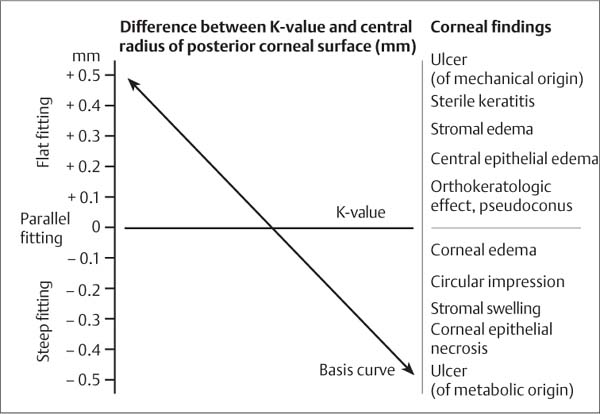
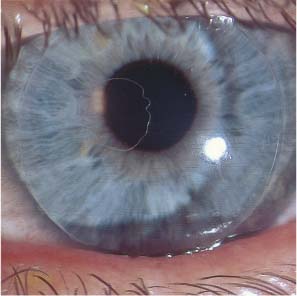
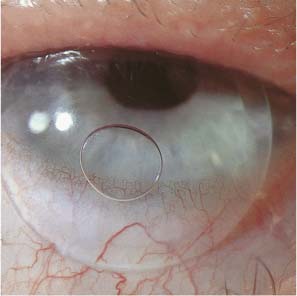
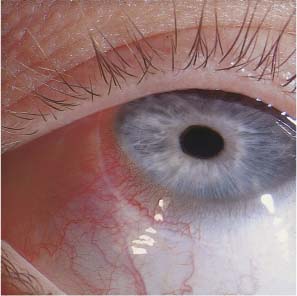
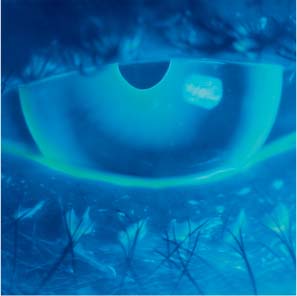
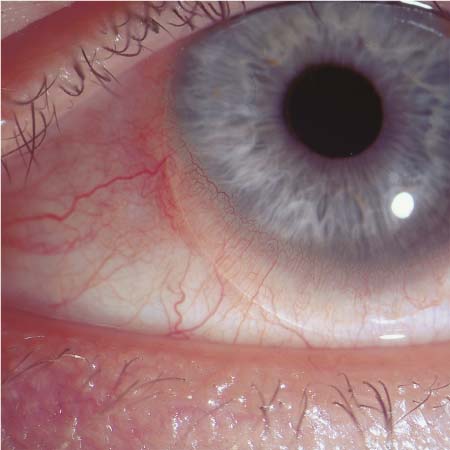
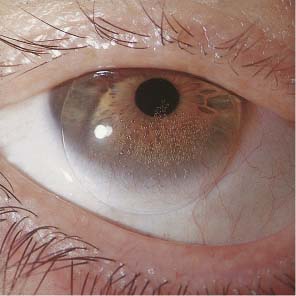
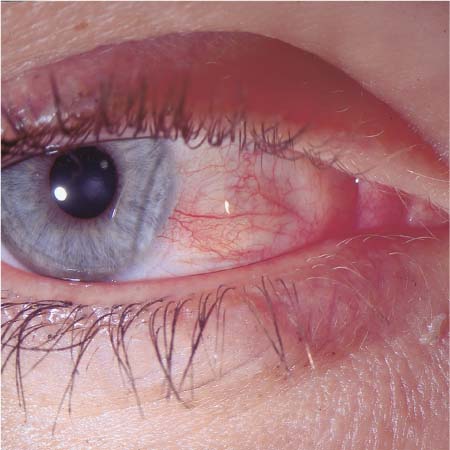
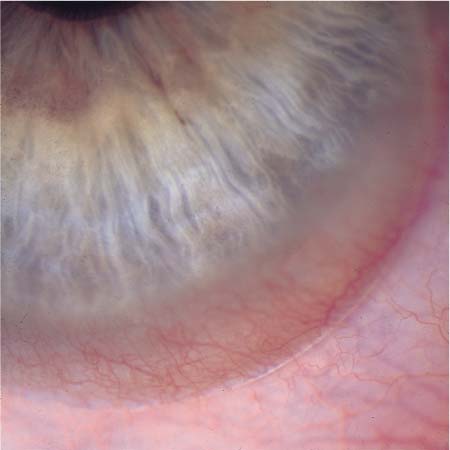
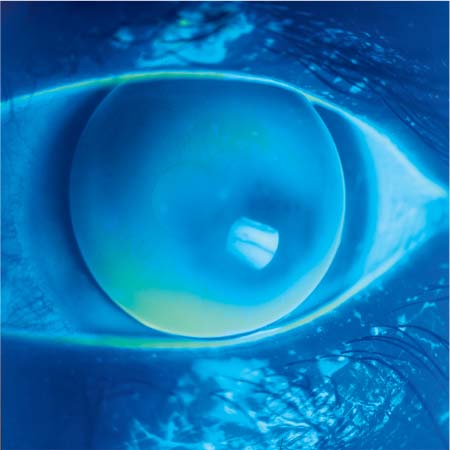
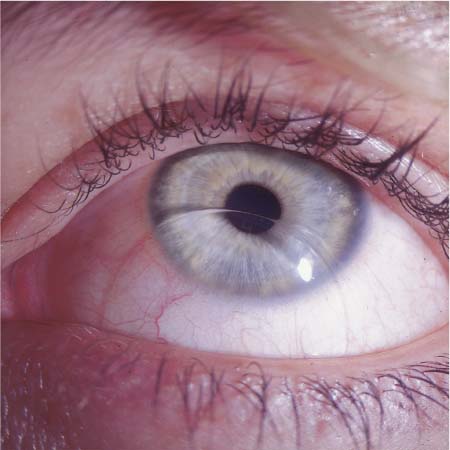
5 Causes of Contact Lens Damage Handling, Hygiene, Wearing Times Contact lens damage is usually due to faulty lens handling and hygiene. Patients must be advised of the need to clean and disinfect the lenses regularly. Serious infections of the conjunctiva and cornea are often caused by microbial pathogens that adhere to deposits on the surface of the contact lens. The contact lens fitter should note the state of the patient’s hands at the initial fitting visit, or indeed at the prefitting consultation. Long, sharp fingernails can not only damage the lenses but also cut the lids, conjunctiva, or cornea during lens insertion. Dirty fingers are vehicles of infection. Fungal lesions of the skin or nails indicate poor personal hygiene. Rheumatic changes of the fingers and hands may impede safe lens insertion and removal. Allergic changes on the skin imply that contact lens wearing may also be complicated by allergy. The lens case should be inspected at each follow-up visit. A dirty lens case implies that lens hygiene is probably deficient. Fingerprints on the lens case are, perhaps, tolerable, but actual dirt serves as an excellent reservoir for microbes that can then be transferred by the patient’s finger into the eye during lens insertion. A leaky case cannot assure sterility; bubbles or crystalline deposits inside the case implies that the patient is too sparing with storage solution and changes it too infrequently to assure adequate disinfection of the lenses. Cloudiness, streaks, or even visible remnants of lens deposits inside the lens case clearly indicate that the patient is not treating the lenses with the necessary care. Lens fragments or even several entire lenses swimming in the basin of the lens case indicate that the patient has been attempting to spare disinfecting solution. Inspection of the lens case yields a clear indication of the adequacy of the patient’s lens hygiene. Microbial cultures of the lens case are also advisable as an occasional screening test, and, of course, mandatory if any ocular complication should arise. Fig. 298 Sharp fingernails: a cause of corneal injury and resultant infection. Fig. 299 Hands of a farm worker who wore soft contact lenses and suffered from recurrent Pseudomonas infections of the eyes. Fig. 300 The lens case of a patient with a corneal ulcer. Note the proteinaceous debris in the storage fluid. Fig. 301 Very dirty lens from a patient with a corneal ulcer; positive culture for Pseudomonas. Fig. 302 Very dirty lens case of a patient with chronic conjunctivitis. Fig. 303 Soiled lens case of a construction worker; positive cultures for Pseudomonas and Staphylococcus from the surface and Aspergillus niger from the interior. The time a contact lens can safely remain on the eye is limited, as is the life of the lens itself. If a lens is kept on the eye for too long without interruption, it can cause corneal epithelial edema and an increase in pachymetric values, while the patient complains of increased glare (an important warning sign). Such findings imply that the metabolic tolerance of contact lens wear has been exceeded, and that the continued presence of the lens on the eye will be dangerous. Similar considerations apply to lenses worn past their useful life. Deposition of foreign matter in the interior of the lens and on its surface markedly decreases the oxygen permeability (Dk) of old lenses, leading in turn to diminished comfort and more frequent complications. The fitter must be aware of such problems and communicate them to the patient. It is particularly important not to exceed the recommended wearing time when contact lenses are worn for medical indications, for example recurrent corneal erosion or bullous keratopathy, which are treated with contact lenses that remain on the eye without interruption for days or even months. Overwear syndrome and tight lens syndrome are among the more common reasons why such treatments may be prematurely discontinued. Regular follow-up at short intervals and frequent changing of the lenses help prevent these problems. Poorly fitted lenses cause both mechanical and metabolic damage to the cornea, the latter because of impaired tear fluid convection and the resulting oxygen deficiency. Lens fitting must take the dynamic properties of the lens into account: the lens must be able to glide freely over the cornea during blinking, eye closure, and saccades. As shown in Illustration 9, a steeply fitted hard lens can produce a circular impression on the epithelium and a central corneal deformation. Flatly fitted lenses cause central corneal flattening and corneal thinning and may produce corneal distortion syndrome (see pp. 125, 126). Very flatly fitted lens can probably also cause various forms of keratoconus. Unproblematic long-term contact lens wear can only be assured by meticulous fitting and regular follow-up examination with the ophthalmometer or keratometer, or with computerized topography. Illustration 9 Types of corneal injury caused by faulty fitting of rigid contact lenses. The more the radius of curvature of the posterior surface of the contact lens differs from that of the anterior surface of the cornea (K-value), the greater the resulting corneal deformation. Flat fitting causes central flattening and thinning of the cornea, possibly leading to pseudokeratoconus; steep fitting causes central corneal hypoxia, possibly leading to tissue defects. Either type of faulty fitting can lead, in extreme cases, to destruction of the optical center of the cornea, and to corneal infection. Fig. 304 Soft contact lens fitted too steeply; compression of the limbal sulcus. Fig. 305 High-Dk rigid gas-permeable (RGP) lens fitted too steeply; paracentral air bubble in the tear lens. Fig. 306 Hard CAB lens fitted too steeply and caudally displaced; large air bubble under the lens. Fig. 307 Soft hydrophilic lens fitted too steeply and compressing the perilimbal conjunctiva. Fig. 308 Soft silicone lens fitted too steeply; pooling of fluorescein under the central part of the lens; bubble in the tear lens. Fig. 309 CAB lens for keratoconus, fitted too flatly; paracentral fluorescein-free area. Fig. 310 Soft PMMA lens in stage 2 keratoconus in unacceptable, decentered position (inferiorly displaced). Fig. 311 Hard contact lens for keratoconus, fitted too flatly; paracentral pressure area. Fig. 312 Soft silicone lens fitted too flatly and inferiorly displaced; conjunctival injection. Fig. 313 Hard lens for myopia; inferiorly displaced; fitted too steeply; air bubbles in the tear lens. Fig. 314 Hard lens for keratoconus fit extremely flatly; ring-like air bubble under the lens periphery. Fig. 315 Soft contact lens fitted too flatly and inferiorly displaced; excessive mobility on blinking. Fig. 316 Soft lens fitted too flatly and temporally displaced; focal irritation of the conjunctiva.
Handling, Hygiene, Wearing Times
The Patient’s Hands
The Lens Case




Wearing Times
Fitting Errors




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


