CHAPTER 135 Neuroradiology of the Temporal Bone and Skull Base
External Auditory Canal
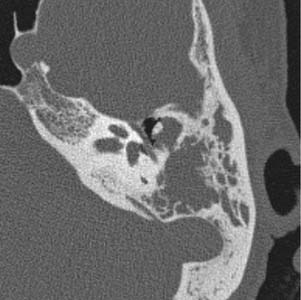
Congenital lesions rarely affect the EAC. The most common lesions are atresia of the EAC and first branchial cleft fistulas and cysts. Atresia and stenosis of the EAC is best evaluated with high-resolution CT (HRCT) of the temporal bones. The contribution of soft tissue and bony components of the stenosis or atresia is easily defined (Fig. 135-1). The presence of an EAC cholesteatoma behind the atresia plate can be determined. The middle ear may be hypoplastic, and typically the malleus and incus are fused into one ossicular mass that is connected to the stapes. The stapes may be malformed as well, and there may be an associated oval window atresia (Fig. 135-2).1–3 The position of the facial canal can be quite anomalous; the nerve tends to be dehiscent in the tympanic segment and can be overlying the oval window. The mastoid segment tends to run in a more anterior and lateral position, and the nerve can exit into the glenoid fossa or lateral to the styloid process. All of these anomalies are important in the assessment of the surgeon’s ability to perform an atresia repair.4
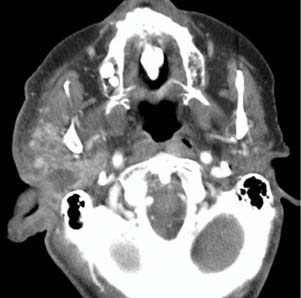
Imaging of severe infections affecting the EAC is generally used to assess for malignant or necrotizing otitis externa. This process typically involves the soft tissues and bone of the EAC, and extends into adjacent soft tissues. Findings on CT typically show soft tissue swelling in the EAC and auricle, with associated bony erosion and an osteomyelitic appearance of the inferior EAC. Contrast-enhanced CT shows enhancement of the soft tissues of the EAC and surrounding cellulitis and abscess (Fig. 135-3). The infection can spread in any direction, and can extend inferiorly to the parotid, masticator, and parapharyngeal spaces; posteriorly into the mastoid air cells; medially into the middle ear and petrous apex; and anteriorly into the temporomandibular joint. Rim-enhancing fluid collections can also be seen in these areas because associated abscesses can develop.
MRI of these lesions shows similar soft tissue thickening. Contrast-enhanced T1-weighted imaging shows diffuse enhancement of the auricle and EAC, with adjacent enhancement in cases with cellulitis, and rim-enhancing fluid collections in cases with abscess. T2-weighted imaging reveals diffuse high signal in areas of cellulitis.5,6
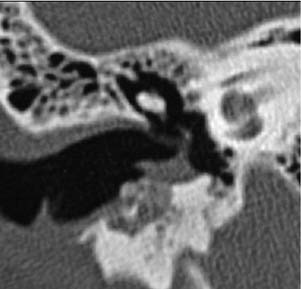
Inflammatory lesions of the EAC include cholesteatoma, keratosis obturans, and medial canal fibrosis. The hallmark imaging finding of cholesteatoma, regardless of location, is bony erosion. The typical imaging finding associated with EAC cholesteatoma is a homogeneous, erosive soft tissue mass in the EAC. These masses tend to occur predominantly in the inferior and posterior EAC. CT shows a soft tissue mass, with scalloped bone in the EAC with flecks of bone within the lesion itself (Fig. 135-4).7 Contrast enhancement is typically not helpful in these cases, but may show rim enhancement in cases with associated inflammation. CT is the study of choice for these lesions.
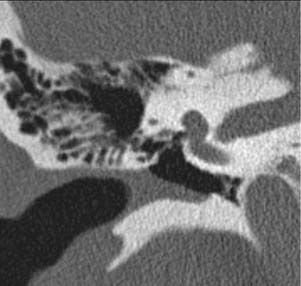
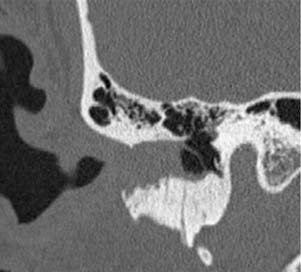
Keratosis obturans is an abnormal accumulation of keratinous debris within the EAC without erosive bony changes.8 This clinical entity can be confused with cholesteatoma, leading practitioners to perform imaging of the ear. HRCT reveals soft tissue filling the EAC, most typically with an intact tympanic membrane. The bony EAC may be enlarged, without scalloping or erosion of the osseous EAC itself (Fig. 135-5).9 Enhanced HRCT is not helpful in these cases.

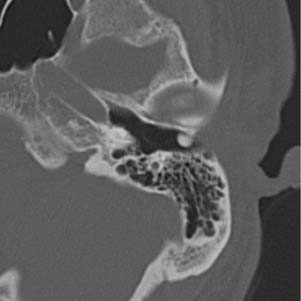
Postinflammatory medial canal fibrosis can be difficult to evaluate in the clinic because the ear canal becomes foreshortened and scarred. This entity is the sequela of chronic inflammation in the EAC, typically resulting from chronic otitis externa, but also can be of autoimmune origin.10,11 Nonenhanced HRCT with axial and coronal images is most helpful. One typically finds soft tissue in the medial one third to one half of the canal that is indistinguishable from the tympanic membrane without erosion or expansion of the bony ear canal (Fig. 135-6); this often has the appearance of a crescent. In the very early stages, there may be thickening of the tympanic membrane only, especially anteriorly. The middle ear and mastoid are not involved.
Benign neoplasms of the EAC include EAC exostoses and osteomas. Exostoses, also known as “surfer’s ear,” can be diagnosed without imaging, but are frequently seen on temporal bone imaging in some regions where cold water swimming is common. On HRCT, these lesions are typically circumferential bony overgrowths with normal overlying soft tissue that begin past the isthmus of the EAC (Fig. 135-7). These are almost always bilateral, and typically occur at the suture lines. EAC osteomas can be differentiated from these lesions by several distinct features. Similar to exostoses, they have normal overlying soft tissue, but they are typically ovoid in shape and less than 1 cm in size (Fig. 135-8). Usually discovered as an incidental finding, these lesions tend to be isolated, asymptomatic, and unilateral.

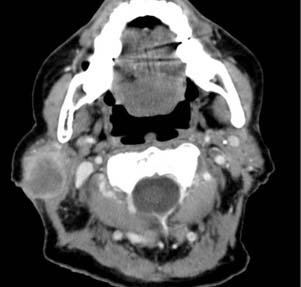
Malignant lesions of the EAC are uncommon, and are typically limited to local squamous cell carcinomas and the occasional metastatic carcinoma to the region. The imaging characteristics associated with squamous cell carcinoma are most commonly a soft tissue mass within the EAC with aggressive underlying bony changes. HRCT without contrast enhancement to delineate the bony extent of tumor and MRI with and without contrast enhancement to delineate the extent of soft tissue involvement are recommended for the radiologic evaluation of these lesions because the bony and soft tissue extent of tumor can impact surgical planning.12,13 HRCT shows the tumor and adjacent bony erosion, which are typically isolated to the EAC (Fig. 135-9). Contrast-enhanced HRCT may show a heterogeneously enhancing mass and spread to adjacent areas. These lesions tend to spread locally to the lining of the EAC and the auricle, sparing the middle ear. Regional metastases to the parotid and neck can be shown as enhancing nodes often greater than 1 cm in size (Fig. 135-10). MRI appearance of these lesions is generally low signal on T1-weighted imaging, which enhances peripherally with contrast medium. T2-weighted imaging commonly shows a heterogeneous high signal invasive lesion.13
Middle Ear and Mastoid
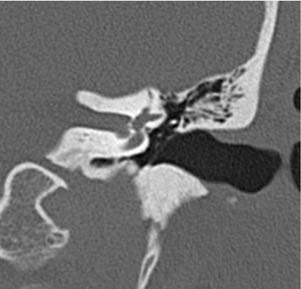
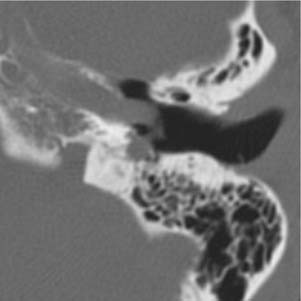
Common lesions affecting the middle ear and mastoid include cholesteatoma, glomus tympanicum, and an aberrant internal carotid artery. Cholesteatoma, although not strictly a radiologic diagnosis, does have specific radiologic characteristics. Congenital cholesteatomas are by definition found behind an intact tympanic membrane and can be very small, limited to the anterior tympanum, or, more rarely, can fill the entire tympanum and extend into the mastoid.14 CT without contrast enhancement shows a homogeneous soft tissue lesion, usually in the anterior tympanum adjacent to the eustachian tube with or without adjacent bony erosion (Fig. 135-11). As these lesions enlarge, they may fill the entire middle ear and erode the ossicles (Fig. 135-12), the fallopian canal, the tegmen, or the otic capsule. As the lesion extends posteriorly, it may widen the antrum and obstruct the mastoid air cells, which may be opacified by trapped secretions (Fig. 135-13).15
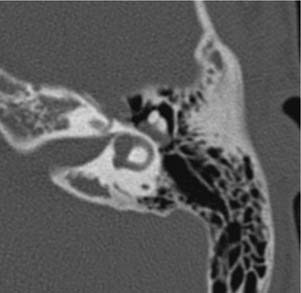
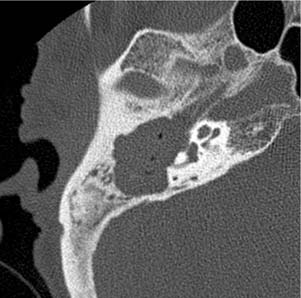
Figure 135-12. Axial CT image of the right middle ear shows a large cholesteatoma with complete ossicular destruction.
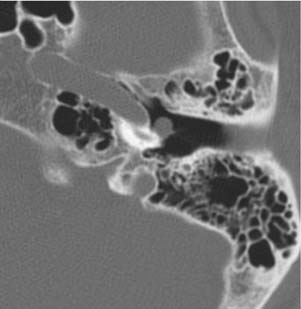
An acquired cholesteatoma has a different CT appearance because it develops in the epitympanum, eroding the scutum and ossicles (Fig. 135-14), and can extend posteriorly to involve the mastoid. MRI of any cholesteatoma is diagnostic because it has a characteristic appearance regardless of location on temporal bone. T1-weighted imaging shows an isointense to hypointense lesion (Fig. 135-15) that does not enhance, but may show a rim of enhancement (Fig. 135-16). T2-weighted imaging shows an intermediate or increased signal intensity lesion, occasionally with high signal secretions in the mastoid cavity (Fig. 135-17). Fluid-attenuated inversion recovery (FLAIR) imaging shows incomplete attenuation, whereas diffusion-weighted imaging shows restricted diffusion (Fig. 135-18).15 These imaging characteristics are typical of all cholesteatomas within the temporal bone, regardless of location.
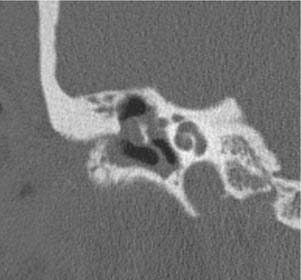
Figure 135-14. Coronal CT image of the right temporal bone shows scutum and ossicle destruction from a cholesteatoma.
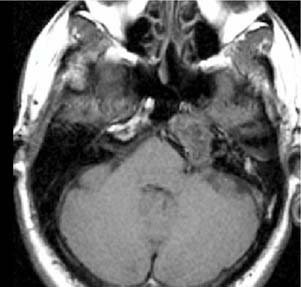
Figure 135-15. Axial T1-weighted noncontrast MR image through the temporal bone shows an isointense mass of the left petrous apex.
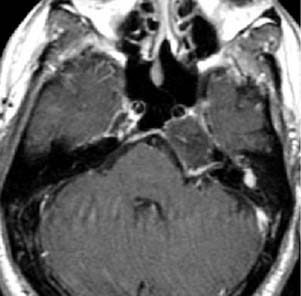
Figure 135-16. Axial postcontrast MR image through the left petrous apex in the same case as in Figure 135-15 shows a nonenhancing lesion with some peripheral enhancement.
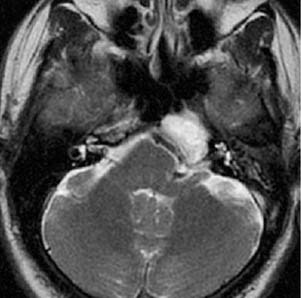
Figure 135-17. Axial T2-weighted MR image of the same case shows increased T2 signal intensity within the lesion.
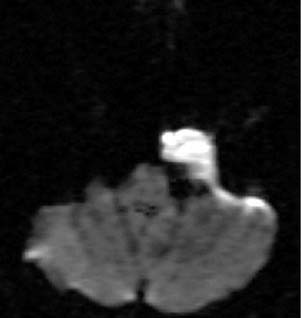
Figure 135-18. Axial diffusion-weighted MR image through the same lesion shows restricted diffusion (bright signal) consistent with a cholesteatoma.
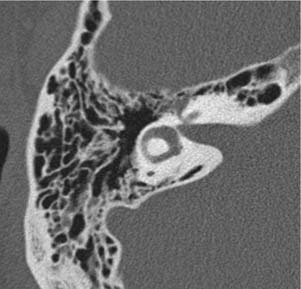
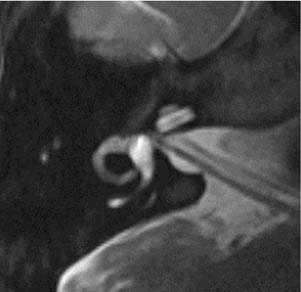
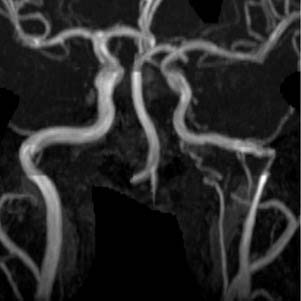
An aberrant internal carotid artery is a rare finding, but can be easily confused with a glomus tympanicum if careful attention is not paid to the imaging findings. Nonenhanced HRCT is diagnostic because it shows the characteristic enlargement of the inferior tympanic canaliculus, anterolateral to the jugular bulb, through which the carotid enters the middle ear (Fig. 135-19). From here, the carotid can traverse the middle ear, crossing the promontory and joining the petrous carotid through a dehiscence in the carotid canal. The carotid foramen and the vertical segment of the carotid are absent, with the aberrant carotid taking a more lateral position in the temporal bone.16 This lesion can be discriminated from a glomus tympanicum by the shape of the middle ear mass (tubular versus ovoid). A glomus tympanicum is limited to the middle ear space (Fig. 135-20). It is imperative to review the images in these cases carefully because the aberrant artery may appear to be an isolated ovoid middle ear mass if visualized only on one cut of the scan. MR angiography is also helpful in the diagnosis of the aberrant artery, showing a more lateral course of a narrowed internal carotid artery (Fig. 135-21).
Inner Ear
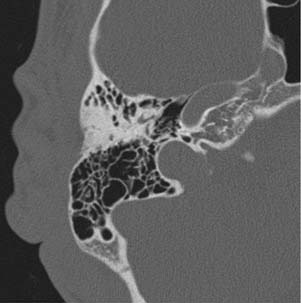
Imaging of the temporal bone can produce excellent visualization of the structures of the inner ear. The cochlea, vestibule, and semicircular canals all can be well visualized on HRCT (Fig. 135-22) and high-resolution T2-weighted MRI (Fig. 135-23). The diagnosis of superior semicircular canal dehiscence on imaging has improved significantly as higher resolution scans are acquired with submillimeter cuts and reconstructions in the plane of the superior semicircular canal that show the absence of bone over the canal (Fig. 135-24). In lieu of these reconstructions, the diagnosis is made by visualizing the lack of bone over the canal on three consecutive coronal cuts (Fig. 135-25).17,18 Congenital abnormalities of the inner ear can also be well defined using HRCT. Cochlear anomalies such as common cavity and cochlear hypoplasia are readily apparent (Fig. 135-26).