Fig. 17.1
Primary orbital retinoblastoma. Orbital extension of an intraocular retinoblastoma at the initial clinical presentation, manifesting as massive proptosis (a). Computed tomography scan confirmed an orbital mass (b)
17.3.2 Secondary Orbital Retinoblastoma
Orbital recurrence following uncomplicated enucleation for intraocular retinoblastoma is termed secondary orbital retinoblastoma (Fig. 17.2). This may present as an orbital mass several weeks to years after the primary surgery. Unexplained displacement, bulge, or extrusion of a previously well-fitting conformer or a prosthesis, a displacement of the implant, or a palpable orbital mass would be suggestive of an orbital recurrence. A vascular conjunctival nodule may also be a feature of orbital retinoblastoma.
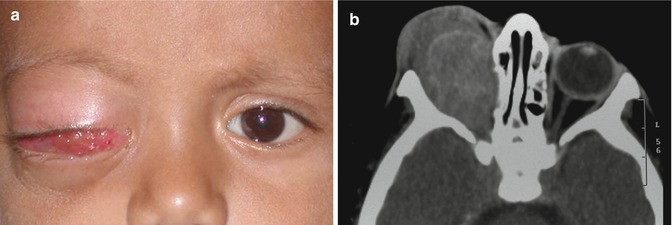
Fig. 17.2
Secondary orbital retinoblastoma. Orbital recurrence of retinoblastoma 6 months following enucleation for intraocular retinoblastoma in the right eye (a). Computed tomography scan showing an orbital mass (b)
17.3.3 Accidental Orbital Retinoblastoma
Inadvertent perforation during enucleation, fine needle aspiration biopsy, or intraocular surgery in an eye with unsuspected intraocular retinoblastoma should be considered as accidental orbital retinoblastoma and managed as such (Fig. 17.3).
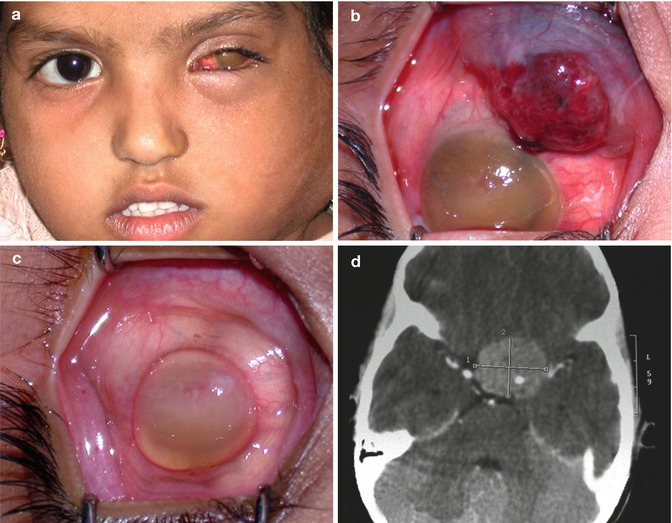
Fig. 17.3
Accidental orbital retinoblastoma. Cervical lymphadenopathy 6 months following hyphema drainage in an eye with unsuspected retinoblastoma (a). Note vascular conjunctival mass (b). Although the conjunctival mass resolved with high-dose chemotherapy (c), the child succumbed to intracranial metastasis (d)
17.3.4 Overt Orbital Retinoblastoma
Previously unrecognized extrascleral or optic nerve extension discovered during enucleation qualifies as overt orbital retinoblastoma (Fig. 17.4). A pale pink to cherry red episcleral nodule, generally in a juxtapapillary location or at the site of vortex veins, may be visualized during enucleation. An enlarged and inelastic optic nerve with or without nodular and adherent optic nerve sheath are clinical indicators of optic nerve extension of retinoblastoma that can be recognized on careful inspection of the eye following enucleation.
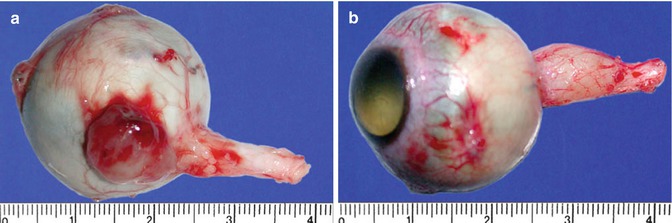
Fig. 17.4
Overt orbital retinoblastoma. Previously unrecognized extrascleral mass (a) and optic nerve extension (b) discovered during enucleation
17.3.5 Microscopic Orbital Retinoblastoma
In several instances, orbital extension of retinoblastoma may not be clinically evident and may only be microscopic. Detection of full-thickness scleral infiltration, extrascleral extension, and invasion of the optic nerve on histopathologic evaluation of an eye enucleated for intraocular retinoblastoma are unequivocal features of orbital retinoblastoma (Fig. 17.5). Tumor cells in choroidal and scleral emissaria and optic nerve sheath indicate possible orbital extension mandating further serial sections and detailed histopathologic analysis.
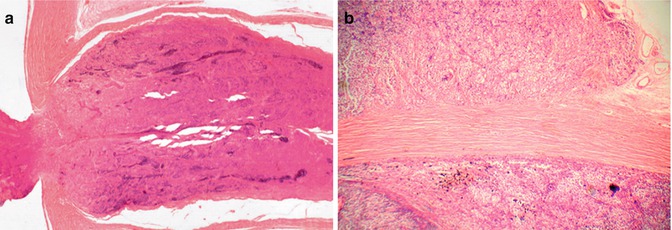
Fig. 17.5
Microscopic orbital retinoblastoma. Histopathologic evaluation of an eye enucleated for intraocular retinoblastoma. Invasion of the optic nerve to the level of transection (a) and extrascleral extension (b)
17.4 Diagnostic Evaluation
A thorough clinical evaluation paying attention to the subtle signs of orbital retinoblastoma is necessary. Magnetic resonance imaging preferably or computed tomography scan of the orbit and brain in axial and coronal orientation with 2-mm slice thickness helps confirm the presence of orbital retinoblastoma and determine its extent. Systemic evaluation, including a detailed physical examination, palpation of the regional lymph nodes, and fine needle aspiration biopsy of the enlarged lymph nodes, imaging of the orbit and brain, chest x-ray, ultrasonography of the abdomen, bone marrow biopsy, and cerebrospinal fluid cytology are necessary to stage the disease. Technetium-99 bone scan and positron-emission tomography coupled with computed tomography (PET-CT) may be useful modalities for early detection of subclinical systemic metastases [16, 17]. Orbital biopsy is rarely required and should be considered specifically when a child presents with an orbital mass following enucleation or evisceration where the primary histopathology is unavailable.
17.5 Management
17.5.1 Primary Orbital Retinoblastoma
Primary orbital retinoblastoma has been managed in the past with orbital exenteration, chemotherapy, or external beam radiotherapy exclusively or in sequential combination, with variable results [18–23]. It is well known that local treatments have a limited effect on the course of orbital retinoblastoma. Orbital exenteration alone is unlikely to achieve complete surgical clearance and preclude secondary relapses and systemic metastasis; external beam radiotherapy will not affect systemic micrometastasis; and chemotherapy alone may not eradicate residual orbital disease [21, 22]. Therefore, multimodal therapy with a judicious, customized, and sequential combination of neoadjuvant and adjuvant chemotherapy, surgery, and EBRT is considered to be more effective. In a case series of five children, Goble and associates demonstrated long-term survival with local surgical excision, orbital radiotherapy, and systemic chemotherapy [21].
We have developed a treatment protocol (Table 17.1) consisting of triple-drug (vincristine, etoposide, and carboplatin) high-dose neoadjuvant chemotherapy (3–6 cycles) followed by surgery (enucleation, extended enucleation, or orbital exenteration as appropriate after determining the extent of residual orbital tumor by CT scan), orbital radiotherapy, and adjuvant chemotherapy (Table 17.2) [24, 25]. In all, 12 cycles of chemotherapy are administered.
Table 17.1
Suggested protocol for management of primary orbital retinoblastoma
Baseline investigations | |||
Computed tomography scan or magnetic resonance imaging | |||
Bone marrow biopsy | |||
Cerebrospinal fluid cytology | |||
Treatment | |||
Initial chemotherapy | High-dose three-drug chemotherapy for 3–6 cycles (every 3 weeks) | ||
Surgery | Enucleation | Assessment of orbital tumor by imaging after completion of third cycle | |
After completion of third cycle if the orbital tumor is resolved | |||
Additional 3 cycles of chemotherapy | |||
After completion of sixth cycle if the orbital tumor is resolved | |||
Exenteration | After completion of sixth cycle if the orbital tumor is present | ||
External beam radiation | 45–50 Gy (fractionated) to the orbit | ||
Subsequent chemotherapy | Continuation high-dose chemotherapy for 12 cycles | ||
Follow-up investigations | |||
Imaging at 12, 18, 24, and 36 months | |||
Bone marrow biopsy and cerebrospinal fluid cytology at 6, 12, 18, 24, and 36 months | |||
Table 17.2
Chemotherapy drugs, dose (milligram per kilogram body weight), and schedule for treatment of orbital retinoblastoma
Drugs | Standard dose | High dose | ||
|---|---|---|---|---|
Day 1 | Day 2 | Day 1 | Day 2 | |
Vincristine | 0.05 | 0.025 | ||
Etoposide | 5.0 | 5.0 | 12.0 | 12.0 |
Carboplatin | 18.6 | 28.0 | ||
17.5.2 Secondary Orbital Retinoblastoma
Our treatment protocol outlined for primary orbital retinoblastoma currently under evaluation for secondary orbital retinoblastoma and early results have been very encouraging. Surgical intervention in such cases may be limited to excision of the residual orbital mass or an orbital exenteration depending on the extent of the residual tumor after the initial 3–6 cycles of high-dose neoadjuvant chemotherapy. Surgery is not necessary if the orbital tumor completely resolves following neoadjuvant chemotherapy. Treatment is completed with orbital EBRT and chemotherapy for a total of 12 cycles.
17.5.3 Accidental Orbital Retinoblastoma
The surgeon should be careful not to accidentally perforate the eye during enucleation for retinoblastoma. Many surgeons prefer to avoid traction sutures applied at the insertion of extraocular muscles to minimize the risk of accidental perforation. Instead, hemostat applied to medial or lateral rectus muscle stump or cryoprobe applied at the limbus provides adequate traction. Eyes manifesting tumor necrosis with aseptic orbital cellulitis pose specific risk for accidental perforation. Surgery in such eyes is best performed when the inflammation is resolved. A brief course of preoperative oral and topical steroids helps control inflammation. If inadvertent perforation does occur during enucleation, further steps of surgery should be performed carefully, with minimal manipulation, under good illumination and magnification, and preferably by a senior surgeon. If the perforation is small, orbital contamination can be limited by sealing the perforation site with a patch of Tenons glued into position with cyanoacrylate glue. Larger perforations can be handled by isolating the area with dry absorbent cotton, suturing the perforation if possible and sealing the suture site with a glued-on Tenon’s patch. Extensive perforations can be managed by isolating the area with dry absorbent cotton and suction evacuation of tumor tissue prolapsing through the wound using a powered suction, followed by wound suturing and glued-on Tenon’s patch. In all these situations, enucleation is completed as planned with minimal manipulation. Integrated orbital implants are best avoided, and a polymethyl methacrylate or silicone implant is preferred in such cases, since there would be an impending need for adjuvant radiotherapy.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


