CHAPTER 38 Noncaucasian Rhinoplasty
Anatomic Considerations
Although there are individual variations, most noncaucasian noses are anatomically characterized by thicker skin with abundant subcutaneous fibrofatty tissue, a weaker cartilaginous framework, short nasal bones, underdeveloped anterior nasal spine, low nasal sill, smaller quadrilateral septal cartilage, and inferior turbinate hypertrophy (Fig. 38-1). The associated cutaneous findings include a wide and underprojected dorsum, a low radix and nasion, a nasal tip that is bulbous, lacking definition, underprojected, and either ptotic or overrotated (short nose), with a short columella and an alar base that is wide and flaring (Table 38-1).1–4 The thicker skin can be an important differentiating feature because it allows for great acceptance of nasal implants, including alloplastic, and camouflages augmentation grafts in a more natural fashion. It also obscures minor changes performed on the cartilaginous framework, necessitating overcorrection as a rule.
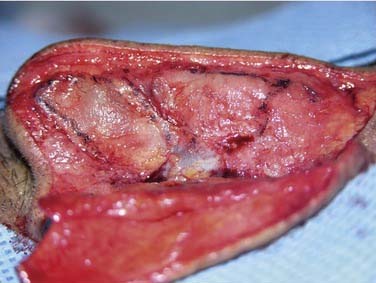
Figure 38-1. The anatomy of a typical noncaucasian nose. Note the weak cartilages, short nasal bones, and thick skin.
Table 38-1 Characteristics of the Asian Nose
| Site | Unique Characteristic |
|---|---|
| Radix | Low and inferior; short nasal bones |
| Dorsum | Underprojected, short |
| Tip | Bulbous, poor definition, underprojected, weak lower lateral cartilages |
| Ala | Thick, flared; with short columella |
| Skin | Thick |
| Septum | Straight, lesser quantity, thinner; small anterior nasal spine |
| Inferior turbinate | Hypertrophied |
In addition to the thicker tip skin, the lower lateral cartilages are weak and pliable, making the creation of tip definition a challenging task. Cephalic trim and dome binding sutures are often inadequate; reinforcing struts and projecting cap grafts tend to be more effective. The short columella merits some consideration when placing a transcolumellar incision for an external approach. Because the tip often requires some projection, one should place the transverse incision lightly lower, allowing it to rise with increased tip projection. Intranasally, most noncaucasian noses are characterized by a straight septum with widely patent internal nasal valves, large inferior turbinates, and a low bony nasal sill. The size of the quadrilateral septal cartilage is typically smaller and thinner, ironically leading to a dearth of desirable donor material in a setting where augmentation is often needed. Consequently, one of the primary sources of augmentation material in Asia remains alloplastic materials.5
The short and wide nasal bones make traditional osteotomies more challenging as the bone cuts easily drift into the ascending process of the maxilla.6–7 They also predispose to the inverted V deformity during the rare hump reduction. Fortunately, the wide internal valve and thick overlying skin make clinical nasal obstruction from this etiology a rare entity in noncaucasians.8 The flat nasal bones and nasal root extend inferiorly onto the cartilaginous dorsum. Therefore most patients require augmentation to the dorsum as well as the radix area.
Aesthetic Considerations
Cultural definitions of beauty vary widely and it is not the desire of all noncaucasians to acquire Occidental features, nor do the aesthetic norms of Western beauties transition to all ethnic faces. An attractive Asian nose, for example, has a slightly lower nasion, which is somewhat below the upper eyelash line. Textbook normative data of the radix and nasion describe the supratarsal crease for the caucasian face as the ideal landmark, best matching their angular topography. Asians have a flatter contour and the high radix would appear unnatural.9 Because the dorsum is often flat and wide, it occasionally also requires lateral osteotomies to narrow the bony aperture in addition to the dorsal augmentation. In regard to tip aesthetics, projection, rotation, and volume are the three most important factors to consider. These three factors influence one another in creating an ideal tip shape. The angulated tip with clear tip defining points is not the ideal appearance for most noncaucasians. A more rounded and lobular tip is preferred as it best blends with the cherubic facial shape and cheekbones. It is common for a retruded premaxilla to coexist with the small nose, creating a retrusive columella and an acute nasolabial angle. A plumping graft to efface the nasolabial angle can improve balance and create the illusion of tip rotation. A wide alar base with flaring of the alar lobules can be found in African-Americans and descendants of Southeast Asians (Filipinos, Malaysians). Northeast Asians (Japan, Korea) tend not to have the same degree of alar flaring.
Augmentation Rhinoplasty
Concept
Dorsal augmentation is a common task in the noncaucasian nose. Although the dorsum appears wide, lateral osteotomies are only rarely needed because the midline augmentation creates the illusion of narrowing. For many years in Asia, the alloplastic, L-shaped silicone strut was inserted to augment the dorsum and lengthen the short nose.10 The tension on the tip occasionally proved too much for even their thicker skin, and cover breakdown with subsequent implant extrusion were unfortunate sequelae. More recently, many surgeons use alloplastic materials for the dorsal upper two-thirds and autologous tissue to the tip region (e.g., tip or cap grafts, columellar struts, and caudal extension grafts).11–13
The surgical approach for augmentation rhinoplasty is largely influenced by the need for tip work. When only dorsal access is needed, an endonasal route is usually used, either through an intercartilaginous approach or via an extended septoplasty incision. When tip manipulation is required, the external approach can offer excellent control. This is particularly true when the tip is in need of projection and lengthening as well.14
Choice of Augmentation Material
There are numerous factors to consider before deciding which augmentation material to use, the amount of augmentation needed, the availability of septal and conchal cartilages, skin thickness, and certainly the patient’s preferences.11,12,15 The potential disadvantages of alloplastic implants are widely recognized, but the severity and likelihood of occurrence remains controversial. The risk of rejection and extrusion of alloplastic implants is of paramount concern, but contemporary porous materials, particularly when used under thicker, ethnic skin, may reduce that risk. Thorough patient education and informed consent is imperative during this preoperative consultation. Common alloplastic implants include Medpor (porous high-density polyethylene; Porex Inc., Newnan, GA), expanded polytetrafluoroethylene (ePTFE), and silicone (Fig. 38-2).

Patients in need of only a limited degree of dorsal augmentation are usually excellent candidates for autologous implants with septal or conchal cartilages. One must carefully inspect and palpate the septum to verify the presence of adequate cartilage. With revision rhinoplasties, the volume of native septal cartilage cannot be counted on and alternative sources should be planned. It is usually necessary to stack multiple layers of cartilage on one another, including ear cartilage. One should suture-secure the pieces of cartilage together, and carefully bevel all edges (Fig. 38-3A and B). Rib cartilage affords adequate volume to augment major deficiency of the dorsum as well as the rigidity needed to lengthen the nose through a caudal extension graft or strong L strut (see Fig. 38-3C).

Technical Considerations to Dorsal Augmentation
Harvesting autogenous cartilage grafts is often performed first. Septal cartilage harvest is readily performed and one must ensure an adequate dorsal and caudal strut (10 mm) and avoid disruption of the keystone area. Conchal cartilage is harvested through either an anterior or posterior approach. The skin and cartilage incisions are staggered such that a small rim of cartilage supports the closure of the skin. One preserves the root of the helix between the cavum concha and cymba concha, thus maintaining the shape of the auricle. Frequently, multiple layers of the septal and conchal cartilage are stacked and sutured together in order to obtain a desirable height. Particular attention must be made to carving of the edges of the grafts to ensure a smooth transition from the dorsum to the sidewall and at the nasion to avoid a step deformity there. The grafts can be fixed temporarily with two 25-G needles while incisions are closed (Fig. 38-4).

Rib cartilage is harvested from the sixth to eighth rib through a 3- to 4-cm skin incision. The incision is performed at the inframammary crease in women to camouflage the incision scar (Fig. 38-5
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


