, Jacques Magnan3, Hassan Haidar4, Karen Nicolas5, 6 and Stéphane Louryan7
(1)
Hospital Sacre Coeur ORL Chirurgie Cervico – Faciale, Lebanese University, Baabda, Lebanon
(2)
ORL Chirurgie Cervico – Faciale, Hôpital Trad, Beirut, Lebanon
(3)
ORL – Chirurgie Cervico – Faciale, University Aix-Marseille Hôpital Nord, Marseille, France
(4)
ORL – Chirurgie Cervico – Faciale, Hôpital Nord, Marseille, France
(5)
Department of Radiology Middle East Institute of Health, Bsalim Levant Clinics, Fachaerztin fuer Radiologische Diagnostik Lebanese University, Beirut, Lebanon
(6)
Department of Radiology, Levant Clinics, Sinn el Fil, Lebanon
(7)
Laboratoire d` Anatomie Biomécanique et Organogenèse, Université Libre de Bruxelles Faculté de Médecine, Brussels, Belgium
3.4.1 Facial Nerve Branches
3.4.2 Tympanic Plexus
3.6.2 Mucosal Folds Anatomy
3.6.3 The Tympanic Diaphragm
3.6.4 The Tympanic Isthmus
Abstract
Traditionally, the ossicular chain is considered as the essential content of the middle ear. It is suspended inside the cavity by ligaments and muscles, which will be addressed in their embryological development and their anatomical details in this chapter.
Nowadays, it is admitted in middle ear mechanics that the most important content of the middle ear to assure a normal sound transmission, in addition to the ossicular chain, is gas (air).
The tympanic cavity contains an average of 2 cc of air. The minimal volume of air necessary for a normal function of the middle ear is at least 0.5 cc. Air transmits the sound wave from outside to the tympanic membrane and inside the middle ear to both the oval and the round windows. Air in the middle ear serves also as an insulator. When air of the middle ear is replaced by an effusion, hearing loss will result due to the reduction of pressure difference of the sound wave in between the oval window and the round window with an escape of sound energy to the surrounding bony structures.
Traditionally, the ossicular chain is considered as the essential content of the middle ear. It is suspended inside the cavity by ligaments and muscles, which will be addressed in their embryological development and their anatomical details in this chapter.
Nowadays, it is admitted in middle ear mechanics that the most important content of the middle ear to assure a normal sound transmission, in addition to the ossicular chain, is gas (air).
The tympanic cavity contains an average of 2 cc of air. The minimal volume of air necessary for a normal function of the middle ear is at least 0.5 cc. Air transmits the sound wave from outside to the tympanic membrane and inside the middle ear, air serves as an insulator. When air of the middle ear is replaced by an effusion, hearing loss will result due to the reduction of pressure difference of the sound wave in between the oval window and the round window with an escape of sound energy to the surrounding bony structures.
Furthermore, the middle ear cavity contains several mucosal folds that divide the middle ear cavity in different compartments and spaces. The folds and their openings define middle ear aeration pathways and play an important role in the evolution of some middle ear pathologies, such as inflammation or cholesteatoma.
3.1 The Auditory Ossicles
The auditory ossicles are the malleus, incus, and stapes; they are named after the objects they resemble (hammer, anvil, and stirrup). The ossicles are suspended in the middle ear cavity by numerous suspensory ligaments, and they are covered by the mucous membrane of the middle ear cavity. The auditory ossicles form the ossicular chain which is responsible for transmission of sound-induced vibrations of the tympanic membrane to the oval window. This system is the cornerstone of middle ear mechanics.
3.1.1 Embryology of the Auditory Ossicles
The ossicles, muscles, and tendons of the middle ear are formed from the mesenchyme of the middle ear and are covered by the epithelial lining of the first pharyngeal pouch [1].
The mesenchyme forming the ossicles is derived from neural crest cells present in the first and second branchial arches. These cells migrate to the branchial arch from the dorsal part of the developing neural tube during the fourth week of gestation [2].
There is controversy about the contribution of each arch to ossicular formation; there are two main theories regarding this subject:
The classical theory: postulates that the incus and the malleus are derived from Meckel’s cartilage of the first branchial arch; the stapes is derived from Reichert’s cartilage of the second branchial arch [3–7].
The alternative theory: proposes that the head of the malleus and the body of the incus originate from the first arch, while the handle of the malleus, the long process of the incus, and most of the stapes originate from the second arch (Fig. 3.1) [8–13].
Fig. 3.1
Destination of the first and the second branchial arches. M malleus, I incus, S stapes, AP anterior malleal process, (*) double origin of the footplate
In both theories, the labyrinthine side of the footplate was considered to originate from the mesenchyme of the otic capsule. However, some normal and teratologic observations in the literature support the idea that the stapes could entirely derive from the Reichert’s cartilage without any contribution of the otic capsule [14–16].
Ossicular development in the human embryo starts at the fourth week of gestation as an interbranchial mesenchymal bridge connecting the mesenchyme of the upper part of the first branchial arch and the central part of the second branchial arch. This condensed mesenchyme gives rise to the primordial malleus and incus [12, 17, 18]. This mesenchymal mass is crossed by the chorda tympani that divides it in two parts: the malleal primordium laterally and the incudal primordium medially (Fig. 3.2). This common rudiment keeps connection with the Reichert’s cartilage, supporting the “alternative” theory in that all of the stapes blastema derives from the second arch mesenchyme.
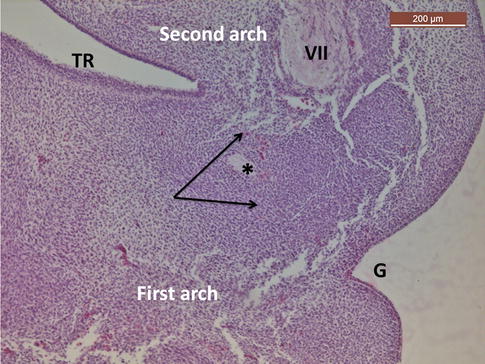
Fig. 3.2
13-mm human embryo. The common blastema of the handle of the malleus and the long crus of the incus (the two arrows) crossed by the chorda tympani (*). TR tubotympanic recess of the first branchial pouch, G first ectodermal groove, VII facial nerve in the second branchial arch. Hematoxylin-eosin staining
During the sixth week, a precartilage forms in the future ossicles. A rapid transformation into true cartilage occurs during the seventh week. By the end of the eighth week, the cartilaginous malleus resembles adult ones. Thereafter, progressive and extensive ossicular growth occurs and, by the 20th week, the ossicles reach adult size and have begun to ossify.
Ossification of the incus takes place slightly earlier than that of the malleus. In the 25th to 26th week, both the incus and malleus are fully ossified with the exception of the distal extremity of the malleus handle. Meanwhile, the pneumatization process of the tympanic cavity extends into the epitympanum and antrum, making the ossicles free only tethered to the tympanic cavity in a mesentery-like fashion.
Clinical application
Before birth, the ossicles have achieved adult size and shape. The endochondral bone of the ossicles, similar to that of the otic capsule, undergoes only little changes over lifetime of the individual and demonstrates poor reparative capacity in response to fractures.
3.1.1.1 Stapes Development
The stapes, the first ossicle to appear, develops from an independent anlage derived from the cranial end of the cartilage of the second branchial arch (Fig. 3.1). The stapedial anlage connects to the remaining Reichert’s cartilage by a formation called the interhyale; the internal part of the interhyale gives rise to the tendon of the stapedial muscle.
The stapedial anlage will be crossed by the stapedial artery during embryonic period, giving the stapes its characteristic ring shape (Fig. 3.3).
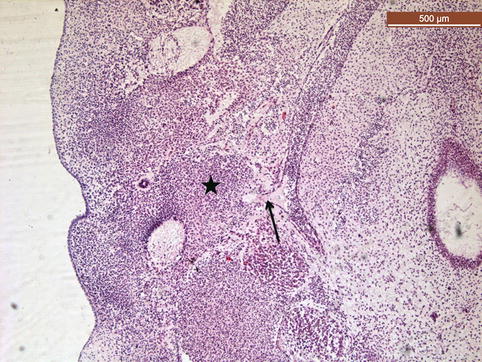
Fig. 3.3
13-mm human embryo section showing the stapedial (*) rudiment crossed by the stapedial artery (arrow). Hematoxylin-eosin staining
3.1.1.1.1 Footplate Development
There are two theories regarding the origin of stapedial footplate. Despite the fact that there are several differences between both theories, it is accorded that footplate development is characterized by a progressive replacement of undifferentiated mesenchyme by chondroblasts, and differentiation of the peripheral mesenchyme into the annular ligament around the presumptive footplate, as demonstrated by Jacksoll in the chick embryo [19] (Fig. 3.4).
Fig. 3.4
Footplate development in the bird (According to Jaskoll 1980 [19]. (a)–(f): Successive stages of development of the footplate and related structures. This material is reproduced with permission of John Wiley & Sons, Inc.). Chondroblasts of the otic capsule and stapes are initially separated by undifferentiated mesenchyme. This mesenchyme progressively disappears and becomes present in the “isthmus” (arrows) in which will develop the annular ligament. FP footplate, AL annular ligament, OC otic capsule
Classical theory of footplate origin
The classical theory presumes that the footplate has two origins: the tympanic side derived from the stapedial ring and the vestibular side derived from the lamina stapedialis of the otic capsule [16]. The medial border of the stapedial ring comes in contact with a facing depression in the lateral wall of the otic capsule. This depression, called the lamina stapedialis, is the future oval window. The medial border of the stapedial ring fuses with the lamina stapedialis to form the stapedial footplate (Fig. 3.5).
Fig. 3.5
Stapes development according to the classical theory
Alternative theory of footplate origin
According to this theory, the otic capsule is not involved in the formation of the base of the stapes and the entire stapes derives from the stapedial anlage of the Reichert’s cartilage [14, 15, 19, 20] (Fig. 3.6).

Fig. 3.6
E16 mouse embryo whose mother received a teratogen molecule (methyl triazene) disturbing ossicles formation. A complete stapes develops independently from the otic capsule (arrow). In front of the stapes, we observe a narrowing of the otic capsule cartilage. Toluidine blue staining at pH2
3.1.1.1.2 Annular Ligament
At the beginning, the footplate is attached to the otic capsule by a band of mesenchyme that later transforms into the annular ligament, once the footplate reaches adult size [19, 20]. The stapediovestibular joint, stapes and the inner ear being decoupled, shows its definitive characteristics at 12th week (Figs. 3.4 and 3.5).
3.1.1.1.3 Stapes Ossification
Stapes endochondral ossification starts at the end of the fourth month from a single ossification center present at the center of the footplate. The ossification extends to the two branches and then to the head of the stapes [21].
Clinical application
Congenital stapes anomalies are sometimes related to an aberrant facial nerve development. During the crucial time period of sixth week, anterior displacement of the second genu region of the facial nerve hinders the normal fusion of the stapedial ring with the lamina stapedialis, resulting in a malformed stapes in conjunction with anomalous facial nerve trajectory.
3.1.1.2 Incus Development
The incus is the second ossicle to appear, but the first to be ossified. The body of the incus derives from the cranial part of the Meckel’s cartilage. The long process of the incus derives from Reichert’s cartilage (Figs. 3.1 and 3.7). Endochondral ossification starts at the beginning of the fourth gestational month from the anterior face of the long process and ends at the sixth month reaching adult size.
Fig. 3.7
Sagittal section of E17 mouse embryo displaying the cartilaginous malleus (M), incus (I), and stapes (S) in close relationship with the otic capsule (O). The incudomallear joint is just forming (*). Toluidine blue staining at pH4
3.1.1.3 Malleus Development
The head of the malleus (Figs. 3.1, 3.7, and 3.8) appears as a mass connected to the cranial end of the Meckel’s cartilage. This connection disappears later to be replaced by the anterior process of the malleus and anterior malleal ligament. The anterior process, which can be up to 10 mm in neonates, remains in the adult malleus only as a small prominence. A lack of bony involution can keep the malleus fixed at the petrotympanic fissure [24].
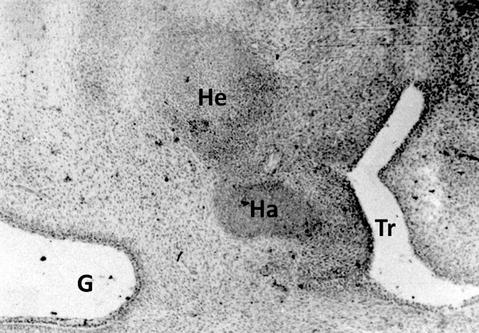
Fig. 3.8
Coronal section of a 19-mm human embryo revealing the coalescence of the handle of malleus (Ha) and the head of malleus (He). The handle projects between the first ectodermal groove (G) and the first endodermal pouch (TR). At this stage, the ossicles are cartilaginous. Hematoxylin-eosin staining
The handle of the malleus has close relationships with the long process of the incus in a blastema originally connected to the Reichert’s cartilage. Failure of resorption of this connection with Reichert’s cartilage leads to formation of malleus handle bony bar (see Sect. 3.1.1.4). Later, the handle of malleus becomes inserted in the tympanic membrane rudiment.
This different origin of the head and of the handle of the malleus explains why in aural atresia the head of the malleus is present while the handle is missing. Malleus ossification ends by the sixth month [25].
Congenital Ossicular Malformations
Congenital ossicular malformations could be associated with aural atresia and microtia, or it could be isolated without external ear anomaly as in minor ear atresia. Ossicular anomalies in minor atresia are subdivided into incudomalleal fixation, stapes fixation, and incudostapedial disconnection [26]. Incudomalleal fixations are the least common, where the malleus head and incus body are usually fused or fixed to the epitympanic walls [27]. Triple ossicular malformations are rare and could be associated with inner ear anomalies [28].
Malleus Congenital Anomalies
The incidence of malleus anomalies is lower than anomalies of the incus or stapes. Hypoplasia or aplasia of the malleus results from a failure of embryogenesis between 7th and 25th week. Given the common pharyngeal arch origin, hypoplasia of the malleus is often associated with hypoplasia of the incus [22].
Epitympanic fixation of the head of malleus is by far the most congenital anomaly of the malleus. This anomaly is related to an incomplete pneumatization of the epitympanum during malleus head ossification. Temporal bone exploration in these patients reveals bony bridges between the head of the malleus and the lateral epitympanum in the majority of cases [24, 27] (Fig. 3.9).
Fig. 3.9
(a) Transversal computed tomography of a right ear: bony bridge (arrow) between the malleus head and the tegmen. (b) Transversal computed tomography of a left ear with fixation of the incus on the medial attic wall (black arrow), malleus head (white arrow)
Incus Congenital Anomalies
Hypoplasia or aplasia of the incus typically occurs in conjunction with hypoplasia of the malleus but may occur in isolation. The incus is also susceptible to fixation to the epitympanum (Fig. 3.9). Congenital absence of the long process of the incus might be associated with aplasia of the stapes and of the handle of malleus, supporting the hypothesis of their common origin [22, 23] (Fig. 3.10).
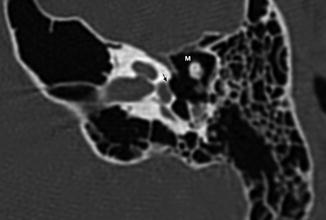
Fig. 3.10
Computed tomography of a left ear with aplasia of stapes suprastructure and the long process of the incus. M malleus; stapes footplate (arrow)
Stapes Congenital Anomalies
Congenital stapes footplate fixation is the most common isolated ossicular anomaly, approximately 40 % of all congenital ossicular malformations. It is thought to result from ossification of the peripheral mesenchyme of the footplate instead of differentiating into the annular ligament [31].
Although aplasia of the stapes is rare, multiple forms of hypoplasia that include small or absent crura and blob-like stapes have been described. In contrast, isolated hyperplasia of the stapes is often an incidental finding that does not require therapy; this anomaly is thought to result from a failure of the resorption and remodeling that occurs during the final stages of stapes development. Several crural anomalies have been described, including thin, absent, fused, and angled crura. The crura may also be replaced with a columella-like structure. Congenital stapes disorders are often related to aberrant facial nerve development [10, 22, 32].
3.1.2 Anatomy of the Auditory Ossicles
3.1.2.1 The Malleus
The malleus is shaped like a hammer and is the largest of the three middle ear ossicles. It is 8–9 mm in length and weighs about 20–25 mg. It consists of a head, neck, handle, and two processes arising from below the neck (Fig. 3.11).
Fig. 3.11
Schematic drawing of the malleus
3.1.2.1.1 The Malleus Head
The malleus head lies in the attic region of the middle ear and is 2.5 by 2 mm in size. On its posteromedial surface, there is an elongated saddle-shaped facet to articulate with the incus. This facet is covered by an articular cartilage.
Malleus head Fixation
Malleus head fixation is not an uncommon pathology. It may be a congenital anomaly (Fig. 3.9) or acquired anomaly as in tympanosclerosis (Fig. 3.12). Clinically it manifests as a 15–25-dB conductive hearing loss [33].
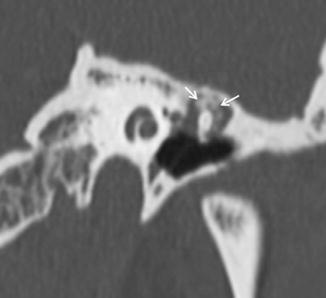
Fig. 3.12
Attical tympanosclerosis of a left ear, computed tomographic coronal reconstruction showing calcifications (tympanosclerosis, arrows), surrounding and fixing the malleus to the tegmen
3.1.2.1.2 The Neck
The neck is a narrow and flattened portion. The tendon of the tensor tympani muscle inserts on its medial surface, and the chorda tympani crosses its medial surface above the insertion of this tendon. Its lateral surface forms the medial wall of the Prussak’s space.
3.1.2.1.3 The Manubrium (The Handle)
The handle forms with the malleus head a supero-posteriorly open angle of 135–140°. It runs downwards, medially, and slightly backwards between the mucous and fibrous layers of the tympanic membrane. The inferior end of the handle is flattened and firmly attached to the tympanic membrane as the pars propria splits to envelop it forming the umbo.
In surgical procedures, the tympanic membrane can be readily separated from the malleus except at the umbo. At the level of the umbo, the periosteum of the handle continues directly with the fibrous layer. Midway between the lateral process and the umbo, the handle has a gentle medial curvature. At this level the handle is not embedded in the tympanic membrane, rather it is linked to the tympanic membrane by a mucosal fold, the plica mallearis. A prosthesis clamped to the manubrium in this area may have little or no contact with the pars propria of the normal tympanic membrane and therefore present a very low risk of extrusion (Fig. 3.13).
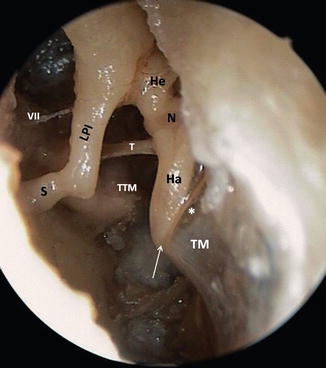
Fig. 3.13
Posterior view of a right middle ear cavity. The inferior end of the handle (Ha) is firmly attached to the tympanic membrane (TM) forming the umbo (white arrow). Relation of the middle part of the handle and the lamina propria of the tympanic membrane (black arrow). Plica mallearis (*). LPI long process of the incus, S stapes, N neck of the malleus, He head of the malleus, VII facial nerve, TTM tensor tympani muscle, T tensor tympani tendon
Clinical application
Usually the handle lies midway between the anterior and posterior borders of the tympanic membrane, but may occupy a more anterior position. Surgical procedures on the tympanic membrane are especially difficult when an anteriorly located malleus is associated with bulging of the anterior canal wall. Rarely, the malleus handle is fixed to the posterior tympanic wall by a bony bar, a malleus bar [29, 30, 32].
3.1.2.1.4 Malleus Processes
The malleus has two processes located at the union of the neck and the malleus handle.
The lateral process
The lateral process is a small conical eminence of 1 mm. It protrudes laterally to the side of the tympanic membrane and gives attachment to the anterior and posterior tympano-malleal ligaments.
The anterior process (processus gracilis)
The anterior process is a 3–5-mm long thin bony spine which extends from the neck of the malleus into the petrotympanic Glaserian fissure. On its medial aspect runs the chorda tympani nerve to enter anteriorly the petrotympanic fissure. It gives origin to the anterior malleal ligament, which also traverses the petrotympanic fissure to reach the angular spine of the sphenoid bone. An extremely long anterior process extending into the petrotympanic fissure may hinder the free movement of the malleus, with little impact on hearing, about 5-dB hearing loss.
3.1.2.1.5 Malleus Ligaments (Fig. 3.14)
Fig. 3.14
Schema showing malleal ligaments and tensor tympani muscle tendon (TTM). SSL superior suspensory ligament, ASL anterior suspensory ligament, LSL lateral suspensory ligament, AML anterior malleal ligament, PML posterior malleal ligament. The AML and PML in blue color represent the axis of rotation of the malleus
The malleus is stabilized in place by five ligaments, one articulation, one tendon, and the tympanic membrane. Three of the five ligaments are outside the axis of rotation: they offer only a suspensory function. They are:
The anterior suspensory ligament (ASL) lies superior to the anterior malleal ligament and attaches the head of the malleus to the anterior wall of the epitympanum.
The lateral suspensory ligament (LSL) attaches the neck of the malleus to the bony margins of the tympanic notch (the notch of Rivinus) and forms the superior wall of the Prussak’s space.
The superior suspensory ligament (SSL) bridges the gap between the head of the malleus and the tegmen of the epitympanum and carries the superior tympanic artery branch of the middle meningeal artery.
These three ligaments apparently do not interfere with sound transmission because of the small movements of the ossicles at their points of attachment. The suspensory ligaments do not play a role in middle ear mechanics.
The anterior malleal ligament (AML) together with the posterior incudal ligament serves to establish the axis of rotation of the ossicles. The anterior malleal ligament must not be confused with the anterior suspensory ligament of the malleus. The anterior malleal ligament extends from the angular spine of the sphenoid bone, passes through the petrotympanic fissure, accompanied by the anterior tympanic artery, and inserts on the neck of the malleus at the base of the anterior process of the malleus.
The posterior malleal ligament (PML) extends from the neck of the malleus to the posterior tympanic spine.
3.1.2.2 The Incus (Fig. 3.15)
Fig. 3.15
Schematic drawing of the incus. Pe lenticular process pedicle, Pl lenticular process plate
The incus measures about 5 by 7 mm and weighs about 30 mg. It has a trapezoidal body, short process, long process, and a rounded lenticular process.
3.1.2.2.1 Body of the Incus
The body of the incus is flat. Its anterior surface houses an elliptical articular surface to receive the head of the malleus. Both body of the incus and the head of the malleus are situated in the attic. Two spines arise from the lower posterior part of the body, the long and short processes. These two processes diverge from each other in a right angle:
3.1.2.2.2 Short Process of the Incus
The short process of the incus extends posteriorly from the body as a thick and triangular process; its major axis is horizontal. Its dorsal end lies on the incudal fossa situated in the floor of the aditus ad antrum.
3.1.2.2.3 Long Process of the Incus
The long process or vertical process of the incus follows a direction similar to the handle of the malleus but in a more posterior and medial plane. Its caudal end forms a hook at a right angle to end up with the lenticular process. The horizontal, cross-sectional configuration of the long process of the incus is circular, in contrary to the ovoid shape of the manubrium of the malleus. The mean diameter of the distal extremity of the long process is 0.63 mm [34].
Because of its terminal and poor vascularization, the long process of the incus is highly susceptible to osteitic resorption secondary to several conditions such adhesive otitis media or extremely tightened stapes prosthesis.
3.1.2.2.4 Lenticular Process
The lenticular process connects the long process of the incus to the head of the stapes. The lenticular process consists of a narrow bony pedicle and a flattened distal plate.
The bony pedicle is surrounded by a joint capsule of thick fibers. The mean diameter of the bony pedicle (0.26 mm) is less than half of the mean diameter of the distal long process (0.63 mm) and less than half of the mean diameter of the distal plate (0.71 mm) [34]. The bony pedicle is flexible and plays a role in the piston-like transmission of the incus movement to the stapes, lateral to medial, by the rotation movement of the incus. All other movements are reduced by the bending of this pedicle before reaching the stapes [35].
Clinical Application
Chronic otitis media (COM) is the most common cause of ossicular chain necrosis and concerns most frequently the long process of the incus (Fig. 3.16). It is the most vulnerable part of the ossicles because of its poor blood supply [36–38]. The malleus and the footplate are more resistant to necrosis [37, 38]. The blood supply of the long process of the incus is provided by end vessels, which descend down along the long process of the incus. Persistent or repeated infection in some cases of COM, or pressure from a severely retracted eardrum in chronic adhesive otitis media, or over-crimped stapes prosthesis, combined with the lack of collateral blood supply, is thought to be the cause of aseptic necrosis [36]. Occasionally dissolution is complete with total incudostapedial separation, but more frequently slow dissolution leads to replacement of the bone by a fibrous tissue [37, 38].
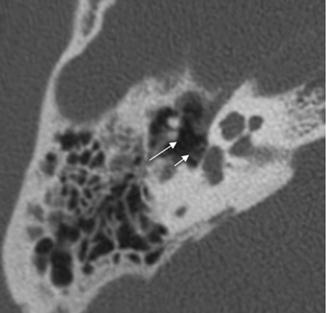
Fig. 3.16
Axial computed tomographic view of a right ear showing a necrosis of the long process secondary to chronic otits media: empty space between the intact stapes (short arrow) and the rest of the incus (long arrow)
3.1.2.2.5 Ligaments of the Incus (Fig. 3.17)
Fig. 3.17
Schematic drawing of incudal ligaments. SIL superior incudal ligament, PIL posterior incudal ligament
The incus has the least number of ligaments and is therefore more susceptible to traumatic dislocation compared to other ossicles. Two ligaments stabilize the incus in place:
The posterior incudal ligament (PIL) secures the short process in the incudal fossa.
The superior incudal ligament (SIL) descends from the tegmen to the incus body. It could be reduced to a single mucosal fold only.
3.1.2.3 The Stapes (Fig. 3.18)
Fig. 3.18
Schematic drawing of stapes in the oval window niche and its relationship with the underlying saccule and utricle. Stapedial tendon in red. (*) annular ligament, P pyramidal eminence, H head, N neck, AC anterior crus, PC posterior crus, FP footplate
The stapes is the smallest bone of the human body; it is 3.25 mm high and 1.4 mm wide with a weight of 3–4 mg [39]. It is situated in an almost horizontal plane between the lenticular process and the oval window and below the facial nerve canal. The stapes consists of a round head, a short neck, anterior and posterior crura, and an oval footplate.
3.1.2.3.1 The Head
The head is the most lateral part of the stapes. It is cylindrical or discoid in shape and bears laterally a glenoid cavity, the fovea, which corresponds to the articular surface of the lenticular process. Its medial end is constricted, forming the neck. Its anterior edge is smooth. Its posterior edge presents a small rough surface for the insertion of the stapedial muscle tendon.
Surgical implication
Partial ossicular replacement requires implants (PORP) which fit onto the head of the stapes alone, thus necessitating the knowledge of the dimensions of the stapedial head. The width of the stapes head is about 1–1.5 mm [39].
3.1.2.3.2 The Crura
The stapes presents two unequal crura: the posterior and the anterior crura; the posterior crus is longer, thicker, and more curved than the anterior one. The relative thickness, the curvature, and the excavation of the crura vary among individuals. The area delimited by the concave arches of the crura is the obturator foramen, sometimes bridged by a veil of mucous membrane. The two crura could be very close to the walls of the niche of the oval window.
Surgical implication
During stapedectomy, it is safer to cut the posterior crus of the stapes rather than to fracture it because the later carries a risk of footplate luxation. This is not the case of the anterior crus which is thinner and can be safely fractured.
3.1.2.3.3 The Footplate
The footplate is a thin and oval lamella of bone. Its length is about 3 mm; its width is about 1.5 mm; its thickness is about 0.25 mm [40].
The lateral or tympanic surface of the footplate is covered by mucoperiosteum of the middle ear; it is slightly twisted around its polar axis so that the anterior half looks to the floor of the vestibule and the posterior part looks up to the tegmen. The distance from the long process of the incus to the tympanic surface of the footplate is about 4 mm.
The medial or vestibular surface of the footplate is flat; it is lined by the endosteum of the otic capsule and is in close relation with the saccule and utricle. The saccule is 1 mm deep from the anterior part of the vestibular surface of the footplate, and the utricle is at 1.5 mm deep from its posterior part (Fig. 3.18).
Surgical implication
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


