Chapter 82 Mycobacterial Infections
Introduction
Ocular mycobacterial infection represents an important form of extra pulmonary infection which encompasses tubercular (TB) as well as nontubercular mycobacterial (NTM) diseases in and around the eye. It presents with diverse clinical manifestations because of a number of factors that are related to the microbe and the host. In spite of recent revolutionary advances in diagnostic technologies, establishing the diagnosis as well as treating the disease are clinical challenges. Mycobacterial disease is known to have affected humans for more than a century and still it continues to be a global health concern. There are several challenges as far as TB is concerned. To list a few, TB stands as the most common opportunistic infection in HIV-positive patients in many developing countries. In 2009, 1.7 million people died from TB, including 380 000 people with concomitant HIV infection, which equates to about 4700 deaths a day.1 Yet another global threat is the emergence of multidrug-resistant (MDR-TB) and extensively drug-resistant strains of tuberculosis (XDR-TB). The World Health Organization has estimated there are 11.1 million patients with tuberculosis worldwide, of which 440 000 cases are due to MDR-TB. XDR-TB cases have been confirmed in 58 countries.1 A second important concern is the emergence of NTM infections, both in immune-competent and immune-compromised individuals in previously unrecognized settings and with new clinical manifestations.2 Clinical manifestations of NTM simulate typical tuberculosis. Lack of better laboratory tools for differentiation, lack of treatment guidelines, and resistance to routine antitubercular treatment challenge the early management of mycobacterial infections.
Pulmonary and extrapulmonary tuberculosis
Tuberculosis is an infection caused by a rod-shaped, non-spore-forming, aerobic bacterium, Mycobacterium tuberculosis. Bacilli spread by small airborne droplets from infected patients. Once the droplet nuclei are inhaled, the bacilli settle in the airways. If the infection is not contained by the immune system, in around 3–8 weeks, local spread and spread to regional lymph nodes in the lungs occur. Subsequent spread to other organs results in extrapulmonary tuberculosis (EPTB). EPTB is reported to be increasing over the last several years.3 Organs affected in EPTB include lymph nodes, pleura, central nervous system, eyes, musculoskeletal system, genitourinary tract and gastrointestinal tract. Symptoms and clinical presentations of EPTB are variable and depend on the organ involved. Unlike pulmonary TB patients, EPTB patients are less likely to present with cough, dyspnea, hemoptysis, abnormal chest X-ray, night sweats, weight loss, anorexia or fatigue. They may present with higher rates of abdominal pain, diarrhea, infertility, monoarticular joint pain or adenopathy depending upon the organ involved. Ocular tuberculosis represents an extrapulmonary dissemination of the bacilli primarily from lungs. However patients with ocular TB may have normal chest X-ray and negative chest complaints; alternatively they may have evidence of other forms of EPTB such as tubercular lymphadenitis. Ophthalmologists have to include appropriate questions in the history and consider extraocular systems whenever a tubercular etiology is suspected. It is essential to rule out EPTB and involvement of other systems in patients who may appear only to harbor pulmonary tuberculosis.
Ocular tuberculosis
Tuberculosis is one of the most common infectious uveitis in tropical countries.4–6 It is either unilateral or asymmetrically bilateral, characterized by a chronic and insidious course. Anatomically, tubercular uveitis may present as anterior, intermediate, posterior or pan-uveitis; it more often presents as granulomatous than nongranulomatous uveitis.
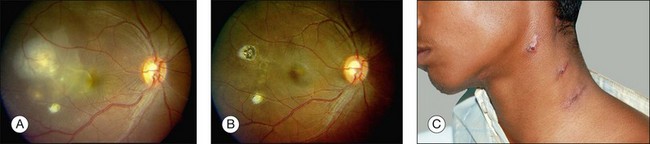
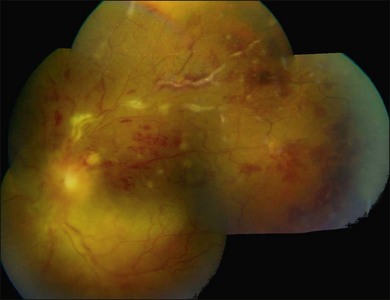
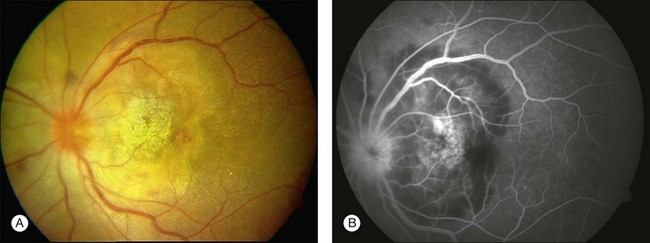
Three classic forms of ocular tuberculosis have been described. Direct ocular infection from an exogenous source may involve ocular adnexa, conjunctiva, sclera or cornea. The second form results from a hypersensitivity reaction to distant foci of infection causing episcleritis, phlyctenulosis, and occlusive retinal vasculitis of the type observed in Eales disease. The third form relates to the hematogenous spread of M. tuberculosis from pulmonary or extrapulmonary sites. The manifestations of this form of ocular tuberculosis are numerous (Figs 82.1 to 82.5), including lupus vulgaris, episcleritis, scleritis, necrotizing scleritis, posterior scleritis, interstitial keratitis, subretinal abscess, optic disc granuloma (Fig. 82.2), choroiditis, chorioretinitis, and choroidal granuloma (Fig. 82.3). Fundus fluorescein angiography may show a well-demarcated choroidal tubercle with initial hypo- and then late hyperfluorescence in such patients. Vessel wall staining, vascular leakage, disc staining and pooling of dye in the area of exudative detachment are other signs commonly seen in fluorescein angiography (Fig. 82.4B,C). Multifocal chorioretinitis with pigmented scars often indicates a tubercular etiology.4 Exudative retinal hemorrhagic periphlebitis (Fig. 82.2) in a patient with uveitis is highly suggestive of tubercular etiology. Healed periphlebitis results in sclerosed venules. Presence of perivascular healed chorioretinal scars in such patients would also suggest tubercular cause. Serpiginous-like choroiditis (SLC) of presumed tubercular etiology closely mimics classic serpiginous choroidopathy (SC) (Fig. 82.5A,B). Patients with SLC, however, are more likely to have multifocal scattered highly pigmented lesions with vitreous cells in contrast to classic SC, which is characteristically seen in the peripapillary area.4,5


Thus tubercular uveitis has a variable presentation, making the clinical diagnosis challenging. To help the clinician, a diagnostic criterion has been recommended. Diagnosis is considered as definitive TB only when the bacilli are isolated from the ocular tissues. The criterion for presumed tuberculous uveitis is reported to be presence of any one of the following clinical signs, such as choroidal granuloma, broad-based posterior synechiae, retinal vasculitis with or without choroiditis, or serpiginous-like choroiditis with a positive tuberculin skin test or QuantiFERON-TB Gold test, or any other relevant tests, such as chest radiograph and computed tomography.4 Good response to anti tubercular treatment and absence of recurrence further supports the diagnosis of presumed ocular tuberculosis.
Differential diagnosis
Granulomatous uveitis may also be seen in patients with herpes simplex or varicella zoster infection, phacoantigenic uveitis, sarcoidosis, syphilis, leprosy, Vogt–Koyanagi–Harada disease and sympathetic ophthalmia. Other causes of choroidal granulomas include syphilis, sarcoidosis, and fungal lesions.4,5
Pathogenesis
Tissue damage in ocular tuberculosis is not only a direct consequence of infection but it is also due to non-resolving inflammation that results from a sensitive balance between protective immunity and destructive pathology.7 Molecular studies and sequencing of the M. tuberculosis genome have identified specific and highly immunogenic antigens. These are the so-called 6 kDa early secretory antigenic target (ESAT-6) and the 10 kDa culture filtrate protein (CFP-10). They are capable of eliciting vigorous helper T-cell responses with resultant cytotoxicity in cellular models. They cause cell lysis and may enable the bacteria to invade and spread within the alveolar epithelium. Recent studies indicate ESAT-6 may also stimulate the trafficking of infected macrophages into the granulomas, to utilize the granulomas as foci of macrophage recruitment, infection, and subsequent bacterial dissemination.
Host genetic factors appear to play a role in disease severity. Abnormalities in the genes encoding the interferon-gamma receptor chain and genes encoding interleukin-12 are important in determining the susceptibility to disseminated mycobacterial disease.8 Pulmonary alveolar macrophages express complement and toll-like receptors and destroy the bacteria when they fuse with lysosomes. However, the mycobacteria can inhibit fusion with lysosomes, and may then thrive in the phagosome. Retinal pigment epithelium (RPE) shares several functions with the macrophages, including expression of toll-like receptors, complement, and phagocytosis of bacteria. Clinicopathologic study combined with molecular analysis revealed distribution of the mycobacteria in the RPE even though the retina and uvea were involved with the inflammatory process. The authors suggest a possibility of reactivation of sequestered organisms in cases of recurrent inflammation.9
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


