CHAPTER 144 Otosclerosis
Otosclerosis is a disease of bone that is unique to the otic capsule. It may cause a conductive hearing loss, a mixed conductive-sensorineural hearing loss, or occasionally a purely sensorineural hearing loss. In 1860, Toynbee1 first described the condition causing a hearing loss by fixation of the stapes. In 1893, Politzer2 referred to the fixation of the stapes as otosclerosis. Siebenmann3 revealed on microscopic examination that the lesion seemed to begin as spongification of the bone and termed the process otospongiosis.
Otosclerosis is an autosomal-dominant hereditary disease with variable penetrance and expression. Two thirds of patients are women. The hearing loss usually begins in the late teens or early 20s, but may not occur until the 30s or early 40s. At the House Ear Clinic, the youngest patient with surgically confirmed otosclerosis was 6 years old.4 It may be accelerated by pregnancy. Many female patients first report hearing loss during or shortly after their first pregnancy.
The prevalence of otosclerosis varies with race and its expression (Table 144-1). In whites, the disease is found in 7.3% and 10.3% of temporal bones for men and women. The stapes appears fixed in only 12.3% of patients with histopathologic evidence of otosclerosis. Clinical otosclerosis is rare in blacks, Asians, and Native Americans.5–11
Table 144-1 Occurrence of Clinical Otosclerosis
| Reference | Prevalence |
|---|---|
| Fowler and Fay, 1961, U.S.44 | 5% of patients with hearing loss* |
| Morrison and Bundey, 1970, England45 | 0.3% of East London’s population |
| Surján et al, 1973, Hungary (two sites)46 | 5.1% of patients with hearing loss; 2.4% of patients with hearing loss |
| Hall, 1974, Norway47 | 0.3% of Norway’s population |
| Pearson et al, 1974, U.S.48 | 239 : 100,000 in Rochester, MN, in 1970 |
| Moscicki et al, 1985, U.S.49 | 0.52% of a cohort study begun 29 years earlier |
| Huang and Lee, 1988, Taiwan50 | 1.13% of patients with hearing loss |
| Reference | Incidence |
|---|---|
| Hall, 1974, Norway47 | 56 : 100,000 for Norway’s population (1960-1969) |
| Pearson et al, 1974, U.S.48 | 13 : 700,000 in Rochester, MN, from 1950-1969; 8.9 : 100,000, from 1950-1959 |
| Stahle et al, 1978, Sweden51 | 12 : 100,000 yearly |
| Levin et al, 1988, Sweden8 | 6.1 : 100,000 for 1981 |
* Discounted patients with cerumen impaction.
From Cummings CW, Fredrickson JM, Harker LA, Krause CT, Schuller DE, eds. Otolaryngology–Head and Neck Surgery. 2nd ed. St. Louis: Mosby; 1993.
Histopathology
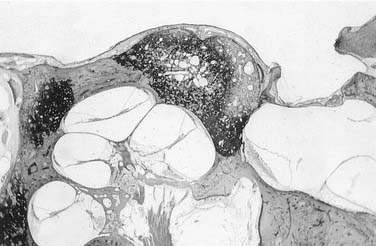
The extent and location of these lesions vary. Some are small and do not involve the stapes. Lesions that have ceased all activity appear sclerotic. As the disease advances, the lesions spread across the stapedial annular ligament, causing stapedial fixation. If the lesion progresses medially to involve the endosteum of the cochlea, sensorineural hearing loss results (Fig. 144-1). It may spread in both directions, resulting in a mixed sensorineural conductive hearing loss (Fig. 144-2).

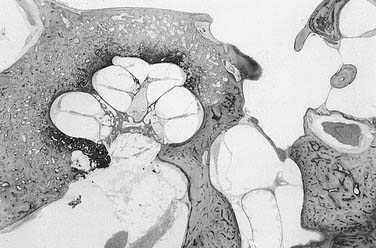
The type of stapedial fixation varies depending on the site of the lesion. If the lesion begins in the posterior oval window and spreads to the stapes through the anterior and posterior annular ligament, it causes bipolar stapes fixation. When the lesion flows across the ligament onto the footplate, it totally obliterates any remnant of the original annular ligament. If the center of the footplate remains uninvolved, it retains its characteristic cartilaginous vestibular and bony tympanic surface. The lesion may replace the entire footplate, causing a solid footplate (Fig. 144-3).
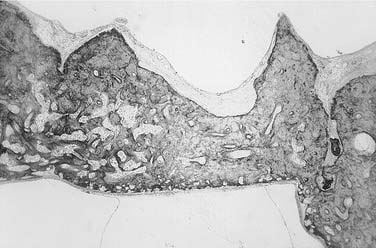
Figure 144-3. A solid stapedial footplate wherein the annular ligament has been totally replaced with otosclerosis.
Occasionally, the lesion may involve only the cochlea, causing an isolated sensorineural hearing loss (Fig. 144-4). Sometimes the entire cochlea is surrounded by otosclerosis, causing total deafness. In the United States, 20 of the first 57 patients to have a cochlear implant were made deaf by otosclerosis.12
Evaluation
Physical Examination
Physical examination includes careful otoscopy, often with the operating microscope. Pneumo-otoscopy is important to rule out middle ear serous fluid or a small perforation that could be the cause of a conductive hearing loss. There may be a red blush over the promontory or the area anterior to the oval window, known as the Schwartze sign. Tuning forks are essential for evaluation of any patient with a hearing loss13 because they may confirm or dispute the finding of a conductive hearing loss on audiometry.
Audiometry
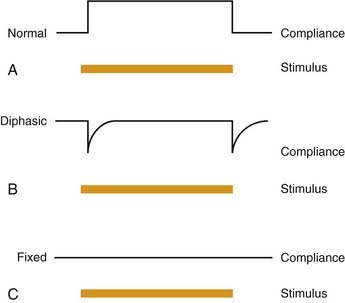
Acoustic reflexes are a sensitive measure of the movement of the stapes. In the presence of otosclerosis, the reflex is absent. With early stapes fixation, the reflex may be abnormal in that there is a negative on-off effect or diphasic reflex (Fig. 144-5). With more advanced disease, the reflex is absent when the probe is in the involved ear. As the disease and hearing loss worsen, the contralateral reflex is affected as a result of the degree of conductive hearing loss in the otosclerotic ear. Hannley14 wrote an excellent article about audiologic evaluation of a patient with otosclerosis.
Surgery
Small Fenestra Stapedotomy
The patient is placed supine on the operating table with the head turned away from the surgeon. The microscope is placed at the head of the table with the nurse standing across the table from the surgeon (Fig. 144-6). If general anesthesia is used, the anesthesiologist is seated at the foot of the table.

Incisions are performed with a sickle knife (No. 1) at the lateral process of the malleus and inferiorly at about the lower one fourth of the canal extended laterally approximately 8 mm. These two incisions are connected laterally with a House canal knife (No. 2). This flap is elevated evenly from lateral to medial with a canal elevator or a round knife (Fig. 144-7). It is important to elevate all of the flap at the same time so as not to tear it. When the anulus is reached, it is carefully exposed and elevated out of its bony canal with an anulus elevator “gimmick”. Care is taken during elevation to identify the chorda tympani nerve so that it is not stretched or injured. The superior elevation is carried forward to the malleus. Care is taken not to dislocate the incus. Usually the stapes is not entirely visualized because of the bony posterior superior external auditory canal overhang. This overhang is removed with a curet; alternatively, some surgeons prefer a microdrill (Fig. 144-8). The exposure is adequate when the facial nerve can be visualized superiorly, and the pyramidal process can be visualized posteriorly.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


