, Jacques Magnan3, Hassan Haidar4, Karen Nicolas5, 6 and Stéphane Louryan7
(1)
Hospital Sacre Coeur ORL Chirurgie Cervico – Faciale, Lebanese University, Baabda, Lebanon
(2)
ORL Chirurgie Cervico – Faciale, Hôpital Trad, Beirut, Lebanon
(3)
ORL – Chirurgie Cervico – Faciale, University Aix-Marseille Hôpital Nord, Marseille, France
(4)
ORL – Chirurgie Cervico – Faciale, Hôpital Nord, Marseille, France
(5)
Department of Radiology Middle East Institute of Health, Bsalim Levant Clinics, Fachaerztin fuer Radiologische Diagnostik Lebanese University, Beirut, Lebanon
(6)
Department of Radiology, Levant Clinics, Sinn el Fil, Lebanon
(7)
Laboratoire d` Anatomie Biomécanique et Organogenèse, Université Libre de Bruxelles Faculté de Médecine, Brussels, Belgium
2.1 Lateral Wall
2.1.2 Lateral Wall Anatomy
2.3 Posterior Wall
2.3.2 Posterior Wall Anatomy
2.4.2 Superior Wall Anatomy
2.5.2 Anterior Wall Anatomy
2.6.2 Medial Wall Anatomy
Abstract
The middle ear cavity is an irregular air-filled space hollowed out in the center of the temporal bone between the external auditory meatus laterally and the inner ear medially. It lies at the intersection between two important axes: one latero-medial between the external and the internal auditory canals, the other one posteroanterior between the mastoid antrum and the Eustachian tube.
For descriptive purposes, the tympanic cavity may be considered as a box with four walls, a roof, and a floor. Because of the convexity of the medial and lateral walls, the middle ear cavity is constricted at its center. The width of the middle ear cavity is 2 mm at the center, 6 mm superiorly in the attic, and 4 mm inferiorly in the hypotympanum. In the sagittal plane, the middle ear cleft measures about 15 mm both in the vertical and horizontal directions.
The middle ear cavity is an irregular air-filled space hollowed out in the center of the temporal bone between the external auditory meatus laterally and the inner ear medially (Fig. 2.1). It lies at the intersection between two important axes: one latero-medial between the external and the internal auditory canals, the other one posteroanterior between the mastoid antrum and the Eustachian tube (see Fig. 1.8).
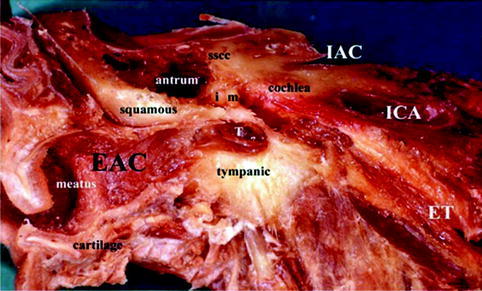
Fig. 2.1
Oblique cut of a right temporal bone. The middle ear cavity lies in the center of the temporal bone between the outer ear (EAC) and the inner ear. T the tympanic membrane, i incus; m malleus, sscc superior semicircular canal, ET Eustachian tube, IAC internal auditory canal, ICA internal carotid artery
For descriptive purposes, the tympanic cavity may be considered as a box with four walls, a roof, and a floor. Because of the convexity of the medial and lateral walls, the middle ear cavity is constricted at its center. The width of the middle ear cavity is 2 mm at the center, 6 mm superiorly in the attic, and 4 mm inferiorly in the hypotympanum. In the sagittal plane, the middle ear cleft measures about 15 mm both in the vertical and horizontal directions (Fig. 2.2).
Fig. 2.2
Schematic drawing of the middle ear cavity showing its different dimensions. VII facial nerve, CP cochleariform process
The middle ear cavity is surrounded by six walls: the lateral wall, the inferior wall called the floor or the jugular wall, the posterior called the mastoid wall, the superior wall also called the roof or the tegmen, the anterior wall called the carotid wall, and the medial wall called the cochlear wall.
2.1 Lateral Wall
The lateral wall is formed by the tympanic membrane, the bony tympanic ring and the attic outer wall (Fig. 2.2). This wall of the middle ear cavity, especially the tympanic membrane, is the only wall accessible to clinical examination and is the site of most middle ear pathologies. In addition, the lateral wall represents the classic entry site to the middle ear during ear surgery.
2.1.1 Embryology of the Lateral Wall
The development of the tympanic bone and membrane starts as early as the fourth week of intrauterine life [1]. A funnel-shaped ectoblastic pouch grows inwards from the first branchial cleft until it reaches an endoblastic pouch growing laterally from the first branchial pouch, known as the tubotympanic recess. The contact between the ectoblastic and the endoblastic pouches is short-living.
By the fifth week of the fetal life and due to the growth of the cephalic extremity with its flexion-extension positions, the region of the future neck creates two types of forces: an expansive force and a depressive force. Under the expansive cephalic flexion, the mesenchyme interposes between the ectoblastic and the endoblastic pouches. At the seventh week this mesenchyme contributes to the formation of the fibrous stratum of the tympanic membrane and the handle of malleus (Fig. 2.3).
Fig. 2.3
Tympanic membrane formation. The tympanic membrane is formed from the three germ layers, ectoderm (1), mesoderm (2), and endoderm (3)
At the eighth week, the epithelial cells at the bottom of the ectoblastic pouch proliferate and form a compact epithelial plate reaching the endoblast. Later, this ectoblastic plate gives rise to the bony external auditory canal and the tympanic membrane at its end. When the tympanic membrane appears, it consists already of three layers and has an elliptical form with a horizontal diameter of approximately 2 mm.
At birth the tympanic membrane is in almost horizontal plane. As the tympanic ring changes its orientation, the caudal tympanic sulcus is pushed laterally and the tympanic membrane becomes more vertical (see Sect. 1.3). This explains the difficulty of exposure of the tympanic membrane in newborns during otoscopic examination or paracentesis.
Clinical Pearl
Congenital Cholesteatoma
Congenital cholesteatoma are residual squamous inclusion cysts that arise from epithelial rests in the middle ear. These epithelial rests are normally seen during fetal development and usually disappear by the third trimester. The failed involution of these epithelial rests leads to a congenital cholesteatoma [2, 3].
2.1.2 Lateral Wall Anatomy
The lateral wall of the tympanic cavity is partly bony and partly membranous. The central portion of the lateral wall is formed by the tympanic membrane and the incomplete tympanic ring to which the membrane is attached. Above the tympanic membrane there is a bony wall forming the attic outer wall.
2.1.2.1 The Attic Outer Wall
The attic outer wall, part of the squamous bone, is the bony lateral wall of the attic. It is a wedge-shaped plate of bone that separates the attic from the zygomatic mastoid cells laterally (Fig. 2.4).
Fig. 2.4
(a) Coronal reconstruction of a computed tomography of a right ear, showing the scutum as a sharp bony spur (white arrow) and the attic outer wall (white arrowhead) that separates the attic (*) from the zygomatic cells (ZC). (b) Coronal computed tomography reconstruction of a right ear: erosion of the scutum (long arrow), due to a retraction pocket in the Prussak’s space with keratin debris (short arrow). Thickened tympanic membrane (arrowhead); M malleus, EAC external auditory canal
The part of the attic outer wall lying below the plane tracing the roof of the external auditory canal is called the scutum (means shield in Latin).
The scutum is a thin sharp bony spur formed by the junction of the attic outer wall and the superior wall of the external auditory canal. The scutum forms part of the superior deep portion of the external meatus and gives attachment to the pars flaccida of the tympanic membrane, which is the lateral wall of the Prussak’s space (Fig. 2.4).
Clinical Impact
The scutum is the first bony structure to be eroded by an attical cholesteatoma secondary to a retraction pocket of the pars flaccida into the attic (Fig. 2.4b).
2.1.2.2 The Tympanic Ring
The tympanic ring is the most medial portion of the tympanic bone; it is C shaped and represents the frame in which inserts most of the tympanic membrane periphery. In the inner aspect of the tympanic ring, there is a gutter, the tympanic sulcus, which houses the annulus of the tympanic membrane.
The tympanic ring is deficient superiorly to form the notch of Rivinus. The pars flaccida inserts directly on this notch, and due to the absence of sulcus and the tympanic ring, the pars flaccida is lax rendering it more predisposed to a retraction (Fig. 2.5).
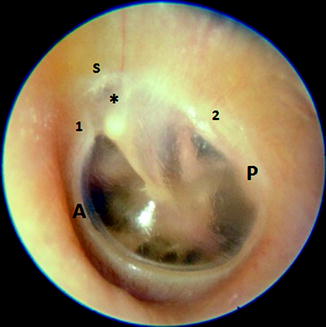
Fig. 2.5
Left tympanic membrane showing the notch of Rivinus (*) limited by the anterior (1) and posterior (2) tympanic spines. Notice the direct insertion of the tympanic membrane on the scutum (s) and the absence of annulus in this zone. Also notice the difference in size between the anterior part of the annulus (A) and the posterior part (P) of the annulus
2.1.2.2.1 The Tympanic Spines
At the junction of the tympanic ring and the attic outer wall, we can identify two spines – the anterior and the posterior tympanic spines (Fig. 2.5):
1.
Anterior tympanic spine: is present at the anterosuperior end of the tympanic ring and represents the anterior limit of the notch of Rivinus
2.
Posterior tympanic spine: is present at the posterosuperior end of the tympanic ring and represents the posterior limit of the notch of Rivinus
2.1.2.2.2 Tympanic Canaliculi
The medial surface of the tympanic ring near the tympanic spines presents three openings (Fig. 2.6):
Fig. 2.6
Schematic drawing of the medial surface of a right tympanic membrane showing Glaserian fissure containing the anterior malleal ligament (AML), the more medial canal of Huguier giving exit for the chorda tympani to the infratemporal fossa. The chorda tympani enters the middle ear through the iter chordæ posterius
The Petrotympanic Fissure (Glaserian Fissure)
The petrotympanic (Glaserian) fissure opens anteriorly just above the attachment of the tympanic membrane. It is a slit about 2 mm long, which receives the anterior malleal ligament and transmits the anterior tympanic artery, a branch of the internal maxillary artery to the tympanic cavity (see Fig. 1.11).
The Iter Chordæ Anterius (Canal of Huguier)
The canal of Huguier is a separate canaliculus placed in the medial end of the petrotympanic fissure; through it the chorda tympani nerve leaves the tympanic cavity towards the infratemporal fossa.
The Iter Chordæ Posterius
The iter chordæ posterius is situated medial to the posterior tympanic spine. It leads into a minute canal through which the chorda tympani nerve exits to enter the tympanic cavity. It lies immediately medial to the tympanic membrane at the level of the upper limit of the malleus handle.
2.1.2.2.3 The Tympanic Sulcus
The tympanic sulcus houses the annulus of the tympanic membrane. The lateral edge of the tympanic sulcus is higher than the medial edge.
The average depth of the sulcus is about 1 mm. However, this depth is not constant; it is maximal at 6 o’clock and decreases gradually as it goes up towards the tympanic spines where it disappears completely. The posterosuperior part of the sulcus is shallow and its depth is around 4 mm.
Clinical Implications
These changes in the depth of the sulcus reflect the stability of the insertion of the annulus; in the posterosuperior quadrant the annulus is not totally inserted into the sulcus and is merely supported (Fig. 2.7). This weak insertion of the posterosuperior quadrant of tympanic membrane to the tympanic ring makes it lax and predisposed to retraction [4].
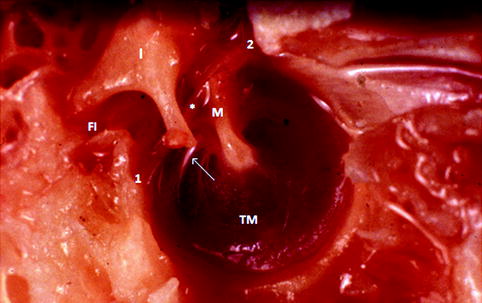
Fig. 2.7
A medial view of the lateral wall of a left middle ear showing the incomplete insertion of the posterosuperior part of the annulus (white arrow) in the tympanic sulcus. 1 iter chordæ posterius, 2 iter chordæ anterius, FI fossa incudis, TM tympanic membrane, M malleus, I incus, * chorda tympani
2.1.2.3 The Tympanic Membrane
The tympanic membrane (TM) separates the external auditory meatus from the middle ear. It is a thin semitransparent membrane that is nearly circular in form and is approximately 8 mm wide, 9–10 mm high, and 0.1 mm thick.
The inferior part of the membrane lies more medially than the superior part; the TM forms an inclination of about 40° relative to the inferior wall of the auditory meatus (Figs. 2.1 and 2.8).
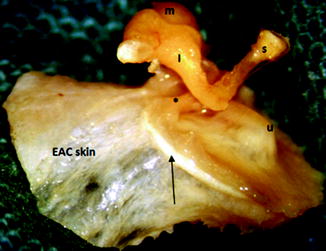
Fig. 2.8
Left ear tympanic membrane allograft showing the annulus (black arrow) and the posterior tympano-malleal fold (*). I incus, m malleus, u umbo, s stapes
The handle of the malleus is firmly attached to the central part of the inner surface of the TM and draws it centrally; this zone of the TM is called the umbo (Fig. 2.10).
Shrapnell divided the TM into two parts, an upper small part called pars flaccida and a lower bigger part called the pars tensa.
The pars tensa, the largest part of the TM, is taut, thickened peripherally into the annulus which is inserted into the tympanic sulcus.
The pars flaccida, Shrapnell’s membrane, is lax, occupies the notch of Rivinus, and is attached to the scutum [5].
2.1.2.3.1 The Tympanic Annulus
The tympanic annulus, or Gerlach’s ligament is a horseshoe-like fibrocartilaginous structure that maintains the insertion of the tympanic membrane in the tympanic sulcus (Fig. 2.8). The annulus is absent superiorly at the level of the notch of Rivinus.
In cross section, the annulus shows a triangular form with a summit pointing towards the pars tensa and a base inserted on the tympanic sulcus [6].
At the level of the tympanic spines, the tympanic annulus prolongs centrally towards the lateral process of the malleus constituting two strands: the anterior and the posterior tympano-malleal strands. These two strands divide the tympanic membrane into the pars flaccida superiorly and the pars tensa inferiorly. Medially, these two strands rise up two slight ridges of mucous membrane on the inner side of the tympanic membrane called the anterior and posterior tympano-malleolar folds (Fig. 2.8).
The diameter of the annulus is not uniform. The maximal mean caliber of the annulus is at 6 o’clock level; from this point, the annulus gradually thins out in both directions until it reaches about 15 % of its maximal caliber at the anterior and posterior tympanic spines [4, 7] (Fig. 2.5).
Surgical Application
During middle ear surgery, the annulus allows an operative dislocation of the tympanic membrane out of the sulcus without tearing it. The most difficult part of the annulus to dislodge is the anterior part because of its firm attachment to the sulcus.
2.1.2.3.2 Microscopic Structure of the Tympanic Membrane
The pars tensa and pars flaccida differ in structure despite the fact that both parts are made of three layers: a lateral epidermal layer, a medial mucosal layer, and a middle layer or lamina propria.
The epidermal layer
The epidermis of the TM and of the bony part of the external ear canal is a specialized type of skin; it does not contain any glands or hair follicles, and it has a potential of lateral migration not encountered in any epidermis elsewhere. Epithelial cells migrate centrifugally outwards from the center of the drum desquamating only when they reach the cartilaginous portion of the ear canal. This process accounts for the self-cleaning ability of the ear canal [8].
The Mucosal layer
The mucosal layer of the eardrum is a continuation of the mucosal lining of the middle ear cavity. It is a very thin monocellular layer of cells.
Lamina propria
This intermediate layer consists of fibrous tissue: The amount and the organization of this tissue is the main difference between the pars tensa and the pars flaccida of the TM.
The pars tensa
The fibrous layer of the pars tensa is attached to the malleus handle and to the tympanic bone and consists of two layers of densely packed collagenous fibers; one is oriented radially and another one oriented circularly [9, 10].
Radial fibrous layers (stratum radiatum) are attached to the manubrium and radiate outward to the annulus.
Circular fibrous layer (stratum circulare) is medial to the radial layer and has its fibers arranged concentrically and insert on the manubrium.
The pars flaccida
The lamina propria of the pars flaccida is composed of small amount of elastic and collagenous fibers with no special arrangement and gradually passes into the dermis of the meatal skin [11].
2.1.2.3.3 Blood Supply of the Tympanic Membrane
Inner surface of the tympanic membrane
The TM is supplied by a vascular circle formed by the anterior tympanic artery branch from the internal maxillary artery and from the stylomastoid branch of the posterior auricular artery (Fig. 2.9).
Fig. 2.9
Medial view of a left tympanic membrane showing tympanic membrane vascularization
Outer surface of the tympanic membrane
The tympanic membrane is supplied by the arteria manubrii having origin from the deep auricular branch of the internal maxillary artery.
2.1.2.3.4 Nerves of the Tympanic Membrane
The membrane receives its innervations from the auriculotemporal branch of the mandibular nerve (CN V3), the tympanic branch of the glossopharyngeal nerve (CN IX), and the auricular branch of the vagus (CN X).
Clinical Application
Tympanic Membrane Retraction Pockets
Pars flaccida retraction pockets
The pars flaccida is the most common area of TM retraction pockets because it is the weakest part of the TM. Two reasons stand behind this weakness:
1.
Sparse amount of unorganized fibres in its lamina propria
2.
Direct insertion of the skin of the pars flaccida on the scutum in the absence of the combination annulus-sulcus, which acts like a ligament stabilizing the insertion of the TM to the surrounding bone [12]
Pars tensa retraction pockets
Pars tensa retraction pockets are more common in its posterosuperior part. Three reasons stand behind this fact:
1.
This part of the TM is more vascularized and thus more vulnerable to inflammation, which leads to secretion of collagenase and destruction of collagen fibers. This renders this part of the TM atrophic and prone to retraction in case of middle ear negative pressure.
2.
The middle fibrous layer of the posterosuperior part lacks a well-developed circular fibrous layer.
In contrary, the anterosuperior quadrant of the TM is less prone to retraction because of its strong insertion into the sulcus, the better arrangement of its circular fibers and the presence of the anterior malleal ligament acting as a support [4].
2.2 Inferior Wall (Jugular Wall)
2.2.1 Embryology of the Inferior Wall
The inferior wall of the middle ear develops between the 21st and the 31st gestational week, from the fusion of the tympanic bone and the petrosal bone. The fusion of these two bones, at 24th gestational week, closes the hypotympanum incompletely and leaves a persistent hypotympanic fissure, which houses the inferior tympanic canaliculus. The inferior tympanic canaliculus transmits the Jacobson’s branch of the glossopharyngeal nerve and the inferior tympanic artery to the middle ear [13] (see Fig. 1.2) (see Sect. 1.1.1).
2.2.1.1 Development of the Jugular Bulb After Birth
The jugular bulb, absent at birth, is a dynamic structure which develops after the age of 2 years and reaches its definite size in adulthood. Children younger than 2 years old do not demonstrate the bulbous enlargement typical of the jugular bulb. The upward forces and the hemodynamic changes that accompany prone position lead to the bulbous enlargement typical of the adult jugular bulb. An erect posture, as opposed to the “fetal” or lying-down positions maintained in utero and in neonates, results in an ascending negative pulse wave originating from the heart and traversing upward to strike the jugular sinus at the jugular foramen. This phenomenon is responsible of the expansion of the jugular bulb [14].
Because the left brachiocephalic vein is relatively longer than the right one, it may dissipate the energy of the venous pulsation generated from the heart and consequently explain the development of a larger jugular bulb on the right side.
The absence of the jugular bulb at birth and its development in early infancy suggest that jugular bulb abnormalities are acquired rather than congenital and thus may progress with time to expand into the adjacent structures.
The venous blood flow dynamics may ultimately determine the variations in final size and position of the jugular bulb [14].
2.2.2 The Inferior Wall Anatomy
The floor of the middle ear cavity is narrow and consists of a thin plate of bone that separates the middle ear from the jugular bulb posteriorly and the internal carotid artery anteriorly. Between the carotid artery and the jugular bulb near the medial wall, there is a small canal, the inferior tympanic canaliculus, which transmits the Jacobson’s nerve, branch of the glossopharyngeal nerve (CN IX), and the inferior tympanic artery (Fig. 2.10).
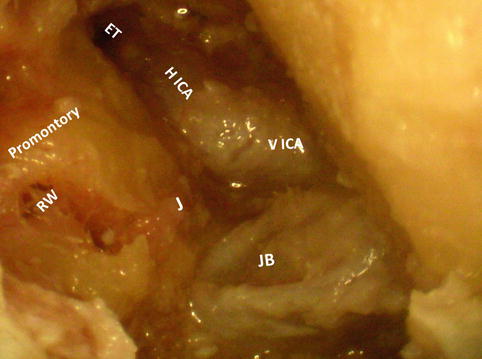
Fig. 2.10
Right ear after transcanal hypotympanotomy and dissection of the vertical portion of internal carotid artery (VICA) and the jugular bulb (JB), notice the emergence of the Jacobson’s nerve (J) between the VICA and the JB and its relation to the round window (RW); also notice the relation of the horizontal portion of the internal carotid artery (HICA) and the Eustachian tube (ET); the HICA lies in the medial wall of the Eustachian tube
The surface of this wall may show irregularities due to the overlying pneumatized cells. In the posterior part of the floor is the root of the styloid process which gives rise to a bony eminence, the styloid eminence.
2.2.2.1 The Jugular Bulb
The jugular bulb connects the sigmoid sinus to the internal jugular vein.
It lies in the jugular fossa, an oval hollowed area at the internal and inferior surface of the petrous pyramid. The jugular bulb inhabits the posterior and largest compartment of the jugular foramen. The IX, X, and XI cranial nerves pass the skull base with this venous system.
The jugular bulb communicates with the cavernous sinus through the inferior petrosal sinus.
The jugular bulb dome lies at the floor of the middle ear cavity below the labyrinth and medial to the mastoid segment of the facial nerve.
It is variably positioned in relation to the hypotympanum, and its distance from the facial nerve laterally and the labyrinth superiorly is variable (Fig. 2.11). The distance from the jugular bulb to the posterior semicircular canal superiorly ranges from 0 to 10 mm (mean, 4 mm). The distance from the jugular bulb to the facial nerve laterally ranges from 0 to 12 mm (mean, 7 mm) [15].
Fig. 2.11
Coronal computed tomographic reconstruction on the mastoid segment of the facial nerve (arrowheads) on both ears and the relation to the jugular bulb (JB) and the posterior semicircular canal (PSCC) (black arrow): (a) On the right side (R), small jugular bulb (JB) with a large distance (red arrow) to the PSCC. (b) On the left side (L), huge JB with a short distance (red arrow) to the PSCC
Surgical Application
Retrofacial Approach to the Middle Ear
Retrofacial approach to the middle ear is done by drilling the area between the facial nerve laterally, the jugular bulb inferiorly and medially, and the ampulla of the posterior semicircular canal superiorly. This approach can provide a good access to the hypotympanum and the related structures without transposing the facial nerve or taking down the posterior external auditory canal wall. In cases with a high and lateral jugular bulb, this approach could not be done easily [15] (Fig. 2.12).
Fig. 2.12
(a) Retrofacial approach in a left ear hypotympanum. (*) surgical instrument; VII mastoid segment of the facial nerve, JB jugular bulb, TM tympanic membrane, M malleus, I incus, S stapes, LSCC lateral semicircular canal, PSCC posterior semicircular canal. (b) Sagittal oblique reconstruction of a computed tomography showing the retrofacial hypotympanotomy approach (red arrow). Mastoid segment of the VII nerve (arrowheads), hypotympanic air cells (black arrows), round window membrane (between the white arrows), basal turn of the cochlea (empty arrow). A antrum, JB jugular bulb
Clinical Application
Jugular Bulb Anomalies
A high jugular bulb (HJB) is a condition in which the jugular bulb dome rides above the tympanic annulus. A HJB has an intact sigmoid plate which separates it from the middle ear cavity. If the sigmoid plate is deficient, the bulb protrudes into the middle ear cavity; this situation is called a dehiscent jugular bulb (JBD) (Fig. 2.13).
Fig. 2.13
(a) Coronal computed tomographic view on a right ear with a normal jugular bulb (JB), round window recess (black arrow). (b) High riding JB obliterating the round window recess (black arrow). (c) JB diverticula (small white arrow), reaching the round window recess (black arrow). Notice the transtympanic tube in place (long white arrow)
A HJB or JBD manifests as a pulsatile tinnitus and appears like a posteroinferior retrotympanic blue mass on otoscopic examination. Injury of a JBD during tympanomeatal flap elevation results in profuse bleeding [16, 17].
The incidence of high JB ranges from 5 to 20 % and that of JBD ranges from 1 to 10 % [17].
2.3 Posterior Wall
2.3.1 Embryology of the Posterior Wall
The posterior wall develops from the Reichert’s cartilage. The facial nerve develops in a groove on the otic capsule. By the 20th week, the facial canal is better defined by fibrous tissue laterally as the otic capsule ossifies medially. Reichert’s cartilage persists as a cartilage bar interposed between the otic capsule and the facial nerve medially and the tympanic annulus laterally [18]. Ossification starts in this cartilage bar and continues in the mesenchyme both medial and lateral to this cartilage bar, forming the facial canal and the posterior wall of the middle ear cavity. The cartilage remnant of Reichert’s bar frequently persists to the time of birth, ossifying separately from the surrounding mesenchyme. The first cartilaginous wall of the facial canal is the laterohyale connected primitively with the interhyale, rudiment of the stapedial tendon (Fig. 2.14).
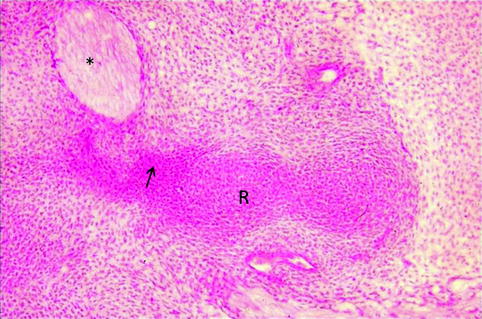
Fig. 2.14
15.5-mm human embryo coronal section showing the laterohyale (arrow) covering facial nerve rudiment (*), in connection with the Reichert’s cartilage (R). Hematoxylin-eosin staining
2.3.2 Posterior Wall Anatomy
The posterior wall is the highest wall of the middle ear and measures about 14 mm. It is formed essentially by the petrous bone. The posterior wall separates the middle ear from the mastoid air cells, except at the area of the aditus ad antrum, where it is deficient and permits communication between the attic and the mastoid antrum.
The posterior wall can be divided into two distinct parts: the upper third which corresponds to the aditus ad antrum and represents the posterior limit of the epitympanum and the lower two thirds which correspond to the posterior wall of the retrotympanum.
The two parts are separated by the incudal buttress which is a compact bone that runs from the tympanic ring laterally to the lateral semicircular canal medially. It houses the incudal fossa in its superior surface which lodges the short process of the incus (Fig. 2.15).
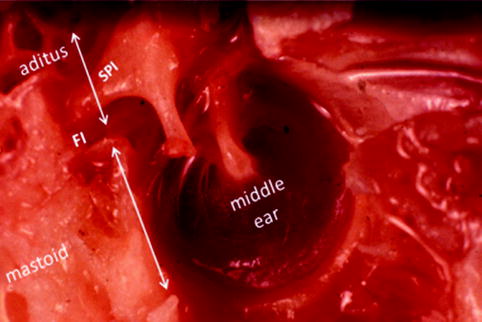
Fig. 2.15




A medial view of a left middle ear showing the posterior wall composed of an inferior closed part separating the middle ear from the mastoid and a superior open part, the aditus ad antrum, which connects the middle ear to the mastoid. Notice that the floor of the aditus houses the fossa incudis (FI), which lodges the short process of the incus (SPI)
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
