Chapter 85 Ocular Toxoplasmosis
Introduction
Toxoplasmosis is a common zoonosis caused by the infection with Toxoplasma gondii, and it is also the most important and frequent cause of infectious retinal disease and posterior uveitis. Toxoplasmosis can cause severe, life-threatening disease, specially in newborns and immunosuppressed patients but the majority of T. gondii infections in immunocompetent patients remain asymptomatic.1,2
In the eye it can cause blindness secondary to the retinitis present in the posterior pole of the eye or vitreoretinal complications in the acute or recurrent form of the disease.3 Ocular toxoplasmosis (OT) represents 50–85% of the posterior uveitis cases in Brazil and about 25% of cases in the United States.4 The prevalence of OT in the United States is not well determined but it ranges from 0.6 to 2% according to published reports and in Brazil, the prevalence ranges from 10 to 17.7%.5
Ocular toxoplasmosis may occur either in a congenital or a postnatal acquired form, and in both the eye may be affected during the acute phase of the infection or, more commonly, many months to years later.6 Many concepts related to OT have changed in the last years and are presented in Box 85.1.
Beef probably is not an important source of transmission; undercooked lamb, pork, and chicken are the common culprits as well as food and environment contaminated by the feces of infected cats. Transmission can also occur via organ transplantation and blood transfusion.7 Recently, water has been associated with the transmission of ocular toxoplasmosis on different continents.8
Fetal toxoplasmosis tends to occur only when the woman acquires the infection during or months before the pregnancy. The infection may be severe and is a frequent cause of abortion in the first months of pregnancy. When the fetus is infected, OT may become clinically apparent decades later and when it does, it presents bilaterally 85% of the time.9 Even women with IgG serum antibodies against toxoplasma may not be always protected against transmitting congenital toxoplasmosis to the fetus.10
Biology, life cycle, and transmission
Toxoplasma gondii is an obligate, intracellular protozoan parasite that undergoes a life cycle which includes both sexual and asexual reproduction. The sexual cycle occurs exclusively in felines, which shed a large number of infectious oocysts in their feces once in life, usually for a few weeks. Members of the cat family are its definitive hosts (hosts in which the parasite reproduces sexually), but hundreds of other species, including mammals, birds, and reptiles, may serve as intermediate hosts.11 The parasite can be found in the host’s tissues, such as muscles, retina, nervous system, and body fluids (saliva, milk, semen, urine, and peritoneal fluid).12
T. gondii exists in three forms: the oocyst, the tachyzoite, and the bradyzoite (also called the tissue cyst). Once the cyst is ingested by the intermediate hosts it causes disease with the production of tachyzoites. Under the pressure of the immune response the bradyzoites are formed. They are very resistant and may remain in the retina as well as the central nerve system and different muscles such as the tongue and heart for many years.13 The bradyzoites can remain dormant in the host for years without tissue damage and, for unknown causes, may rupture, causing reactivation of the ocular acute and recurrent disease.14
Strains/clonal populations: haplogroups genetics
The ability to identify parasite types may provide new insights into the pathogenesis of this disease, and genotyping ultimately may become an important diagnostic and prognostic tool.15
The majority of strains identified in Europe and North America are classified into three distinct genotypes (types I, II, and III). Type I strains are very virulent and types II and III strains are less virulent. All of them can cause disease in humans. Type I strains are considered to be more often associated with postnatal acquired ocular infections, and type II strains are more associated with congenital infections and toxoplasmic encephalitis.16 Atypical strains as well as mixed infections have been identified in many parts of the world and these atypical strains seem to be common in Brazil.17 The genetic make up of T. gondii is more complex than previously recognized and unique or divergent genotypes may contribute to different clinical outcomes of toxoplasmosis in different localities.18
Atypical toxoplasmic retinochoroiditis as well as variations in the clinical presentation and severity of disease have been attributed to several factors, including the genetic heterogeneity of the host and the genotype of the parasite responsible for infection.19
Pathogenesis
Serologic evidence of previous toxoplasma infection is present in 20–70% of individuals in different countries, depending on a variety of factors including climate, hygiene, and dietary habits. There is no consistent correlation between the prevalence of serum antibodies and the frequency of ocular disease.20 Different factors, such as the pathogenicity of the toxoplasmosis strains, may play an important role.21
Ocular toxoplasmosis in immunocompetent patients is characterized histologically by foci of granulomatous chorioretinal inflammation and coagulative necrosis of the retina with sharply demarcated borders. Inflammatory changes can be widespread in the eye and involve choroid, iris, and trabecular meshwork. Immunosuppressed patients with ocular toxoplasmosis have both tachyzoites and tissue cysts in areas of retinal necrosis and within retinal pigment epithelial cells.22 Parasites can occasionally be found in the iris, choroid, vitreous, and optic nerve. The lesions tend to be diffuse and often are active in both eyes.23,24
Ocular disease
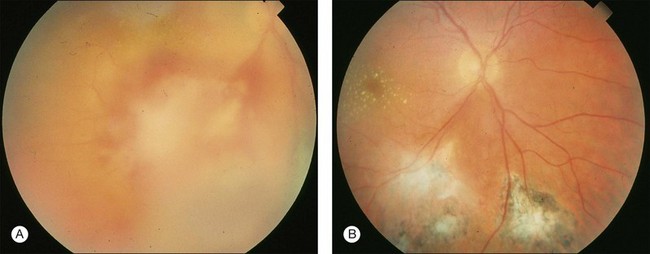
The retina is the primary site of T. gondii infection in the eye and the hallmark is a necrotizing retinochoroiditis satellite lesion adjacent to old hyperpigmented scars accompanied by vitreous inflammation and anterior uveitis. Retinal vasculitis is also present (Fig. 85.1). OT is characterized by recurrent episodes of necrotizing retinochoroiditis thought to be caused by the proliferation of live organisms that emerge from tissue cysts and/or an inflammatory reaction triggered by autoimmune mechanisms.25
The most common clinical signs of active ocular toxoplasmosis are blurring or loss of vision and floaters. Depending on the location of the lesions and the anterior chamber and vitreous inflammation patients can be more or less symptomatic.26
The diagnosis is clinical and suspected based on the ocular examination, the exclusion of the differential diagnostic entities (see below), and the presence of circulating antibodies for toxoplasmosis. It is important to perform both biomicroscopy and indirect ophthalmoscopy in both eyes. In special cases other procedures such as optical coherence tomography or fluorescein angiography may be necessary to diagnose and manage complications like macular edema and vasculitis.27 Toxoplasmic retinochoroiditis can be associated with severe morbidity if disease extends to structures critical for vision, including the macula and optic nerve, if there is damage to the eye from inflammation or if there are complications such as retinal detachment due to necrotic hole formation or tractional changes or neovascularization.28
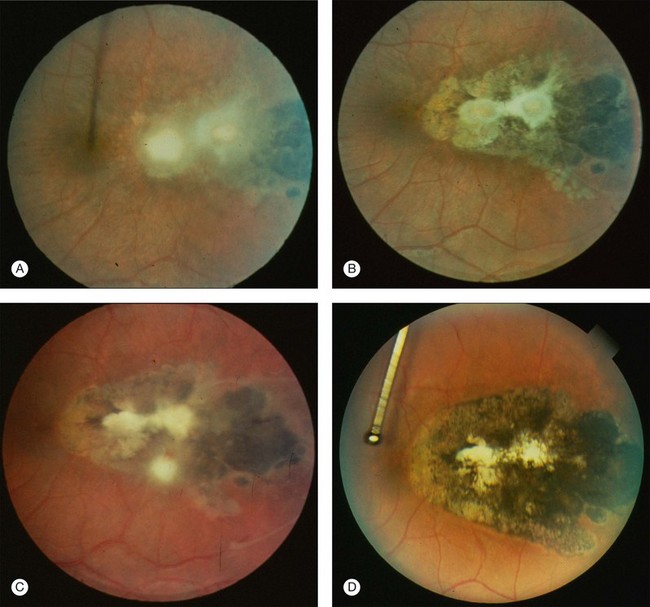
Recurrence frequency varies between individuals and is unpredictable, not only with respect to frequency but also regarding the retina site and its clinical presentation29 (Fig. 85.2).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


