Chapter 69 Angioid Streaks
Introduction
The appearance of angioid streaks was initially described by Doyne in 1889 as irregular and radiating lines extending from the optic nerve to the peripheral retina found in an eye with retinal hemorrhages after blunt trauma.1 The term “angioid streaks” originated as the ophthalmoscopic appearance of the lines was similar to that of blood vessels.2 Histopathologic studies found that angioid streaks represent irregular dehiscences in the collagenous and elastic portion of Bruch’s membrane.3,4 Associations have been found between angioid streaks and systemic conditions such as pseudoxanthoma elasticum (Grönbald-Strandberg syndrome),5,6,7 osteitis deformans (Paget’s disease),5,8–10 blood dyscrasias such as sickle-cell anemia,5,11–13 fibrodysplasia hyperelastica (Ehlers–Danlos syndrome),5,14 and acromegaly.5,15 However, angioid streaks may also occur in patients without associated systemic disease.16 Patients with angioid streaks usually are asymptomatic unless complications such as macular choroidal neovascularization develop.5,16 In cases of macular involvement the prognosis is often poor, with most eyes progressing to legal blindness without treatment.5,6,16 Multiple therapeutic strategies have been used to treat choroidal neovascularization secondary to angioid streaks, including argon laser photocoagulation,17–19 transpupillary thermotherapy,20 photodynamic therapy,21,22 macular translocation surgery,23–25 intravitreal antivascular endothelial growth factor treatments with pegabtanib,26 bevacizumab,27–33 or ranibizumab,33–38 and combination therapy.39
Histopathology
Angioid streaks represent discrete irregular breaks in Bruch’s membrane, and are often associated with atrophic changes of the overlying retinal pigment epithelium (RPE) and calcific degeneration.4 Klein proposed a dual mechanism for the development of Bruch’s membrane, including (1) a primary abnormality in the fibers of Bruch’s membrane and (2) increased deposits of metal salts or an increasing tendency for their pathologic deposition.3 The deposition of calcium may cause Bruch’s membrane to be more brittle and to develop choroidal rupture.4 Recent immunohistochemical studies show significant calcium deposition and infiltration of vascularized tissue above the RPE from Bruch’s membrane in the area of choroidal neovascularization in an eye with angioid streaks.40
Tissue metalloproteinase, specifically MMP-9, was found in high concentrations in the excised Bruch’s membrane in an area of choroidal neovascularization in an eye with angioid streaks. MMP-9 is known to induce basement membrane destruction and angiogenesis.40
In the early stages, angioid streaks are partial breaks of the thickened and calcified Bruch’s membrane with thinning of the RPE, events that do not cause anatomic changes in the overlying retinal layers.41 Subsequently a full-thickness defect of the Bruch’s membrane may occur followed by atrophy of the choriocapillaris, RPE, and photoreceptors. Fibrovascular proliferation from the choroid may occur through the Bruch’s membrane break resulting in choroidal neovascularization and subsequent development of a disciform scar.4,10,41 This process usually results in slowly progressive macular changes and vision loss. Sudden vision loss can result, however, from a serous or hemorrhagic detachment around the areas of choroidal neovascularization.4,10 Sudden loss of central vision may occur following mild trauma leading to choroidal rupture and submacular hemorrhage resulting from the brittleness of Bruch’s membrane.4,10
Systemic associations
Angioid streaks have been most commonly associated with systemic conditions such as pseudoxanthoma elasticum (Grönbald–Strandberg syndrome),5–7 osteitis deformans (Paget’s disease),5,8–10 fibrodysplasia hyperelastica (Ehlers–Danlos syndrome),5,14 acromegaly,5,15 Marfan syndrome,6 and blood dyscrasias such as sickle-cell anemia,11,12 thalassemia,6 and spherocytosis.6 Angioid streaks have also been described in patients with the following conditions: alpha-beta-lipoproteinemia, acquired hemolytic anemia, hemochromatosis, hypertension, diabetes, hypercalcinosis, hyperphosphatemia, diffuse lipomatosis, Sturge–Weber syndrome, tuberous sclerosis, neurofibromatosis, microsomia, epilepsy, senile elastosis, cutaneous calcinosis, and trauma5,6,16 (Box 69.1).
Box 69.1
Systemic conditions associated with angioid streaks
In a large study examining associated systemic diagnosis in 50 patients with angioid streaks, half of the patients were found to have a related systemic condition.5 Seventeen of the 25 patients were diagnosed also with pseudoxanthoma elasticum (PXE), 5 patients with Paget’s disease, and 3 patients had sickle-cell disease.5 The remaining half of the patients with angioid streaks did not demonstrate associated systemic disease.5
The most common systemic association of angioid streaks is PXE, an inherited disorder associated with degeneration of the elastic fibers in the dermatologic, gastrointestinal, cardiovascular, and ocular tissues. PXE accounts for 59–87% of cases with angioid streaks.7 In PXE, the primary finding is elastic fiber degeneration in connective tissue, followed by a secondary calcium deposition.4,10 In addition to angioid streaks, eyes also demonstrate a so-called “peau d’orange” pigmentary change, reticular pigmentary dystrophy affecting the macula, atrophic lesions of the RPE, crystalline bodies, and optic disc drusen (in 21% of patients with PXE and angioid streaks).42 By 20 years after first diagnosis, angioid streaks develop in almost all patients with PXE.16
In patients with Paget’s disease, extensive Bruch’s membrane calcification and angioid streaks followed by choroidal neovascularization and disciform scarring may develp.9,10 About 10% of patients with advanced Paget’s disease develop angioid streaks.9,10
Similar significant calcium depositions at Bruch’s membrane have been identified using histochemical and electron microscopic studies in patients with sickle-cell hemoglobinopathies.13 The presence of iron–calcium complexes at the level of Bruch’s membrane was previously suggested as an etiology for angioid streaks in patients with hemoglobinopathy; however, histopathologic studies demonstrate no increased iron deposition at the Bruch’s membrane.42 Compared to PXE, a smaller proportion of patients develop choroidal neovascularization and subsequent visual loss.6
Ocular manifestations and clinical course
Angioid streaks usually originate from the optic nerve and may either radiate out or surround it concentrically and appear as irregular lines of varying width.6 The subretinal lines can range in diameter from 50 to 500 µm.16 The color of angioid streaks varies based on the fundus pigmentation and tends to be reddish in light-colored individuals and brown-colored in darker-pigmented individuals16 (see Fig. 69.1A–D).
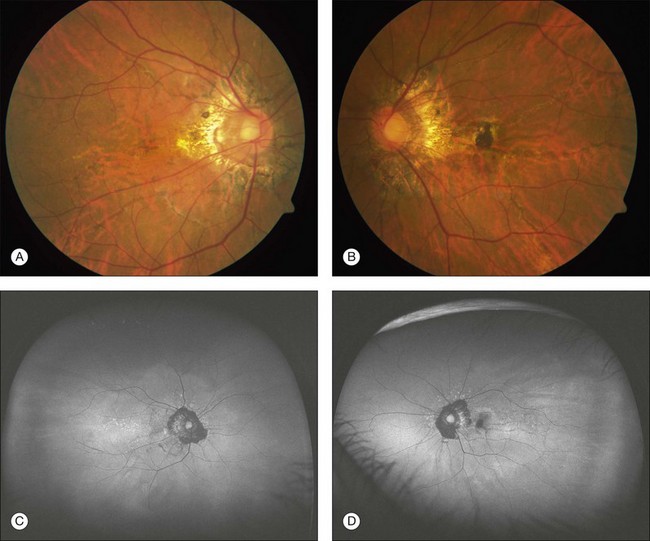
Fig. 69.1 A 63-year-old Asian woman with pseudoxanthoma elasticum and angioid streaks. Wide-field imaging of the right (A) and left (B) eyes shows angioid streaks (darker lines) radiating out from the optic disc. A hyperpigmented scar just nasal to the fovea developed after laser photocoagulation (A). The laser treatment was given prior to the use of intravitreal anti-VEGF therapy. Fundus autofluorescence imaging demonstrates the angioid streaks in the right (C) and left (D) eye. Spectral domain optical coherence tomography in this patient is shown in Fig. 69.3.
Angioid streaks have not been reported in newborns, and few cases have been described in individuals under 10 years of age.6 Angioid streaks remain over time and do not regress, and the streaks may increase in length and width over time.43 New streaks may form adjacent to old lesions. Over time, the adjacent RPE and choriocapillaris may develop atrophy.43
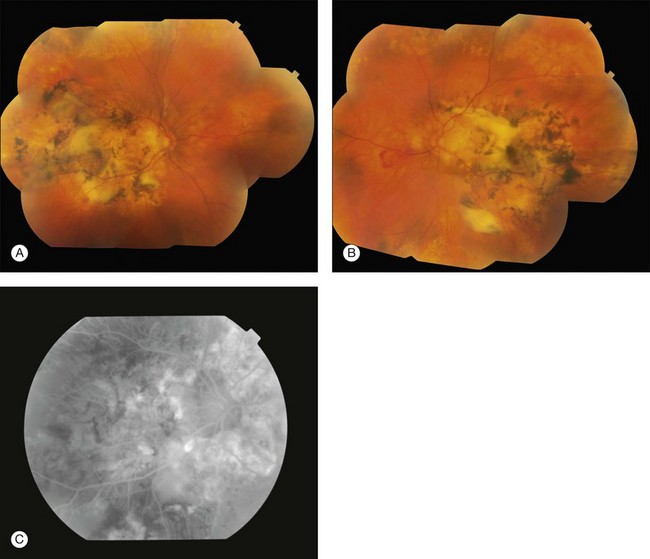
Most patients with angioid streaks are asymptomatic unless the macula is involved, with the development of traumatic rupture of the Bruch’s membrane or choroidal neovascularization (Figs 69.1B, 69.2A,B). If the macula is involved, patients may report metamorphopsia or blurred vision.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


