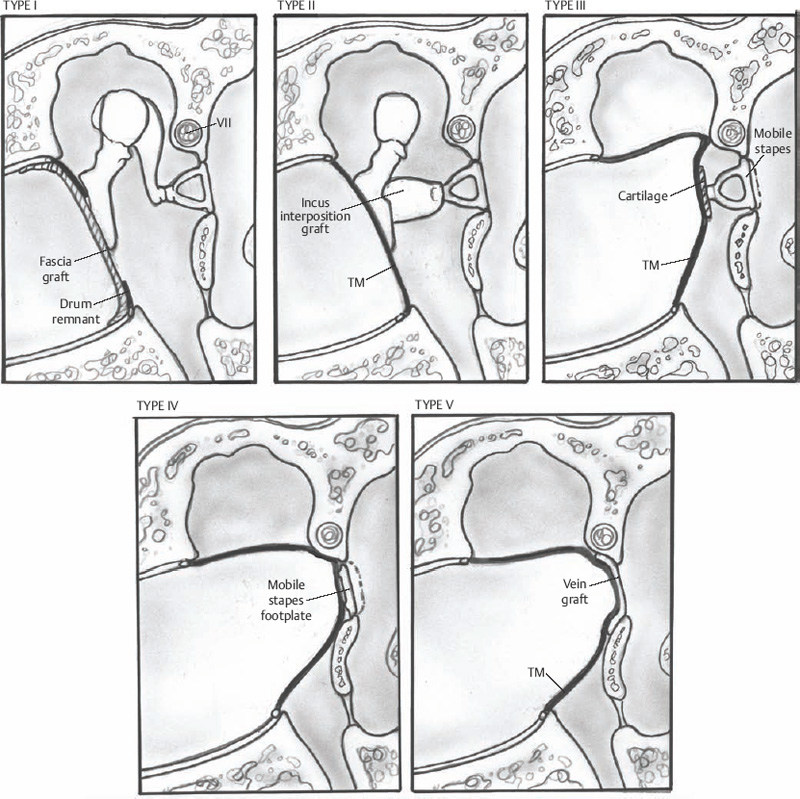
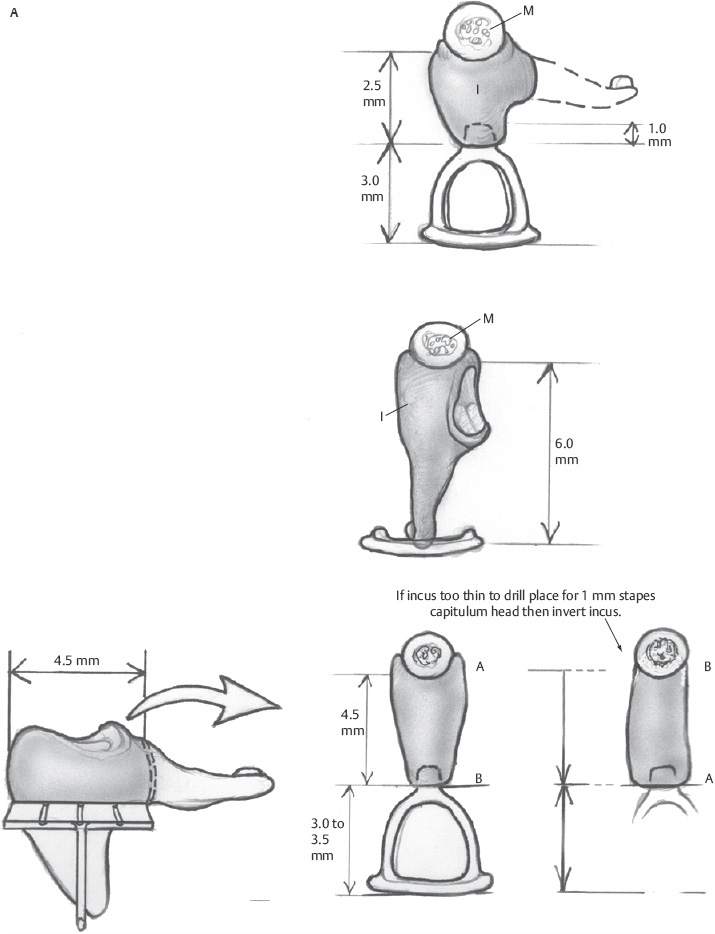
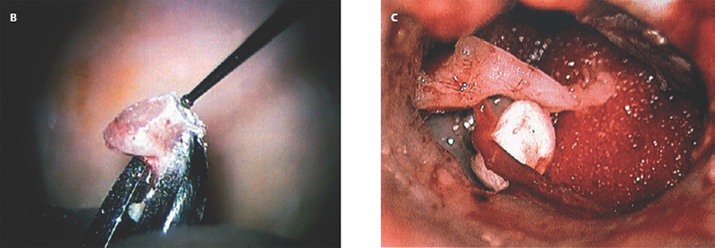
3 Ossicular Chain Reconstruction Success in ossicular chain reconstruction (OCR) is achieved when a mobile tympanic membrane and a secure sound-conducting mechanism to the inner ear fluids are present in the absence of infection or cholesteatoma. Early thoughts on hearing restoration following surgery for chronic ear disease date to some of the work of Wullstein and Zollner.1,2 This chapter reviews the mechanics of hearing, the history of OCR, the materials used for OCR, and factors predicting success in OCR. The normal human middle ear couples sound from the low-impedance sound energy in the ear canal through the tympanic membrane and ossicles to the relatively high impedance of fluid within the cochlea. In the absence of this mechanism, ∼97% of the sound waves reaching the oval window would be reflected or lost due to the impedance mismatch between the air and cochlear fluids. The difference between these media through which sound is conducted through the external auditory canal, the ossicles, and the fluids of the cochlea makes the middle ear an impedance-matching system minimizing the energy loss. This energy loss is made up in part by the acoustic transformation theory. There is the advantage of the tympanic membrane lever, the ossicular lever, and the hydraulic lever, and the gain is ∼27 to 34 dB.3 The tympanic membrane lever effect is from the tympanic membrane attachment to the malleus and provides a mechanical advantage creating amplification of energy of at least twofold gain in sound pressure at the malleus.4 The ossicular lever effect consists of malleus manubrium to incus lenticular process length and provides another 1.3 sound energy gain. The hydraulic lever effect is the 17-fold gain from the size mismatch between the tympanic membrane and the oval window footplate area (55 mm2 is the functional portion vs. 3.2 mm2 for the stapes footplate). Natural resonance and efficiency refer to the inherent anatomical and physiological properties of the external and middle ear, which allow certain frequencies to pass more easily to the inner ear.4 The natural resonance of the external auditory canal is 3000 Hz, whereas the middle ear is 800 Hz. The tympanic membrane is most efficient in transmitting sounds between 800 Hz and 1600 Hz, whereas the ossicular chain is most efficient in transmitting sounds between 500 and 2000 Hz. These properties produce the greatest sensitivity in sound transmission between 500 and 3000 Hz, approximately those frequencies that are most important in routine conversation. Three theoretical explanations for the frequency-dependent response of the ossicular chain are presented: ossicular coupling, acoustic coupling, and stapes-cochlear input impedance. Ossicular coupling refers to the sound pressure gain occurring through the actions of the tympanic membrane and ossicular chain. This is important when considering results in reconstruction of the ossicular chain and tympanic membrane (types I, II, and III tympanoplasties). The maximum middle ear gain is 25 dB at 1000 Hz. Acoustic coupling is due to the difference in sound pressures acting on the two inner ear windows. As sound energy is transmitted to the stapes footplate, fluid vibrations travel from the scala vestibuli up the cochlear partition to the helicotrema, then pass along the scala tympani toward the round window. The round window membrane is an elastic membrane that vibrates in response to sound waves traveling through the fluid medium of the inner ear. Because impulses created at the oval window must travel through the scala vestibuli and scala tympani before reaching the round window membrane, movements of the stapes footplate precede those of the round window membranes producing a phase difference between the two windows. Therefore, to transmit sound most efficiently, there must be oval window exposure and round window protection preventing sound waves from striking the round window simultaneously with the oval window and thus canceling out the vibrations. In some diseased and reconstructed ears (type IV, V tympanoplasties later described), loss of the tympanic membrane and ossicular chain can cause a hearing loss that exceeds 30 dB. This is explained by sound waves having access to both the round and oval windows causing cochlear fluid wave cancellation and interference. Shielding of the round window with cartilage or fascia results in redirection of all sound energy into the oval window.3 Acoustic coupling theory applied allows for closure of the air–bone gap to near 20 dB. Impedance at the oval window occurs because of the annular ligament, the viscosity of the cochlear fluids, and the round window membrane. The round window impedance contribution is negligible in the normal ear. When the round window niche is occluded with fluid or fibrous tissue, the round window impedance increases, resulting in a conductive hearing loss. Sound energy is also lost overcoming the stiffness and mass of the tympanic membrane and ossicular chain.5 One widely accepted classification scheme breaks tympanoplasty into five subtypes. Type I tympanoplasty (myringoplasty) involves reconstruction of a tympanic membrane defect with a completely intact ossicular chain. Type II tympanoplasty involves reconstruction of an eardrum in the absence of a usable malleus; hence the tympanic membrane is brought into contact with the incus and stapes assembly. Type III tympanoplasty grafts the eardrum directly to a mobile stapes superstructure, and type IV tympanoplasty involves grafting the tympanic membrane directly to a mobile stapes footplate and shielding the round window niche from external sound. Finally, the type V tympanoplasty involves removal of a fixed stapes footplate/superstructure and replacement with a fat or vein graft combined with obstruction of the round window niche (Fig. 3.1).3 Ossicular reconstruction has been evolving with technological advances over the past 60 years. Advances of prosthesis design include biocompatible material, ease of use at the time of surgery, lighter-weight design, and means of more firm attachment to the involved structures. Prostheses now have better connection to the capitulum of the stapes, ways to attach to the malleus, and footplate shoes to help limit slippage at the footplate area. Many materials have been used for OCR, but the ideal prosthesis should be biocompatible, capable of maintaining shape, rigid, and lightweight, with good acoustic properties. It should also be cost effective and easy to use in surgery tailored to the particular reconstructive needs of the patient. Extrusion rates for all prostheses are a factor of the material used and the recurrent diseased state of the ear. Cartilage covering all alloplastic material may help decrease the extrusion rate but is not absolutely necessary if the diseased retraction state of the middle ear has been successfully corrected with reconstruction of an aerated normalized middle ear state. Materials include polyethylene tubing, Teflon, Silastic tubing, stainless steel, titanium, gold, high-density polyethylene sponge (HDPS), bioglasses, and bioceramics.6 Utilization of the patient’s own incus or head of the malleus for reconstruction has always been the preferred method of reconstruction if the ossicle is present and not diseased. This is especially helpful in immediate reconstruction. The first of these materials as utilized in 1957 by Hall and Rytzner was the patient’s own malleus and incus.7 The ossicle is sculpted to the desired shape for the operative situation (stapes to malleus, footplate to malleus, stapes to tympanic membrane, or footplate to tympanic membrane) (Figs. 3.2 and 3.3A–C). Autologous incus grafts have been used for many years for middle ear reconstruction by modifying them to fit between the manubrium of the malleus and the stapes capitulum.8 Autograft incus has been shown to maintain contour, shape, size, and physical integrity for at least 11 years.3 In a series of 2200 cases, allograft and homograft prostheses yielded better hearing results than even the most biocompatible allograft prostheses.9 Cartilage is readily available and may be used for chain reconstruction. Autograft material, such as cartilage or bone, was one of the first materials used for ossiculoplasty.7 Over several decades of clinical investigation into the utility of autograft prosthesis, cartilage has been shown to be an inferior implant material because it loses rigidity and mass density through neovascularization and chondritis during long-term implantation in the middle ear.3,10 Schuknecht and Shi investigated the stability of osseous middle ear implants and found no evidence of bone erosion and little resorption.11 Even diseased ossicles that have retained body and bulk are safe to use for reconstruction after surface stripping under the operating microscope, though if the ossicle is malformed by disease at the time of surgery, they likely have microscopic residual and should not be used in reconstruction.12 To overcome some of the disadvantages of autografts, irradiated or preserved (in alcohol) homograft ossicles and cartilage were introduced in the 1960s. Homograft ossicles or cartilage are either presculpted by the processor or sculpted during surgery. Their use was common among early otologic surgeons, with hearing results and biocompatibility equivalent to autograft. The companies would preform the implant into structures of partial or total designs and in various lengths that could be used in the surgical environment. Many sizes and designs were kept in a preservative on the shelf for the surgeon to choose at the time of surgery. The environment surrounding homograft material has changed since 1986 with wider awareness of risk toward communicable diseases (human immunodeficiency virus, Creutzfeldt-Jakob disease).13 Today, at least in the United States, the use of homografts for ossicular reconstruction has drastically fallen. Fig. 3.1 I–V type of tympanoplasties. Fig. 3.2 Incus and malleus head before shaping. Initially there were prostheses designed of polyethylene, then Teflon, and finally porous polyethylene. Many of the early materials demonstrated high rates of migration, extrusion, and reactive fibrosis. Finally HDPS was developed, designed to closely mimic human bone density. HDPS is biocompatible in the middle ear, rigid, light weight, has good acoustic properties and is cost effective. If reconstruction was to go to the undersurface of the tympanic membrane, then a cartilage graft was necessary to prevent extrusion. These were made in two main designs. The partial prosthesis was to go from the capitulum of the stapes to the tympanic membrane with a cartilage cap, and the total prosthesis was to go from the stapes footplate to the undersurface of the tympanic membrane with a cartilage cap (Fig. 3.4). To assist in the angulation of the tympanic membrane some porous polyethylene prostheses have been engineered to have a wire in the lumen of the prosthesis to hold the angulation of the top of the prosthesis. Extrusion rates have averaged 3 to 5% in experienced hands in a series with a 5- to 10-year follow-up.14–16 Fig. 3.3 (A) Incus shaping of different lengths as needed for surgery. (B) Drilling incus with a 1 mm cutting drill and incus held in a malleus cutting forceps. (C)
♦ Acoustic Mechanics
♦ History of Prostheses Development in Ossicular Chain Reconstruction
Autografts
Homografts

Alloplasts
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


