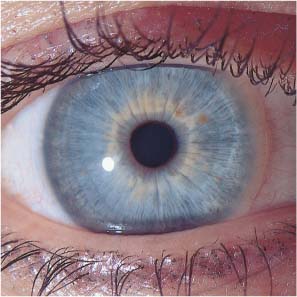
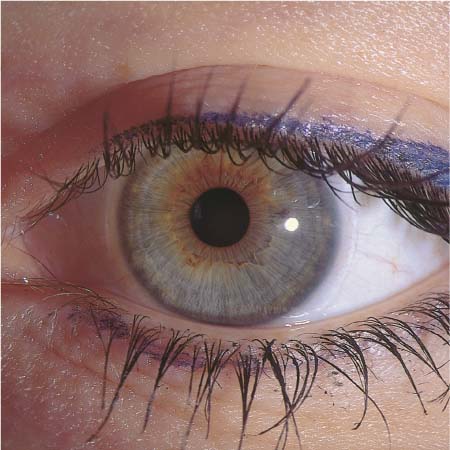
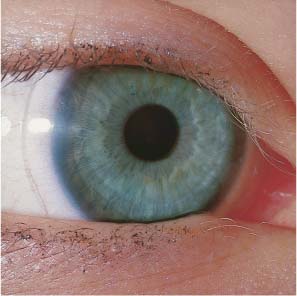
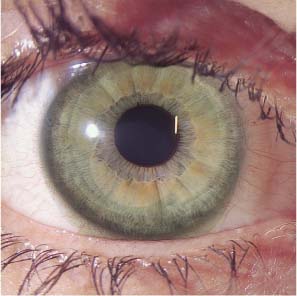
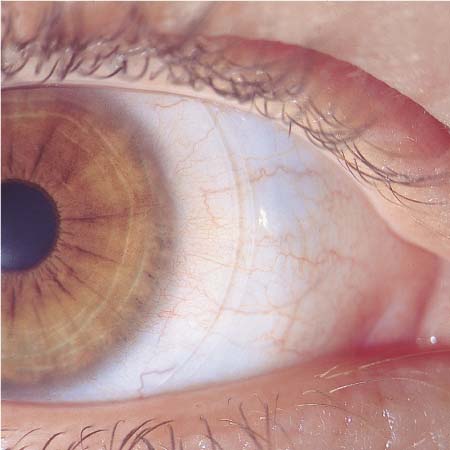
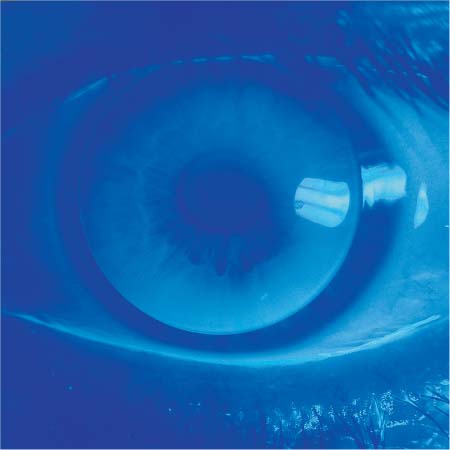
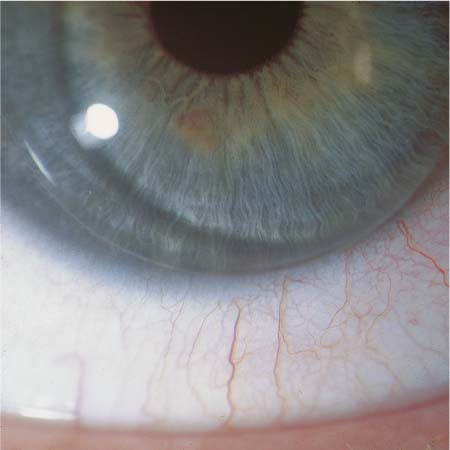
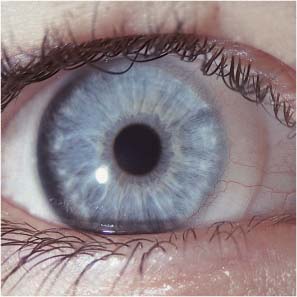
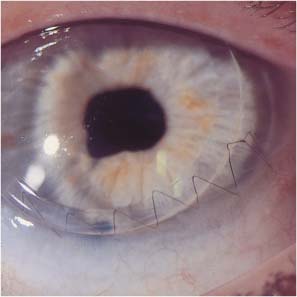
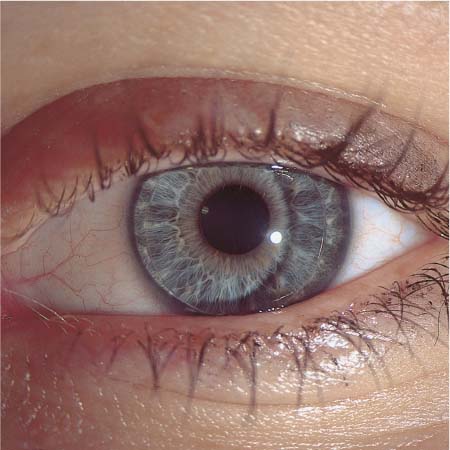
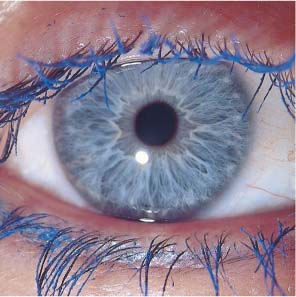
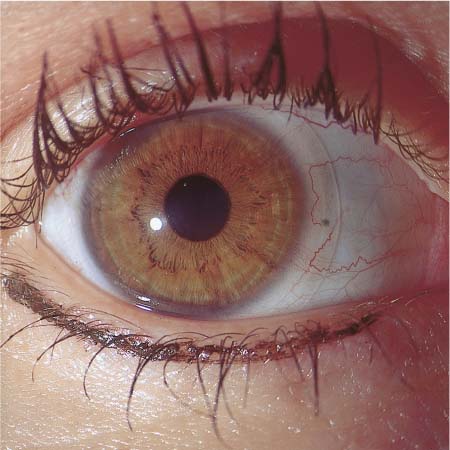
2 Patient Counseling and Examination Refractive Error and Visual Acuity Inspection of Contact Lens Cases All patients need thorough counseling and instruction before they choose the type of contact lenses they will wear and as they begin to wear them. The major issues to be addressed are listed in Table 5. The choice of contact lens is not simply a matter of finding the type that gives the best cosmetic result, as patients may at first assume, but requires consideration of patient-specific risks and other factors, particularly the patient’s living and working environment. Despite recent advances in soft-lens technology, hard lenses are still better tolerated over the long term, though hydrophilic lenses may be better suited to the patient’s lifestyle and desired manner of wearing. For patients who plan to wear contact lenses only occasionally, soft lenses are preferable; those who plan to wear contact lenses instead of spectacles over the long term are better served with hard lenses. Patients should be informed, however, that switching from hard contact lenses back to spectacles may be difficult. Long-term wearing of hard contact lenses can cause irregular astigmatism, leading to diminished visual acuity and increased glare; this is the so-called spectacle blur phenomenon. It often takes several months after the cessation of contact lens wear for these symptoms to resolve so that vision with spectacles is as good as before. Lens care products are to be regarded as medications, and due attention should be paid to their storage, stability, and expiration dates. Every contact lens wearer should be adequately instructed about their use, effects, and potential complications. The proper choice of lens care system depends not only on the type of lens, but also on the type and rate of deposition on the lens surface, which varies from patient to patient. Those for whom lens care is difficult, such as patients with arthritis, should use only one cleaning agent, if possible. Those with particularly sensitive eyes should use hydrogen peroxide. Careful consideration should be given to the possible use of an additional cleaning solution, or of enzyme tablets. The ever-decreasing cost of contact lenses and the introduction of disposable lenses have misled many wearers to imagine that contact lens optics is a routine matter, and that their purchase and use are a retail business like any other. Yet the fitting of contact lenses actually demands the highest expertise of the ophthalmologist and optician. Additionally, their physical specification and manufacture are an intricate technical process, at whose end the lenses can be safely handed over to the patient only when all of the problems discussed above have been resolved, unnecessary risks avoided, and possible contraindications ruled out. Finally, the prescriber of contact lenses must be certain that the patient can care for them properly and knows the problems that may arise with improper use. General reasons for wearing contact lenses Pros and cons of contact lenses vs. spectacles Problems in switching between contact lenses and spectacles Problems in the workplace Limited wearing time Lens handling, insertion, removal Lens cleaning Lens disinfection Frequency of replacement of short-term lenses Contact lenses and use of medication Contact lenses in patients with chronic illnesses Follow-up examinations by the fitter or ophthalmologist What to do in an emergency The patient’s past medical history and review of systems may indicate the presence of an acute or chronic illness that would increase the risk of wearing contact lenses. Such illnesses, a history of major trauma, and the chronic use of medications of certain types may contraindicate wear. The use of oral contraceptives, pregnancy, and breastfeeding are also limiting factors. The patient should be asked about prior ocular injuries, infections, other diseases, and the prior use of eye drops. If the data are available, the physician should also note any changes over time of the patient’s spectacle prescription, which may indicate a progression of the refractive error. Finally, the patient should be asked whether contact lenses were previously prescribed or worn, with what result, and why a previous fitting was unsuccessful, if this was the case. The tasks of the ophthalmologist include ocular examination before contact lens fitting, monitoring for potential problems in the initial adaptation phase, and regular follow-up thereafter. The routine ophthalmological examination of the contact lens wearer is the same as that of any other patient; its most important elements are listed in Table 6. Yet a few special considerations deserve mention in this section. Most problems due to contact lenses develop slowly and become manifest only after a variable interval. It is thus desirable to document the findings regularly with any of the numerous photographic and video systems now available for clinical use, with which the data may be digitally stored and statistically processed. The improved safety of modern synthetic materials and lens care products has greatly lessened the risks associated with contact lenses, but wearers must nonetheless be followed up regularly for the prevention of ocular damage, and particularly of slow, cumulative damage over the long term. General medical history, ocular history Lids Conjunctiva Cornea Sclera Anterior chamber Pupillary mobility Crystalline lens Vitreous body Fundus Visual fields Refractive correction (objective, subjective) Visual acuity Binocular vision Corneal diameter Corneal thickness Corneal topography Tear flow Intraocular pressure (in all patients over age 40 and those with progressive myopia, suspected glaucoma, or a positive family history) Ocular examination before, during, and after contact lens fitting thus serves not only for the immediate detection of acute complications, but also for the early detection of incipient long-term complications, which may affect either the anatomy or the physiology of the eye. We therefore recommend adherence to the classical sequence of the routine ophthalmological examination: visual acuity, motility, lids, conjunctiva, cornea, anterior and posterior chambers, retina, and intraocular pressure. Not only the eyes, but also the contact lenses should be examined. Any abnormalities of lens position, surface depositions, staining, defects, and changes in parameters should be noted. Microbiological tests may reveal poor lens hygiene and an elevated risk of infection. One should also try to determine whether the patient has a proper understanding of lens care. Dirty hands or a dirty lens case indicate that this is not so. Inadequate opening or closure of the eyelids, excessive blinking, or blepharospasm will be immediately visible to the examiner without special equipment. Ordinary daylight is best for examination of the lids. A check for symmetry readily reveals any monocular abnormality, such as ptosis. The normal interpalpebral space is almond-shaped and of equal height on the two sides. The lids snugly overlie the globe and point directly upward (lower lid) and downward (upper lid). The nasal canthus makes a sharp corner, while the temporal canthus is rounded. The lacrimal puncta are fully immersed in the lacrimal menisci. The skin of the eyelids is very thin and elastic, and care must be taken to avoid injuring it when spreading the lids apart to insert contact lenses, particularly in infants and toddlers. Children’s lids are soft and smooth, those of elderly persons baggy and wrinkled. Pathological changes of the lids are often the first sign of an adverse reaction to the lens itself, or to lens disinfectants or cleaners. The skin between the lashes should be examined carefully with a slit lamp under high magnification to detect early reddening and scaling. These findings mandate discontinuation of the contact lenses, as they are predictive of toxic keratopathy, which does not appear till much later. Particular vigilance is required in patients with a history of squamous blepharitis, which predisposes to such problems and is thus a relative contraindication to the wearing of contact lenses. The conjunctiva, an elastic, highly vascularized tissue lying in an exposed position between the globe and the lids, responds to all forms of irritation from within or without by vasodilatation, which is visible as conjunctival hyperemia (injection). This most common abnormal finding associated with contact lens problems often provides the key to their detection and differential diagnosis. Its location, extent, and type depend on the cause of irritation of the anterior segment, which may be mechanical, toxic, or metabolic, and may arise from the lens itself or from lens care products. The tarsal conjunctiva may display massive (follicular) swelling of the papillae in what is known as cobblestone conjunctivitis or giant papillary conjunctivitis (GPC). Zones of conjunctival necrosis are occasionally seen. Inspection of the conjunctiva of the upper and lower lids is thus mandatory not only before fitting, but also at every follow-up examination. Pathological changes of the bulbar conjunctiva range from simple injection to complex isolated or diffuse changes. The form and distribution of any perilimbal injection in the area covered by a soft lens are important clues to the differential diagnosis, as are superficial and deep conjunctival vasodilatation and neovascularization. A circular impression from the lens on the conjunctiva is an early sign of tight lens syndrome (TLS) and should be carefully inspected and documented, as should any microerosions or hemorrhages under the surface of the lens. Fluorescein or rose bengal staining is helpful. Fig. 1 Hard lens (PMMA), myopia, worn without problems for 20 years. Normal findings. Fig. 2 Soft hydrophilic lens (hydroxymethyl methacrylate: HEMA), myopia, worn without problems for 10 years. Normal findings. Fig. 3 Hard lens (fluorosilicone carbonate), high myopia, worn for 6 years without problems. Normal findings. Fig. 4 Hard lens, hyperopia +7.5 diopter (D), worn without problems for 8 years. Normal findings. Fig. 5 Absence of eye irritation, myopia, hard oxygen-permeable (RGP) CAB lenses worn for 8 years. Normal findings. Fig. 6 Absence of eye irritation, keratoconus, spheric equivalent –16.25 D, CAB lens worn without problems for 13 years. Normal findings. Fig. 7 Myopia, gel lens of high water content, worn without problems for 10 years. Normal findings. Fig. 8 Myopia –3.75 D, disposable lenses worn without problems for 5 years. Normal findings. Fig. 9 Absence of eye irritation, irregular astigmatism after photorefractive keratectomy (PRK). Piggyback system (hard lens on soft lens) worn for 3 years without complication. Fig. 10 Aphakia, irregular astigmatism, previous iritis, complication cataract operation with secondary glaucoma. Piggyback system worn for 2 years without complication. The cornea is inspected in the usual manner, with a slit lamp, before and after removal of the contact lens. First, the position and mobility of the lens are examined under low magnification. Tear lenses are more easily examined after instillation of a fluorescein solution of suitable type. Fluorescein sodium, which is water-soluble, must not be used with soft gel lenses, as it will bind to them and cause permanent staining. High-molecular-weight fluorescein preparations are now available for use with gel lenses, but their fluorescence is much weaker than that of fluorescein sodium. Rose bengal 2% is another useful dye for examination of the conjunctival and corneal epithelium after lens removal. Staining of epithelial cells may indicate a dry-eye condition associated with lens wearing. Rose bengal can bind to any type of synthetic material and thus is not routinely instilled when the contact lens is in place. Both fluorescein and rose bengal must be completely rinsed from the eye with sterile saline, and the lens should only be reinserted after a suitable interval, because even minute quantities of dye remaining in the conjunctival sac can stain it irreversibly. The location and extent of neovascularization at the limbus indicate whether a metabolic, mechanical, or toxic disturbance is present. These vessels are best seen with slit-lamp illumination at 10–20 × magnification under red-free light. Fine defects in the epithelium or stroma can be seen with a slit lamp at high magnification only; we recommend 30 ×. Examination of the endothelium requires either an additional noncontact optical device for magnification up to 200 ×, or an endothelial contact lens. The latter provides better optics but requires removal of the patient’s contact lenses, followed by the application of local anesthetic and coupling gel. Because these substances can damage the patient’s contact lenses, there should be an interval of at least 4 hours before reinsertion. The corneal curvature and thickness should be measured regularly, as they may slowly change under the gentle pressure exerted by contact lenses, whether hard or soft. Irregular astigmatism, occurring after years or decades of wear, can make returning to spectacles very difficult and may also impede refractive corneal surgery. A rapid change of corneal curvature is the result, either of an orthokeratological effect, or of flat fitting. Changes of corneal thickness imply an adverse mechanical and physiological effect of contact lens wearing. Fig. 11 Aphakia after bulbar perforation in a 4-year-old child. High (Dk) RGP lens +25 D, 3 months of problem-free wearing, corneal sutures in place. No sign of irritation. Fig. 12 Aphakia after early operation for congenital cataract, image obtained 3 months after surgery. Disposable lens of high water content, +38 D, absence of eye irritation. Fig. 13 Traumatic aphakia and astigmatism after perforating injury (stabbing). Soft lens worn without complication for 13 years, no ocular irritation. Fig. 14 Absence of eye irritation, aphakia, soft lenses worn without complication for 22 years. Fig. 15 Myopic astigmatism 7.0 D, truncated toric gel lens worn for 10 years without complication. Fig. 16 High myopia and astigmatism, scleral PMMA lens –29 D worn for 38 years without complication, no eye irritation. Fig. 17 Perforated bulb, traumatic aniridia, aphakia, and secondary glaucoma. Handpainted iris on gel lens worn for 9 years for cosmetic reasons. Fig. 18 Same lens as in Figure 17. Slightly dried surface, no other abnormalities, no problems with wear. Fig. 19 High Dk RGP lens for myopia –3.0 D, no irritation after 20 hours of wearing. Fig. 20 High Dk RGP lens for high myopia –17.0 D, no untoward findings after 19 hours of wear. Fig. 21 RGP lens after 18 hours of wear, fitted for keratoconus, no irritation. Normal findings. Fig. 22 Myopia –2.75 D, no irritation after 24 hours of uninterrupted wear. Fig. 23 Myopia –4.5 D, high Dk RGP lens after 30 hours of wear during air travel. Normal findings. Fig. 24 Soft lens for hyperopia +3.75 D after 28 hours of wear. No irritation. Fig. 25 Soft lens designed for month-long wear. Worn for 24 hours without problems after 30 days of use. Normal findings. Fig. 26 Gel lens, high myopia –30.0 D, worn for 20 hours. Normal findings. Fig. 27 Soft disposable lens after 30 days of use, no irritation after 42 hours of uninterrupted wear. Fig. 28 Blue-green tinted plano lens worn for cosmetic reasons, no irritation after 24 hours of uninterrupted wear. Fig. 29 Gel lens for myopia –3.25 D, tinted green for cosmetic reasons, no irritation after 10 hours of wear during a visit to a disco. Fig. 30 Extended-wear gel lens worn for medical reasons in the presence of chronically recurring corneal erosion. No untoward findings after 31 days of problem-free wear. Fig. 31 Soft hydrophilic lenses worn in piggyback mode (soft lens on another soft lens) to correct irregular astigmatism due to poor wound healing after an excimer laser operation. The patient was unable to wear hard lenses. The image, obtained after 21 days of wear, shows the absence of eye irritation. Fig. 32 High Dk RGP lenses, myopia –12.5 D, fluorescein instilled for photography, lens well fitted, problem-free wear for 6 years. Fig. 33 Same case as in Figure 32. The corneal topographic image shows no deformation of the anterior surface and stable corneal radii for the entire duration of wear. The contact lenses must be removed for examination of the interior of the eye, because contact lens shadows, particularly from lenticular lenses, may create misleading appearances. Moreover, mydriatic drugs instilled to enable retinal examination can bind to certain types of contact lenses and, as they are slowly released, produce an undesired mydriasis, which may last for days. The intraocular pressure (IOP) should be measured once or twice a year in all persons over 40, more often when there is a family history of glaucoma. The same applies to persons wearing contact lenses, particularly because raised IOP is a potential cause of corneal edema. Any sudden change in refractive error in a patient wearing either spectacles or contact lenses, increased glare, or altered contrast suggests the possibility of raised IOP. As these are also the classic symptoms of damage due to contact lens wearing, a careful differential diagnostic evaluation is needed. If doubt persists, perimetry may help. Just as in patients who do not wear contact lenses, the IOP is measured by applanation tonometry. The patient’s contact lenses must be removed before the instillation of local anesthetic and fluorescein. To prevent binding of these potentially toxic and lens-damaging substances, the reinsertion of hard lenses should be delayed for at least 20 minutes, that of soft lenses for at least 2 hours. Refractive error and visual acuity (VA) should be measured both subjectively and objectively, just as in patients wearing spectacles, and any change should prompt a search for the cause (see p. 128). The pressure exerted by a hard contact lens on the cornea can alter its topography (the so-called orthokeratologic effect). The corneal refractive power may be transiently altered and may not return to a stable value until weeks after the contact lens is removed. Measurement of the refractive error in the meantime may yield misleading results. Lenses fitted too steeply cause apparent worsening of myopia or improvement of hyperopia, while lenses fitted too flatly have the opposite effect. If the patient wants a pair of spectacles for brief, occasional use but plans to continue wearing contact lenses at other times, a prescription for average spherical values will be a satisfactory compromise. In patients who must stop wearing contact lenses because of incipient presbyopia, impending military service, or other reasons, the refractive error should be measured no less than 21 days after the contact lenses are removed, or else the spectacle prescription may turn out to be inaccurate. Any difficulty in finding the correct prescription should be dealt with by objective refraction, with and without contact lenses. Automatic refractometers cannot be used with certain types of lenses, for a variety of reasons. For example, the measuring beam may be of a wavelength that is reflected, rather than transmitted, by the lens material, so that the measured refractive error will be incorrect. A skiascope or manual refractometer will help in such cases. Good binocular vision requires that the eyes be parallel in primary gaze and have unimpaired motility. A patient who has good binocular vision while wearing spectacles will not necessarily have it while wearing contact lenses, even if they are optimally fitted. Movement of the contact lens over the cornea during lid opening and closure may impair image fusion, and the different accommodative effort needed when contact lenses are worn may bring out a latent or barely compensated strabismus. When a problem with fusion arises in a patient wearing contact lenses, and particularly in a hyperopic patient, the contact lenses should be suspected as the cause, and an orthoptic examination should be performed. A Pola test may also be helpful. Not only the patient, but also the contact lenses should be examined, as defective contact lenses frequently cause intolerable eye irritation and other complications. They are best inspected with a binocular dissecting microscope or a slit lamp fitted with a contact lens holder. All lenses should be checked for surface deposits, stains, cracks, tears, defects, and wavy deformations at their edges. Deposits on the lenses may be an early sign of ocular damage or systemic disease and should be carefully classified and documented. For the detection of defects, the slit lamp is not as good as a dark-field device developed by Zeiss for this purpose. Deviations of the geometric and optical parameters of the lens (diameter, thickness, curvature, refractive index) may be looked for under polarized light but are, in general, hard to detect without equipment that is too specialized for most practices. The position and movement of the contact lens on the cornea should be observed during vertical and horizontal eye movements, as well as lid opening and closure. The tolerance values for such movements depend on the type of lens. The contact lens case should be regularly inspected and its condition recorded. Dirty, leaky, or stained cases can cause ocular infection. Disinfectant solution may be less effective if there are air bubbles between the lens and lens case, if the well is incompletely filled, or if the fluid itself is discolored. Repeated topping-off of the disinfectant solution instead of emptying and refilling with fresh solution at each use may cause gradual accumulation of toxic substances, and, ultimately, toxic keratopathy. Proper evaluation of a corneal ulcer requires obtaining a swab for bacterial culture not only of the eye, but also of the lens case. A positive culture from the lens case suggests poor compliance with the recommended lens care routine. Not only is such a finding important for patient care, it may also benefit the ophthalmologist should the corneal ulcer become the object of a lawsuit. Ocular findings are most easily documented on the special file cards provided by contact lens manufacturers. More modern methods of data storage on videotape, computer diskette, or CD-ROM have the advantage of enabling retrieval of earlier slit-lamp images for direct visual comparison with current findings. Sometimes, newly detected pathological conditions will turn out to have been overlooked on earlier examinations. Patients can be registered by code number, and verbal descriptions can be stored along with the images. The video data can be digitized for electronic processing. In the future, the complete set of digitized images of each contact-lens wearer will be stored and evaluated by computer, and statistical analysis will yield information of both clinical and scientific interest. Even today, images are routinely transmitted over the Internet for assessment in centers with special expertise in the diagnosis and treatment of contact lens complications. Every new fitting of contact lenses should be preceded by an ophthalmological examination, so that the potential complications of lens fitting and wearing can be avoided. In fact, studies of unsuccessful fitting have shown that the cause of failure could often have been identified beforehand. Ophthalmologists agree that most serious complications can be prevented by examination of the patient before fitting to detect risk factors, and by more careful medical follow-up afterward. The preliminary and follow-up examinations must be conscientious and thorough, with attention not only to the eye, but also to the general medical history and review of systems. The proper timing and frequency of follow-up depend on the type of lens and mode of wear. Patients who wear their lenses only occasionally, as during athletic activities, need the least frequent follow-up, while, for example, visually impaired babies whose lenses will be in place for days or weeks at a time must be seen much more often. Newborns should be seen daily, and infants once every 1–4 weeks. The contact lenses should not just be checked but also cleaned in the laboratory, or exchanged, if necessary. Particularly in aphakic babies, the condition of the eye and the refractive index must be rechecked at short intervals, so that the geometric and optical parameters of the lenses can be properly adjusted. Follow-up visits can be more widely spaced as the child grows older. Once the age of 12 months is reached, follow-up can be once every 4–6 weeks, and later once every 3 months. The same frequency of follow-up is needed for adult wearers of extended-wear lenses. School-age children and adolescents should be seen every 3–6 months, depending on mode of wear; adults wearing hard or soft lenses should visit the ophthalmologist roughly twice a year, or once a year if they wear lenses only occasionally. Yearly examinations are needed in any case for glaucoma screening. Patients at high risk of complications, such as those with diabetes, allergies, or AIDS or those undergoing chemotherapy, should be seen more frequently, as should adolescents whose prescription is rapidly changing. Patients with seasonal illnesses, such as hay fever or corneal herpes (which worsen during damp periods), should be seen more frequently in the corresponding seasons.
Patient Counseling
History Taking
Examination
General
Lid
Conjunctiva


Cornea







Inner Eye
Intraocular Pressure
Refractive Error and Visual Acuity
Binocular Vision
Inspection of Contact Lenses
Inspection of Contact Lens Cases
Documentation of Findings
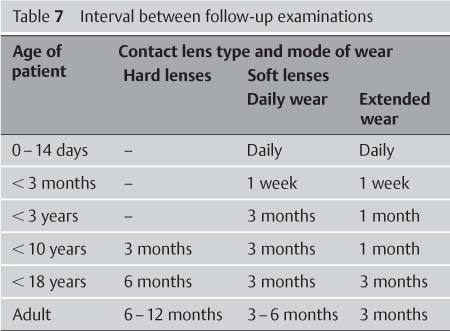
Follow-up


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


