Chapter 134 Remote Effects of Cancer on the Retina
Introduction
Neurologic manifestations from metastatic carcinoma have been recognized for over 100 years. However, paraneoplastic neurologic disorders have been recognized only for the past 50 years, with the initial descriptions of subacute cortical cerebellar degeneration associated with visceral carcinomas. Neurologic paraneoplastic syndromes have been estimated to occur in up to 15% of cancer patients, half of whom have primary carcinoma of the lung.1,2
The prevalence of ophthalmic paraneoplastic syndromes is unknown. Although uncommon, the remote effects of cancer on the eye are important to recognize because they may be the presenting signs of previously undiagnosed malignancy or may suggest recurrence of previously treated disease.3–5 Furthermore, the recognition of these syndromes in patients with unexplained visual loss may aid the ophthalmologist in palliative management, since the disabling ocular symptoms may be amenable to medical therapy.4,6
Paraneoplastic neuro-ophthalmic syndromes are part of a spectrum of autoimmune disorders that also encompass autoimmune retinopathy (Chapter 77, Autoimmune retinopathies) and autoimmune optic neuropathy.6,7
Cancer-associated retinopathy syndrome
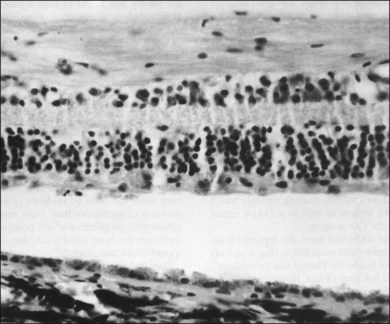
In 1976, Sawyer and coworkers3 described three patients with sudden onset of vision loss, positive visual phenomena, ring-like scotomata, and nyctalopia who developed light perception vision and were later diagnosed as having bronchogenic carcinoma. Fundus examination demonstrated only nonspecific pigment mottling in the posterior pole, normal optic nerves, and a slight degree of vascular attenuation with variable sheathing. Histopathologic examination in each case demonstrated widespread severe degeneration of the outer nuclear retinal layer and disintegration of photoreceptors, as well as the presence of macrophages containing phagocytosed granules from the retinal pigment epithelium (RPE) (Fig. 134.1). As opposed to eyes with retinitis pigmentosa, the RPE and choriocapillaris were remarkably preserved in all eyes examined. The authors believed that these features excluded a vascular basis for the observed findings and concluded that these represented a remote effect of bronchogenic carcinoma.3
Subsequently, Keltner and colleagues4 described a patient with undifferentiated cervical cancer presenting with progressive blindness, progressive retinal arteriolar narrowing, a few vitreous cells, and a flat electroretinogram (ERG). Antibodies were found in the patient’s serum against normal photoreceptors from fresh normal human retinal tissue. A trial of steroids was initiated, which improved vision. Histopathologic examination later disclosed a loss of retinal photoreceptors and the outer nuclear layer. The authors proposed a possible autoimmune mechanism for these findings.
Klingele and co-workers8 described a similar picture in a patient with mottled hyperfluorescence on fluorescein angiography, who was later diagnosed with breast carcinoma, and they termed this “paraneoplastic retinopathy.”
The term “cancer-associated retinopathy” (CAR) syndrome has subsequently come to be used to describe the clinical picture of subacute visual loss resulting from circulating antibodies against retinal proteins in the presence of systemic cancerous tumor growth and over 50 cases have been published to date.2,5,9,10
There is no gender predisposition in CAR syndrome, and the symptoms of decreased vision, a halo of missing peripheral vision, positive visual phenomena (“sparkles”), photosensitivity, impaired color vision and night blindness usually antedate the clinical signs and symptoms of systemic malignancy by a mean of 5 months in up to 50% of cases.11 The longest duration from the onset of CAR syndrome to diagnosis of the carcinoma was 11 years in a patient with a pulmonary carcinoma.12 Patients with CAR syndrome generally progress from initial stages of visual loss to blindness in 6–18 months.4,5,10
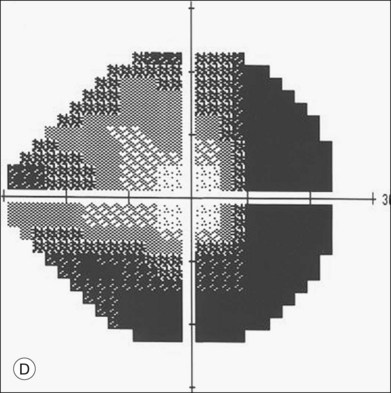
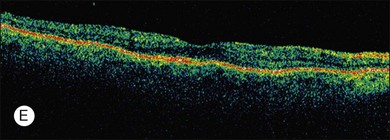
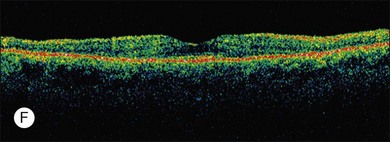
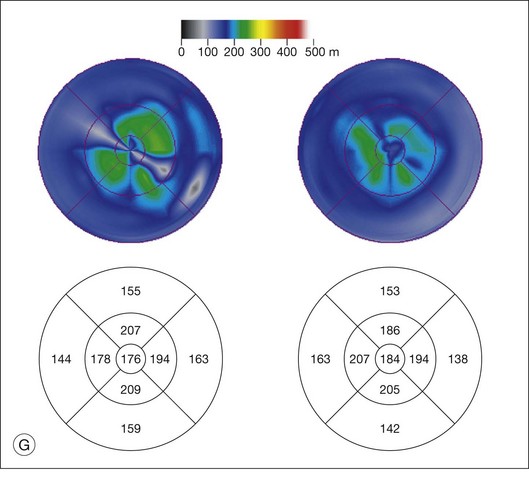
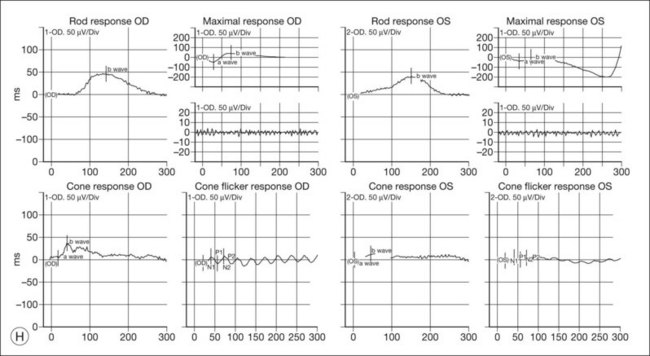
ERG findings in patients with CAR syndrome have been reported to show extinguished a and b waves or rod responses larger than cone responses (Fig. 134.2). Occult malignancy should be suspected in patients with acquired night blindness, minimal ocular findings to account for the visual difficulty, and abnormal ERG results.13 The presenting symptoms may be asymmetric, and some patients complain of glare and photosensitivity.14–17 Cells in the vitreous or anterior chamber are infrequently reported in CAR syndrome.4,8 Tonic pupils have been reported to be a potential ophthalmic finding in paraneoplastic syndromes.18 Reduced macular thickness on OCT examination may be observed prior to severe visual loss, and may be useful in demonstrating retinal damage in these patients.19



The most common malignancies related to CAR are carcinomas, and over half of all these patients have a pulmonary malignancy with the most common being small cell carcinoma of the lung.1,3,5,10,14–17,20–31 A chest X-ray should usually be obtained as part of the evaluation of suspect individuals. Other malignancies associated with CAR include those of the colon,32 endometrium/uterus,33–37 cervix,4,27,38 breast,8,39,40 prostate/bladder,39–41 thorax (rhabdomyosarcoma),42 abdominal liposarcoma,44 and systemic lymphoma.43 In rare instances, patients with documented antibodies to the retina and classic symptoms of CAR may not have an associated underlying malignancy. These patients constitute a minority of patients referred to as autoimmune retinopathy not associated with underlying malignancy and are discussed in greater detail in Chapter 77, Autoimmune retinopathies (Fig. 134.3).2,15,41,45–47
Based on an ultrastructural study showing immature melanin granules within melanolysosomes, Buchanan and co-workers48 suggested that a hormone-like substance produced by the tumor increased melanin synthesis in the pigment epithelium and that the increased melanin content in these cells compromised their ability to phagocytose and maintain normal turnover of photoreceptor outer segments. Since that report, a growing body of evidence has supported an autoimmune basis for CAR syndrome.49–51 In 1982, Kornguth et al.23 reported on the presence of 23 kDa (kilo Dalton) serum antiretinal ganglion cell antibodies in patients with visual dysfunction and small cell carcinoma of the lung. Subsequently, Grunwald et al.14 described the reaction of such antibodies with specific retinal antigens in the ganglion cells and inner nuclear layers and immunologically related antigens in tumor cells (as well as their absence in patients with tumors but with no visual defects). They proposed that the small cell tumor produces antigens normally associated with retinal tissue. These antigens are recognized as foreign, since the retina is an immunologically privileged site without antiself suppressor mechanisms.14,51 CAR syndrome can also be associated with uveitis (vitritis and vascular sheathing)4,35,52,53; as the concentrations of autoantibodies reach a critical threshold, they cross the abnormally permeable blood–retina barrier. It is postulated that a cross-reaction with retinal tissue occurs, and subsequently a nonspecific immune-mediated common pathway of retinal degeneration with apoptosis ensues.
The 23 kDa antigen to which antibodies have been produced in the majority of individuals with CAR syndrome has been shown to be recoverin, a calcium channel photoreceptor protein.17,21,27,29,46,54–57 No clear role for recoverin in the normal functioning of photoreceptor cells has been demonstrated, but binding to this protein results in cellular death by some unknown mechanism. Antibodies to the CAR antigen (recoverin) were not previously demonstrated in any other form of retinopathy, nor were these antibodies believed to be expressed by tumors without associated retinopathy.5,17 Recently, however, a clinically distinctive condition has been described resembling CAR with a cellular immune response against recoverin (recoverin-associated retinopathy).58
Now available commercially, the Western blot analysis for the CAR antigen-antibody may be negative even in the presence of CAR syndrome.52 Moreover, the titers of antibody versus recoverin do not necessarily correlate with the severity of the clinical retinopathy. Hence, clinical criteria and a high index of suspicion remain the mainstay of diagnosis.
Thirkill and co-workers10 reported on isolation of antibodies reacting strongly with the 23 kDa retinal protein in addition to yet another 65 kDa lung cancer antigen. Other antiretinal antibodies have been found in patients with retinopathy (abnormal ERGs, ring scotomata or depressed visual fields), but these patients did not have demonstrable cancer. However, these patients differ from patients with CAR syndrome on the basis of lower antiretinal antibody titers, as well as on the basis of their reaction to a different 40 kDa retinal protein.17,59
Adamus and colleagues56 reported several cases of CAR syndrome in association with antibodies to a 46 kDa antigen identified as human alpha-enolase, a glycolytic enzyme. They postulate that antigens aberrantly expressed in tumor cells of affected individuals trigger an immune response that cross-reacts with similar antigens in the retina causing cell damage. Further work by Adamus has led to the hypothesis that antibodies against recoverin and other retinal proteins such as alpha-enolase, are cytotoxic by triggering apoptosis via a caspase 3-apoptotic pathway.60–62 Therefore multiple antigens may be capable of inducing retinal damage and a clinical autoimmune retinopathy.6,58,63,64 There is a high degree of correlation between the presence of serum autoantibodies, the development of visual symptoms, and the presence of retinal degeneration.63
Cutaneous melanoma-associated retinopathy (MAR) syndrome
A paraneoplastic syndrome of acquired night blindness associated with rapidly developing vitiligo of the skin and uveal tract was reported in two patients with metastatic cutaneous melanoma.65,66 This process was described originally in 1984 by Gass as “an acute Vogt–Koyanagi–Harada-like syndrome.” These patients, like those with CAR syndrome, had ERG a and b waves that were markedly reduced in amplitude, indicating widespread photoreceptor cell dysfunction.
“Paraneoplastic acquired night blindness” has since been described in over 60 patients with cutaneous malignant melanoma and is being reported in a greater frequency than that of CAR syndrome.2,13,15,38,66–76 Melanoma-associated retinopathy (MAR) syndrome is thought to be a clinically distinctive subset of cancer-associated retinopathy. Specifically, this form of cancer-associated retinopathy is clinically differentiated from CAR syndrome by being nonprogressive, causing central visual loss (versus ring scotomas), a sensation of shimmering or pulsating light and being associated with vitiligo in up to 20%.66 In contrast to patients with CAR syndrome and the “acute Vogt–Koyanagi–Harada-like syndrome,” patients with MAR syndrome demonstrate a substantial elevation of rod absolute thresholds and selective reductions in the rod and cone ERG b waves, resembling those of patients with congenital stationary night blindness. The photoreceptor function is intact but signal transmission between the photoreceptors and second-order interneurons appears to be defective. MAR syndrome, unlike CAR syndrome, is more likely to be visually symptomatic in more advanced stages of disease and, in general, does not manifest before the clinical diagnosis of cutaneous malignant melanoma.2,75,77,78 Unilateral presentation of MAR has been reported over 18 months of observation but this may represent asymmetric ocular involvement.79 However, recent studies demonstrate that subclinical evidence for MAR may be present in earlier stages of cutaneous melanoma and this may portend a worse overall prognosis for the patient.78 Antibodies to retinal bipolar cells in MAR syndrome have been reported, but not against the 23 kDa CAR antigen.72,75,76 The nature of the bipolar cell antigen is not yet known but studies have verified that the bipolar cells are the primary site of pathology in this condition.80–82 Finally, antibodies against transducin, aldolase A and aldolase C have also been documented in patients with MAR.83,84
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


