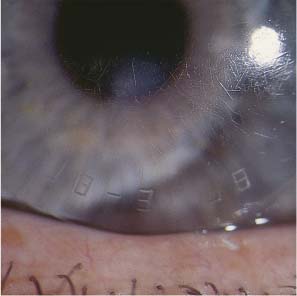
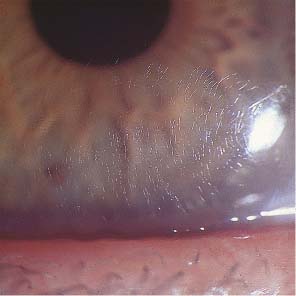
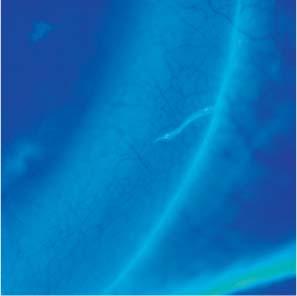
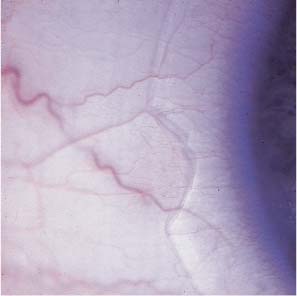
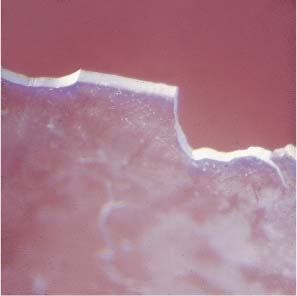
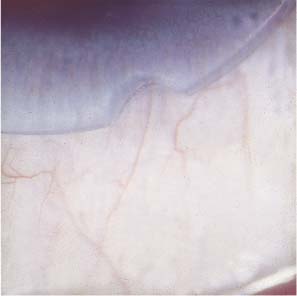
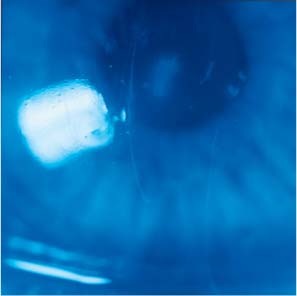
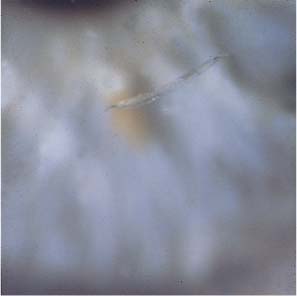
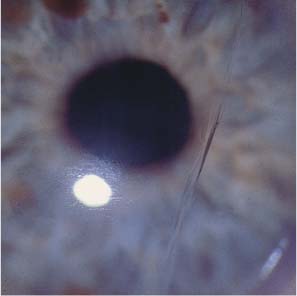
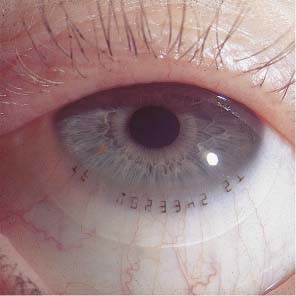
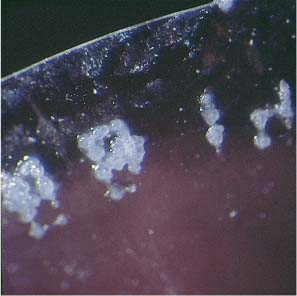
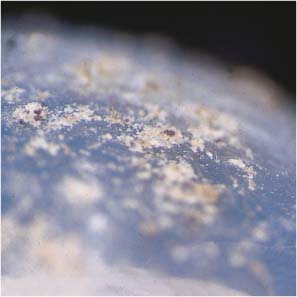
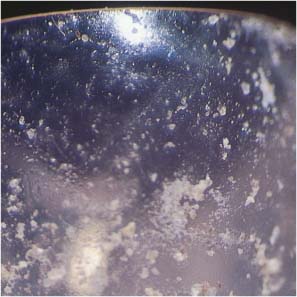
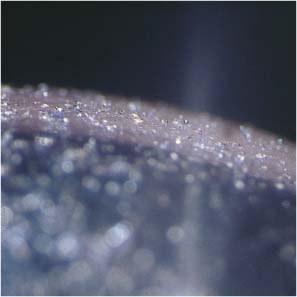
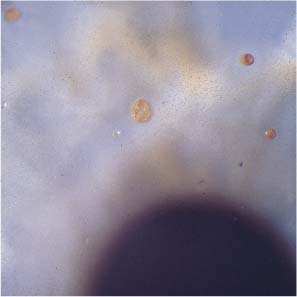
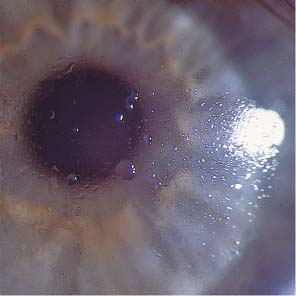
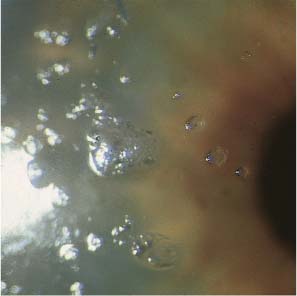
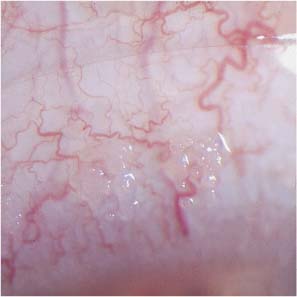
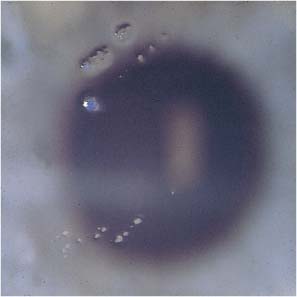
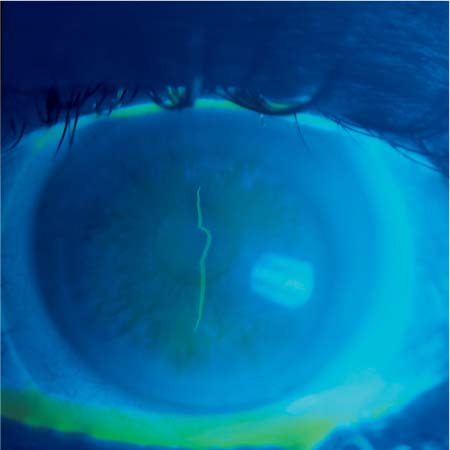
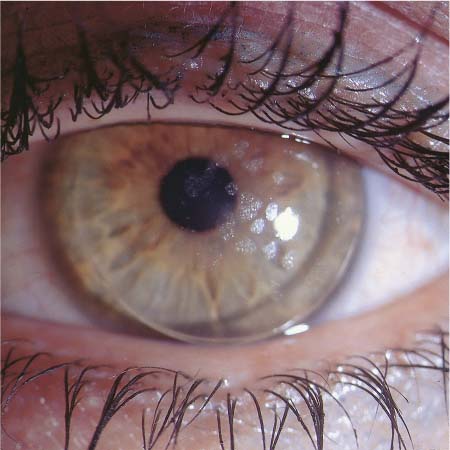
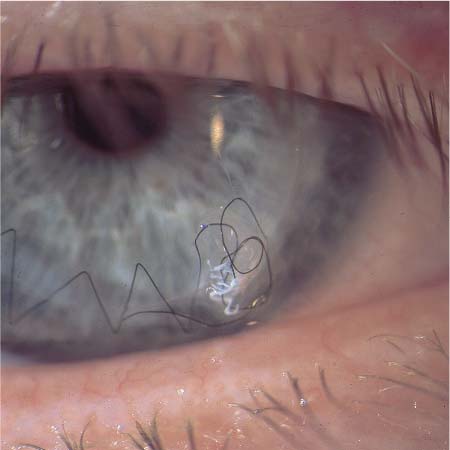
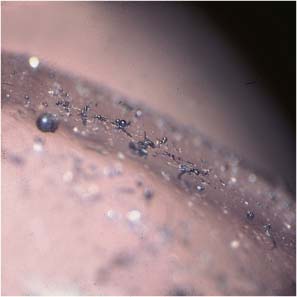
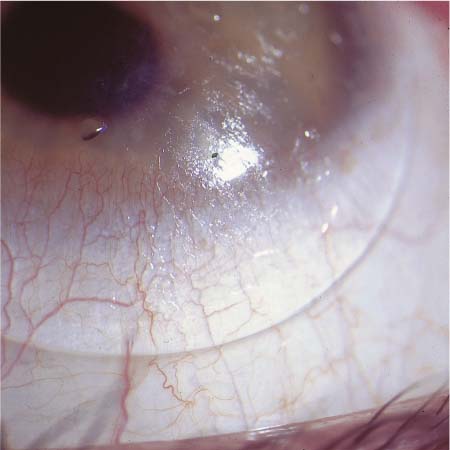
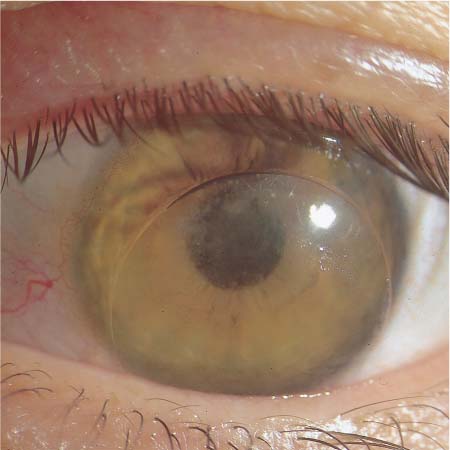
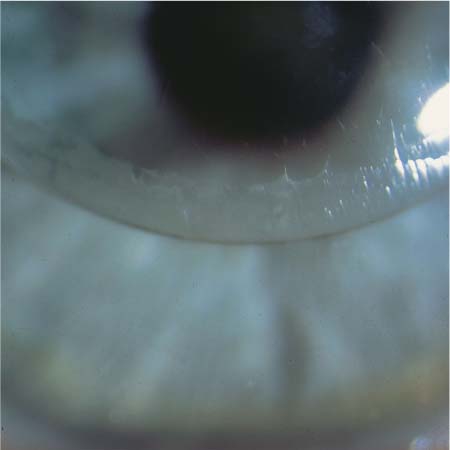
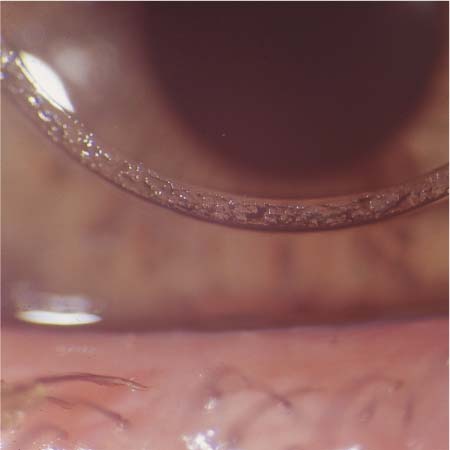
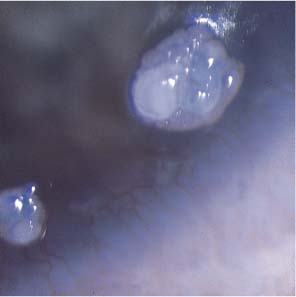
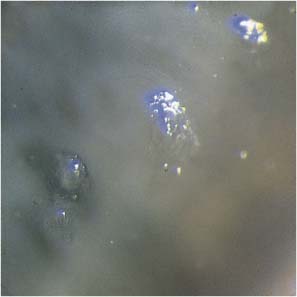
6 Alterations of Contact Lenses Symptoms: Fluctuations in visual acuity associated with blinking. Clinical findings: Inadequate wetting of the lens surface; abnormal break-up time (BUT) on the lens surface. Transient visual impairment associated with blinking implies a disturbance of wetting of the eye or of the contact lens surface. Glare is produced by cloudiness of the lens surface, the interior of the lens, or the refractive media of the eye. Visual impairment lasting 10–20 minutes after lens insertion in the morning may also indicate a wetting problem, as tear flow is normally less during sleep. Such problems can be dealt with by instillation of artificial tears upon awakening, before the physiological inflow of tears starts. Wetting the lens after insertion may also solve the problem. Impaired vision during the day accompanied by cloudiness or glare may be a sign of early corneal edema or giant papillary conjunctivitis (GPC); these conditions are readily diagnosed with the slit lamp. Visual impairment can result from disorders of lacrimation and the dry-eye syndrome. Any abnormality of the quality or quantity of tear fluid can impair vision in a contact lens wearer. Soft lenses need a reservoir of tears to retain their elasticity; hard lenses need a cushion of tears so that they can glide freely over the corneal surface. The tear lens between the contact lens and the cornea can only form if adequate tear fluid is present; the tear lens is an optical medium in itself and, depending on its geometry, serves as an additional plano, convex, or concave lens that cancels out small astigmatic errors. Thus, any change in the refractive index of the tear fluid, caused by fluctuations of its osmolarity, pH, or salt content, may affect visual function (cf. p. 128). A contact lens can be worn safely and comfortably only if its surface is smooth, that is, free of nicks, scratches, tears, sharp-edged defects, fracture lines, deposits, or foreign bodies. All of these abnormalities can cause an uncomfortable foreign-body sensation. Surface deposits serve as a culture medium for microbial pathogens and thereby promote infection. They also impair the wettability of the lens surface, which leads, in turn, to impaired vision and increased glare. Surface deposits must be removed from the lenses before each insertion, and defective lenses must be discarded. Patients wearing disposable lenses, in particular, should be reminded of these important facts at each follow-up visit, as these are precisely the patients that tend to wear their lenses much longer than recommended by the manufacturer. Defective contact lenses can injure the lids, conjunctiva, and cornea. Hyperemia or hemorrhage of the tarsal or bulbar conjunctiva, and corneal epithelial defects, are usually caused by wearing contact lenses past their wearable lifetimes. All contact lenses deteriorate over time and are therefore meant to be worn for a limited time only. Lens manufacturers do not guarantee their lenses for any specific length of time, but the general recommendation is that soft lenses should be worn for no longer than 1 year, hard lenses for no longer than 2 years. Contact lenses should be discarded at the end of their wearable lifetime and replaced with new ones. Disposable, oneday, and reusable lenses should be worn for no longer than 24 hours, a few days, and a few weeks, respectively. Patient compliance with these guidelines is, unfortunately, often suboptimal. Disposable lenses that have been worn too long are often broken, discolored, or deformed; fatigue fractures (stress lines) are seen in the lens matrix, the rim of the lens is broken or torn, and tenacious deposits are found on its surface. All of these findings indicate that the tolerance of the contact lens material for prolonged wear has been exceeded. Fine scratches on the anterior surface of hard lenses are only rarely disturbing; these can arise simply from the lens being worn in the eye, but may also be caused by mechanical cleaning with bare fingers. If the lens is well wetted, these defects are optically compensated for by the tear fluid, and are thus barely noted at first. They are disturbing only if they exceed a certain size so that they irritate the cornea or impair vision. If this occurs, it is time to replace the lens. Some types of highly gas-permeable rigid lenses are prone to the development of a mosaic pattern on their surface which resembles a smashed windshield. This change usually occurs after a relatively long period of wear; if it is found shortly after fitting, it is presumably due to a manufacturing error. Such patterns are probably created by too rapid cooling of the lens material in the polymerization process. At each follow-up visit, the contact lenses should be inspected under a dissecting microscope, or under a slit lamp with the aid of an inverting prism. The inspection can be performed in white light, but the use of polarized light will facilitate early detection of stress lines and other defects. Surface and edge defects are very reliably detected by Zeiss dark field examination in cold light. Fig. 317 Scratches on a hard CAB lens. Fig. 318 Scratches on a hard fluorosilicone carbonate lens. Fig. 319 Scratches on a hard PMMA lens. Fig. 320 Fine superficial cracks on a hard contact lens; aging of the material. Fig. 321 Scratches on a hard lens. Faulty cleaning and aging of the lens surface. Fig. 322 Central fracture in a worn-out soft disposable lens (worn for 16 months). Fluorescein stain. Fig. 323 Cracked edge of a 2-year-old soft contact lens. Fig. 324 Cracked edge of a high-Dk RGP lens, about 3 years old. Fig. 325 Sharp broken edge of a 4-year-old soft contact lens. Fig. 326 Edge defect in a soft contact lens; slit-lamp image, X30. Fig. 327 Horizontal tear in a soft lens of high water content, due to improper handling. Fluorescein stain. Fig. 328 Flawed edge of a soft lens of high water content, about 3 years old. Fig. 329 Edge defect in a 6-month-old disposable lens. Fig. 330 Y-shaped central crack in a soft hydrophilic lens, caused by faulty handling during lens cleaning. Fig. 331 Circular paracentral lens tear, caused by faulty handling during insertion. Fig. 332 Single-use soft contact lens; fluorescein staining; edge defect caused by faulty handling during insertion. Fig. 333 Fracture lines in a soft lens creating a stainable corneal epithelial defect. Fig. 334 Multiple edge fractures resembling a circular saw in a soft 1-month lens worn for 14 months. Fig. 335 Central fissures in a soft hydrophilic contact lens, caused by drying out and rehydration. Fig. 336 Fatigue fracture in a soft 1-month lens that was worn for 32 months. Fig. 337 Total opacification of a hard lens made of fluorosilicone carbonate, cause unknown. Fig. 338 Soft, disposable lens that broke after 1 hour of wear; manufacturing error. Fig. 339 Paracentral fissure in a rigid lens due to faulty handling. Fig. 340 Deposits on the surface of a hard lens, which has become hydrophobic; manufacturing error. Fig. 341 Cracks in a high-Dk RGP lens due to an error in tempering. Most contact lenses become discolored with wear because of a change in the molecular structure of the lens material over time. In general, soft hydrophilic lenses turn yellowish-brown after they have been worn for a number of years. The discoloration is harmless in itself but serves as a marker for an accompanying decline in gas permeability. Thus, discolored lenses should be replaced. Eye make-up in all colors is often found on the anterior surface of contact lenses and is not always removable. Lenses rinsed with tap water of high iron content develop a brown hue. The soft lenses of cigarette smokers are often stained reddish-brown to an extent that reflects how much they have smoked; those of firemen turn rust-brown after repeated exposure to the chemical substances liberated in fires (see Table 26). Lenses that have become discolored by external substances in this manner should be replaced, as the risk of toxic keratopathy from re-release of the adsorbed substances is difficult to assess. Patients at risk for such problems (heavy smokers, firemen, others) should wear disposable lenses. Oral, parenteral, or even topical medications can discolor soft contact lenses, particularly when they are used to treat ophthalmic diseases, such as recurrent corneal erosions or bullous keratopathy. Many different types of dyed and painted lenses are now commercially available; they are used to occlude the eye, to mask ocular birth defects or traumatic lesions, to reduce glare in aniridia or fixed mydriasis, or for elective cosmetic purposes. The last few years have witnessed the rising popularity of so-called party lenses with surface designs such as cat’s eyes, hearts, flowers, and dollar signs. The coloring of such lenses is not necessarily stable and may leach out of the lens to cause an allergic or toxic reaction. Color of staining Causes White, bright gray Proteins, lipids, mucopolysaccharides, calcium, jelly bumps, fungi, medications Dark gray, black Thiomersal, mercuric compounds Red Iron, fungi, tap water, medications Pink Vitamin B12, antibiotics Yellow Cosmetics, aging of lens material Brown Nicotine, fumes from fires, cosmetics, sprays Green Sorbic acid (a preservative), algae, chlorhexidine Blue Cosmetics Tinted, light-absorbing lenses are medically indicated in certain forms of retinal degeneration, and in albinism. They can also be worn for cosmetic purposes to change the color of the eye to blue, green, or brown according to the whim of the wearer. These lenses slowly fade over time; fading may be accelerated by the use of inappropriate lens care products, such as hydrogen peroxide, which acts as a bleach. It is not known with certainty whether the chemical dyes used could, in some circumstances, pose a risk to the cornea and conjunctiva. These substances should be remembered in the differential diagnosis of allergic and toxic reactions in the contact lens wearer; the Ophthalmotest may help resolve the issue (see p. 80). Fig. 342 Make-up residue on the surface of a hard lens. A typical instance of faulty cleaning. Fig. 343 Cloudy areas of a soft contact lens cleaned with an unknown household cleaner. Improper lens care. Fig. 344 Rust-brown staining of a CAB lens worn during a major fire in a chemical laboratory (responsible substance unknown). Fig. 345 Coloring of the engraving on a soft contact lens by eyeliner pigment. Fig. 346 Destruction of the surface of a hard lens by nail polish remover (contains acetone). Substances from the environment are deposited on the anterior surface of the contact lens. Solids, including foreign bodies, remain there, while liquids penetrate into the lens itself, and gases are dissolved in the tear film and transported by it around and into the lens. Only meticulous daily cleaning and disinfection can prevent long-term damage from such substances. Fig. 347 Broken suture after corneal graft. Wearing a soft contact lens; marked foreign body irritation. Fig. 348 Deposits on the irregular surface of a soft contact lens; dark-field image. Fig. 349 Jelly-bump-like residue of clear varnish in the engraving of a contact lens; dark-field image. Fig. 350 Metallic dust on a soft lens worn in the workplace without protective goggles. Fig. 351 Sawdust on a soft contact lens worn in a carpenter’s shop. Fig. 352 Deposits of molten metal on a hard contact lens worn by a welder without protective goggles. Fig. 353 Flour on a soft contact lens worn in a bakery. Fig. 354 Hairspray residue on the surface of a soft lens. Fig. 355 Metallic particles on the surface of a soft lens. Fig. 356 Soft lens perforated by a metallic splinter. Fig. 357 Iron spring embedded in the surface of a soft contact lens. Fig. 358 Rusted metallic foreign body at the edge of a soft contact lens. Fig. 359 Rusted metallic foreign body in a soft contact lens. Fig. 360 Rusted metallic foreign body in a soft contact lens. Fig. 361 Multiple rust-like deposits on a soft contact lens (Aspergillus niger). Not only environmental pollutants, but also components of the tear fluid leave their mark on the lens, as seen under the slit lamp. The tear fluid normally contains proteins, lipids, and desquamated cellular debris from the cornea and conjunctiva, all of which are deposited on the surface of the contact lens during the daily period of wear. If these deposits are allowed to accumulate, they can impair vision, increase glare, and mechanically irritate the eyelids, making lens wear uncomfortable (see p. 66). They can also decrease lens wettability and cause GPC. These organic deposits can also promote infection; kept moist by the tear fluid and the matrix of hydrophilic lenses, they serve as a bacterial and fungal culture medium. Dirty lenses confer a particularly high risk of infection. A special form of contact lens deposit has been termed the “sock phenomenon.” Proteinaceous deposits on the posterior surface of the lens can decrease its mobility by, in essence, gluing it to the cornea. The name is derived from the appearance of the deposits along the lens edges under the slit lamp (they are said to resemble socks on a clothesline). This phenomenon is rare, and its cause is unknown. Jelly bumps are small grayish-white deposits that appear to be spattered on the anterior surface of the lens. Microscopic or slit-lamp examination reveals their crystalline or onion-skin structure. They are hardly ever seen on the inner surface of the lens. They may appear singly or dispersed over the surface of the lens like stars in the night sky. Jelly bumps are commonly found on soft lenses, rarely on hard lenses. The water content and chemical structure of the lens material determine whether they will form. The more hydrophilic the lens, the more rapidly jelly bumps are deposited; deposition is also promoted by poor-quality material and by defects of the lens surface such as scratches, grooves, and polishing flaws. Jelly bumps make blinking uncomfortable because they irritate the lid margin. They are hard to remove and they recur rapidly if they are due to a structural defect of the lens. Such lenses should be replaced. Jelly bumps are composed of water-insoluble calcium–protein complexes. This explains both how they are generated and why they are so difficult to remove. In addition to the defective contact lens, the concentration of calcium in the tear fluid is another important determinant of their formation. Pregnant and breastfeeding women and those taking oral contraceptives develop jelly bumps more rapidly than others; so do patients with parathyroid disorders or hypercalcemia of other causes, as well as patients being treated with medications affecting calcium metabolism or high-dose hormones or oral antibiotics. In some cases, new jelly bumps can be seen as early as a few hours after lens insertion. There remains no effective way to prevent the formation of jelly bumps. Intensive cleaning, sometimes with highly concentrated cleaning solutions, is frequently recommended, but should in fact be avoided, because residues of the cleaning chemicals may be stored in hydrophilic lenses and may then interact with the patient’s lens care solution. Patients prone to the development of jelly bumps should avoid wearing highly hydrophilic lenses to minimize the risk of such problems. A switch to rigid gas-permeable (RGP) lenses or soft lenses with less than 40% content usually renders the patient asymptomatic. Because of the association between jelly bumps and disorders of calcium metabolism, patients with recurrent jelly bumps should have their serum calcium level determined. Any abnormality should be followed up with a general medical evaluation. Fig. 362 Dense proteinaceous deposits on a soft lens; poor lens hygiene. Fig. 363 Proteinaceous deposits on the surface of a worn-out hard CAB lens. Fig. 364 Lipid deposits on the anterior surface of a worn-out fluorosilicone carbonate lens. Fig. 365 Droplets of fat and protein on a hard contact lens; poor lens hygiene. Fig. 366 Protein coating on a soft contact lens; poor lens hygiene. Fig. 367 CAB lens densely coated with protein in an allergic patient during the hay-fever season. Risk of GPC. Fig. 368 Dense proteinaceous deposits on a 4-year-old soft contact lens. Fig. 369 Dense proteinaceous deposits on a 6-year-old soft contact lens. Fig. 370 Dense proteinaceous deposits on a soft contact lens; hydrophobic surface. Aging of the lens material. Fig. 371 Dense proteinaceous deposits on a soft contact lens; hydrophobic surface. Aging of the lens material, faulty cleaning. Fig. 372 Sock phenomenon; lens stuck to the cornea because of abnormal proteinaceous deposits. Fig. 373 Dense proteinaceous deposits on a soft contact lens; faulty cleaning. Fig. 374 Dense, sock-like proteinaceous deposits on the surface of a soft lens; sock phenomenon. Fig. 375 Proteinaceous deposits on a soft contact lens; faulty cleaning. Fig. 376 Proteinaceous deposits on a hard contact lens; poor lens care. Fig. 377 Proteinaceous deposits on the edge of an RGP lens, causing foreign body sensation. Fig. 378 Jelly bumps on a soft contact lens; surface damage; faulty cleaning. Fig. 379 Jelly bumps on a soft contact lens; faulty cleaning. Fig. 380 Jelly bumps on a soft contact lens; poor hygiene. Fig. 381 Jelly bumps on a soft contact lens; disorder of calcium metabolism. Fig. 382 Jelly bumps on a soft contact lens; developed after only a few days of hormone therapy. Fig. 383 Jelly bumps on a soft contact lens; material defect. Fig. 384 Jelly bumps on a soft lens of high water content; defective material. Fig. 385 Isolated jelly bump deposited on the defective surface of a soft contact lens. Fig. 386 Jelly bumps in the engraving of a soft hydrophilic contact lens. Fig. 387 Jelly bumps on a soft contact lens; tear deficiency; worn-out lens. Fig. 388 Jelly bumps on a soft disposable lens; tear deficiency; oral calcium supplementation; lens worn for 6 months. Fig. 389 Jelly bumps on a worn-out soft lens. Fig. 390 Jelly bumps on the defective surface of a worn-out soft lens.
Wetting Problems
Material Defects











Discoloration and Fading



Deposits







Components of Tear Fluid
Jelly Bumps






















Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


