Chapter 105 Optimal Procedures for Retinal Detachment Repair
 For additional online content visit http://www.expertconsult.com
For additional online content visit http://www.expertconsult.com
Introduction
About a century ago, rhegmatogenous retinal detachment (RRD) was essentially untreatable. A survey of ophthalmologists, carried out in 1912, estimated the success rate of therapy to be 1 in 1000.1 Many treatments were attempted, ranging from draining subretinal fluid to injections of mercury salts around the eye, but without success. Jules Gonin was the first to realize that curing RRD required prevention of recruitment of subretinal fluid through retinal breaks. His introduction of thermocautery immediately raised the success rate to about 1 in 2, a landmark achievement.2 The etiology of RRD is now better understood, and most surgeons agree that retinal breaks should be first closed, and then permanently sealed with retinopexy. However, despite this agreement, there is still enormous variation between surgeons in their choice of procedure for particular detachments.3 This chapter aims to examine those procedures, and assist the reader in choosing between them, for eyes with noncomplex RRD.
Round hole retinal detachment
Introduction
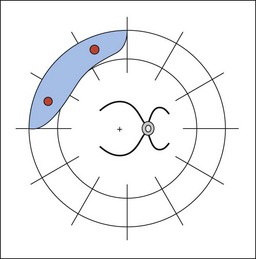
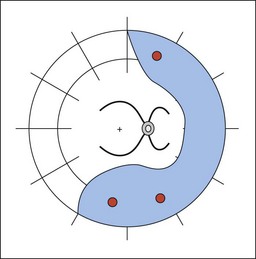
In eyes with round hole retinal detachment, the causative breaks are small round holes, often associated with lattice degeneration. Patients affected are typically young, low myopes, presenting with blurring of vision and a visual field defect. Some patients are asymptomatic and picked up on routine examination (Figs 105.1, 105.2). Round hole detachments are relatively uncommon, and in a large series of RRD reported by Tillery and Lucier, only 2.8% of cases were found to be secondary to round holes.4 Other series have reported a higher frequency, with 13.9% being reported by Morse and Scheie,5 and 21% in a series from Japan.6 An important clinical finding in these patients, is that the posterior hyaloid is usually attached. For example, in a large series of 110 round hole detachments requiring treatment, only eight (7%) of the eyes had a detached vitreous, and in these cases, the associated clinical findings suggested that the retinal detachment predated the posterior vitreous detachment (PVD).7
Natural history
Much of our understanding of the natural history of round hole detachments comes from the painstaking work of Norman Byer. In a long-term follow-up of patients with asymptomatic retinal lesions, there were 17 eyes with 18 areas of round hole retinal detachment.8 The majority (75%) of the patients were followed-up for more than 5 years, and some for up to 12 years. There was no change in 13 of the 18 areas of detachment, and only a minor change in three areas (18%). In a later report, Byer reported on 19 eyes with up to 33 years of follow-up.9 There were 22 areas of subclinical detachment in the 19 eyes, seven of which showed some form of progression, and only two of which required treatment, which was successful in both. Therefore, it can be stated that none of the patients in this series lost vision as a result of the initial decision to defer surgery.
A common misconception is that a pigment line, or “tide mark” or “demarcation line” posterior to the area of detachment will prevent progression. This is not the case, though such a line does imply stability of the extent of the detachment for at least some months. Benson studied 66 retinal detachments with demarcation lines (a subset of a larger series all requiring surgery), 20 of which were detected on routine examination. Most of these patients were young (median age 33), and had detachments secondary to round holes. The demarcation line had failed to prevent progression in 51 of the 66 cases.10
Brod et al. observed 28 patients (31 eyes) for 0.5–12.1 years (a mean follow-up of 3.4 years). The patients’ age range was 17–82 years, with a mean of 49 years. The majority of eyes were myopic, with 76% of patients having refractive errors of −2 diopters or more. A demarcation line was present in 23 eyes (74%). Only one patient progressed to develop symptoms with associated detachment of the macula, and reduction of visual acuity to 20/30, 3.3 years later. Vision returned to 20/20 following successful surgery. Another patient developed a new detachment from a subsequent PVD and a retinal “U” (“horseshoe”) tear.11
Jarrett reported on 16 patients with retinal detachments in whom surgery was delayed or did not occur. Eleven of these patients had round holes or dialyses. Eight patients had buckling surgery up to 8 years after detection, the delay being for a variety of reasons, including reluctance on behalf of asymptomatic patients to undergo eye surgery. Seven eyes progressed, but only one patient who delayed surgery presented later with a detached macula.12
Treatment
Laser demarcation
The extent of detached retina can be limited by creating a surrounding adhesion between the retina and the retinal pigment epithelium (RPE). This is the principle of retinopexy, and is widely used to treat retinal tears. The principle can also be applied to wider areas of detachment with a view to limiting progression.13 Such treatment of course does nothing to resolve an existing detachment, so this choice of management effectively “writes off” the detached area of retina. This is appropriate in patients with asymptomatic retinal detachments, or those with very minimal symptoms.
The aim of demarcation treatment is to create a band of effective chorioretinal adhesion, which completely surrounds the area of detachment. This generally means applying treatment from ora to ora, just posterior to the fluid (Fig. 105.3). Although cryotherapy could be used, laser photocoagulation is preferred as it causes less tissue damage, and less inflammatory reaction to the external eye. There is evidence that an adhesion stronger than normal appears within 24 hours of the application of treatment,14 but maximum strength is achieved between 3 and 14 days later.15 Therefore, laser demarcation is not suitable for rapidly progressive detachments.
There is only a limited amount of experience in the literature to assess the long-term value of this treatment. Okun et al. discussed demarcation in 1968. The authors treated 48 eyes, and 42 (88%) were stable after 0.5–6 years follow-up. Of the remaining six eyes, three developed additional areas of detachment from new breaks, and three were judged at the time of laser to need surgical treatment.16 Treplin presented a series of four cases from Tasmania, explaining; “Any Tasmanian presentation is in single figures, as there are not very many Tasmanians.” In one case with an extensive area of detachment, laser failed to prevent progression.17
Gratton treated 42 phakic patients with limited retinal detachments and attached maculae. Most patients (54%) were myopes. Follow-up was for 1–4 years, during which time only one case progressed. In this patient, surgery was successful in reattaching the retina with no visual loss or complications.18
Vrabec and Baumal treated 34 eyes with a variety of retinal detachments, all with attached maculae. They used the indirect laser ophthalmoscope to produce three confluent rows of retinopexy extending posteriorly to the fluid from ora to ora. All eyes were stabilized except one, in which inadequate laser had been applied because of the proximity of the posterior pole.19
Scleral buckling
The primary success rate of scleral buckling in round hole detachments is very high, but there is a risk of ocular morbidity. Tillery and Lucier reported results of buckling surgery in cases with detachments secondary to round holes in lattice (some of whom were asymptomatic). The reattachment rate with scleral buckling was 98%. However, 15% had worse vision postoperatively, and the proportion of eyes with worse post-operative vision in the subgroup of those eyes with 20/40 or better preoperatively, was 31%.20 Greven et al. reported results of 28 eyes of 27 patients with subclinical detachments. In 16 eyes (57%), the detachment was detected on a routine examination, and in eight patients, the fellow eye had a previous symptomatic detachment. All eyes were treated with segmental scleral buckling, and two were encircled. The initial reattachment rate was 100%, but one eye developed another retinal detachment associated with new breaks after 14 months. One eye lost vision from 20/20 to 20/30 “without obvious cause,” but no mention was made of any other complications.21
Ung et al. from Cambridge reported excellent results from scleral buckling in a large series of retinal detachments secondary to round holes. All but one of 110 detachments were repaired with a single procedure, a success rate of 99%.7
Detachment due to retinal dialyses
Introduction
A retinal dialysis is a tear of the retina from its insertion at the ora serrata.22 Some dialyses are secondary to trauma, and are most commonly found in the inferotemporal quadrant.23 Non-traumatic idiopathic dialyses also occur, and tend to be bilateral and inferotemporal,22,24 and some such cases may be inherited.25 In a large series of 1601 retinal detachments, 71 (4.4%) were found to be secondary to a retinal dialysis.26 The majority of patients were young (mean age 30), and there was a male to female preponderance of 1.3 : 1. Only 70% of patients gave a history of trauma. The vitreous is attached in the vast majority of cases. In Bonnet’s series, a PVD was only found in 1 of 48 cases (2.1%).27
Natural history
There is often a long interval between the creation of the dialysis, and the development of a symptomatic retinal detachment. In the series of traumatic retinal detachments described by Cox et al., the time from trauma to retinal detachment was up to 40 years, though in 80% of cases, was less than 2 years.28 In another series of 50 patients, 41% of the detachments due to traumatic dialysis were diagnosed more than 1 year after injury.29 The progression of the detachment can be slow, and this may be related to the lack of vitreous detachment. If the detachment is not detected until the macula becomes involved, then the final visual acuity can be compromised. In Ross’s series, 84% of eyes had detached maculae prior to surgery.29 In a report on patients with traumatic retinal detachments from Northern Ireland, patients with delayed diagnosis were found to have a less favorable visual outcome than those who were diagnosed within 6 weeks of the trauma.30
Conservative management
The considerations and options for management of patients with limited detachment secondary to dialysis are identical to those for patients with round hole detachments. Cases with signs of chronicity, such as tidemarks and retinal cysts, have probably been stable for some time, consequently with a relatively low risk of progression. In one series of 71 detachments secondary to dialysis, three patients had such signs of chronicity and were therefore followed-up without incident.26
Treatment
Laser demarcation
Limited detachments secondary to dialysis respond well to laser demarcation. This is particularly true for the majority of detachments from dialyses which are in the inferotemporal quadrant. Walling off of the affected area here results in a permanent field defect superonasally, which is likely to be less important to the patient, than inferotemporal field loss. In Kennedy’s series of 71 patients, five were successfully treated with retinopexy in order to demarcate a local detachment.26
Scleral buckling
Dialyses respond well to segmental scleral buckling procedures. In a series of traumatic retinal detachments including 49 cases of dialysis, the primary success rate was 96%.30 In another series from France of 48 cases of retinal detachment secondary to dialysis, the primary success rate was 100%.27 Ross described a series of 50 eyes with a primary success rate of 94% and a final success rate of 98%.29 The primary success rate for surgery in Kennedy’s series was 97%.26
Retinal detachment secondary to “u” (“horseshoe”) tears
Introduction
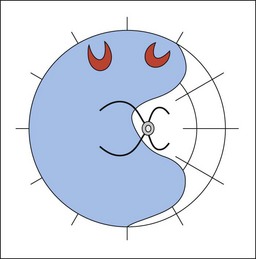
This category represents the most common group of rhegmatogenous retinal detachments. The detachment is secondary to one or more traction “U” tears, which in turn follow PVD (Fig. 105.4). A typical patient will present with visual loss, a symptomatic field defect, and a history of floaters and flashing lights some weeks previously.
Natural history
We know from studies prior to Gonin that the prognosis for vision in untreated cases is very poor. A relatively recent study of long-term findings in untreated retinal detachment showed severe loss of vision in all patients, with the best level of vision being hand movements. In addition there was a significant rate of discomfort and cosmetic problems.31 Following formation of tears, detachment tends to occur rapidly, due to a combination of recruitment of subretinal fluid through the break, and continuing vitreous traction on the flap. In the majority of cases, tears occur at the time of the PVD, or shortly afterwards. However, there is evidence that in pseudophakic eyes, chronic traction from a pre-existing PVD can lead to new, anterior breaks.32,33 Fluid currents within the eye also play a significant role in the development of the detachment, as described by Machemer in his Jackson Memorial Lecture in 1988.34 Subretinal fluid from superior tears spreads more rapidly than that from inferior ones, and this needs to be borne in mind when planning the timing of intervention in eyes with an attached macula. The rapid progression of most detachments in this category means that a majority of patients present with their macula already detached. In Burton’s series of 953 primary retinal detachments, 69.5% of cases had detached maculae preoperatively.35
Conservative management
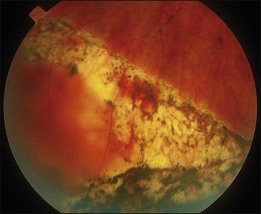
Occasionally, a small, asymptomatic peripheral detachment from a “U” tear might appear stable, with subsequent development of a tide mark, in which case, careful observation might be appropriate (Fig. 105.5). Since these detachments tend to occur in an older age group, there are also cases in whom severe medical comorbidity precludes any form of treatment.

Treatment
Laser demarcation
Although laser photocoagulation creates an instant adhesion, this is not up to full strength for up to 14 days.15 Rapidly progressing fluid may extend through the area of demarcation before a strong enough adhesion develops. This form of treatment should therefore be used with caution in patients with RRD secondary to “U” tears.
Pneumatic retinopexy
The use of intraocular gas in the treatment of retinal detachment was first described by Ohm in 1911,36 and good results in a large series were reported by Rosengren.37 Modern pneumatic retinopexy was introduced by Hilton and Grizzard in 1986.38 Expanding gas is injected into the vitreous cavity, followed by application of cryotherapy or laser photocoagulation. The technique can be applied in an outpatient setting under local anesthesia. Postoperatively the patient positions their head so that the gas bubble is opposed to the break or breaks. This limits the flow of fluid into the subretinal space, and allows reabsorption of the existing fluid by the retinal pigment epithelium. The technique is most appropriate for detachments with breaks limited to one quadrant, usually superiorly. Complications of pneumatic retinopexy include raised intraocular pressure, and subretinal gas.39 The expanding gas may exert traction inferiorly leading to the creation of new, inferior breaks, particularly in the presence of inferior lattice degeneration.40 New or missed breaks are a common cause of failure following pneumatic retinopexy, accounting for half the failures in one series.41
Pneumatic retinopexy was found to have a comparable success rate to vitrectomy with cryotherapy and gas in a prospective randomized control trial in 120 cases.42 A large multicenter randomized trial compared pneumatic retinopexy with scleral buckling in 198 patients. There was a higher rate of primary reattachment in the scleral buckling group (82% versus 73%), but this difference did not achieve statistical significance (P>0.05). There was no difference in the final reattachment rate (98% versus 99%). However, the patients with pneumatic retinopexy had less morbidity and better final visual acuity.43
A recent meta-analysis comparing pneumatic retinopexy to primary scleral buckling, reported that scleral buckling had a higher primary success rate.44 However, most studies have indicated no difference in the final success rate between the two, and more importantly, no difference in the final visual acuity. A large retrospective series of 302 eyes treated with pneumatic retinopexy showed an average primary success rate of 68%, with a final reattachment rate of 95%.45 Given that pneumatic retinopexy is a relatively quick and simple procedure, with less morbidity than scleral buckling, it is worth considering as an initial procedure. This is particularly the case for patients who have “classic” indications, as the success rate appears higher in this group. In a subgroup of patients with phakic eyes, single breaks, and fluid confined to one superior quadrant, the primary success rate was 97%.45
There is evidence that pneumatic retinopexy is less effective in aphakic and pseudophakic eyes. In a series of 56 eyes, the primary success rate was 81% in a subgroup of phakic eyes but only 43% in eyes which were aphakic or pseudophakic.46 In summary, a high primary success rate with pneumatic retinopexy can be achieved in phakic eyes with “classic” indications. Even if treatment fails, a good final result can be expected following further surgery.
Most surgeons who use pneumatic retinopexy, apply it as a primary procedure, and then employ scleral buckling if it fails. However, pneumatic retinopexy can also be used as an effective method of treating detachments after failed scleral buckling. In most of these cases there is persistent elevation of the retinal break above the buckle, and retinopexy has already been applied. All that is necessary is temporary reduction in fluid flow through the break to allow the retina to settle. In a series of 36 eyes with failed scleral buckling surgery, injection of gas was successful in reattaching the retina in 25 (69.4%).47
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


