CHAPTER 32 Mentoplasty and Facial Implants
Mentoplasty
The chin prominence is not present in any four-legged mammal.1 During evolution, with the adoption of an upright posture and with verticalization of the face; the chin became an important facial feature. The events contributing to the evolutionary development of the chin in humans are open to speculation; however, the importance of the chin in the overall appearance of the face cannot be overstated.
In general, when patients inquire about improving their facial appearance, they rarely ask about surgical correction of the chin. More commonly, requests focus on seemingly more obvious problems, such as reduction of a large nose or correction of sagging skin of the neck and jowls. However, recognition, evaluation, and treatment of chin abnormalities often has a great impact on facial appearance. It is clear that all attractive faces have an underlying balance and structural symmetry to their facial skeletons.2 Proper balance of the facial skeleton requires harmony and proportion of all bones of the face in all three planes of space. The chin should therefore be evaluated as it relates to important adjacent structures, such as the lips, teeth, and nose.3 Appropriate treatment of aesthetic deformities of the chin contributes to facial harmony and often improves the appearance of the mouth, the lips, and the nose. It is for these reasons that every face should be carefully studied to determine why the chin appears unattractive. This enables the surgeon to correct the deformity and improve facial proportion.
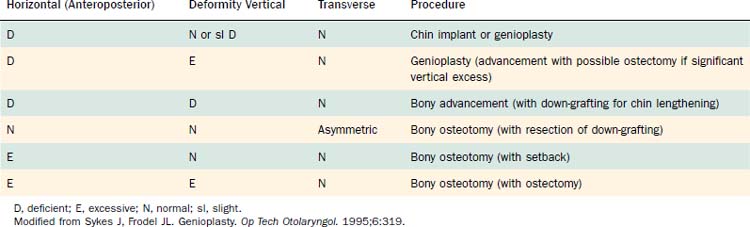
Surgical correction of aesthetic deformities of the chin can be performed by either chin augmentation with an implant or by osteotomy and advancement (or reduction) of the bony mentum. Augmentation using alloplastic implants can camouflage a horizontal (AP) bony deficiency.4 However, this technique is not effective in correcting vertical (superoinferior) or transverse deformities of the lower face and chin. Horizontal bony osteotomy of the chin (osseous genioplasty) is a simple and versatile procedure. This technique allows horizontal advancement or reduction of the chin, vertical lengthening or shortening of the chin, and correction of transverse deformities of the chin. The procedure chosen to correct the specific aesthetic problem is based on the type and extent of the deformity (Table 32-1).3 If carefully evaluated and planned, aesthetic correction of chin deformities can provide significant improvement in the overall balance and proportion of the face.
Patient Evaluation
To precisely correct any chin deformity, careful preoperative analysis of the deformity is essential.3,5 Specifically, the chin should be evaluated as it relates to other skeletal and soft tissue structures, including the lips, teeth, nose, and soft tissues of the neck. A detailed history of past trauma, orthodontic treatment, or prior oral surgery is essential. This is important because many patients with dental malocclusion and underlying facial skeletal abnormalities are treated with orthodontics. This method of dental compensation may correct the malocclusion, but it fails to improve the underlying skeletal deformity. It is therefore important to discuss prior therapy, including orthodontics, with the patient.
Physical examination should include inspection and palpation of the chin, lips, nose, and teeth. The entire face should be observed at rest and during animation to evaluate the mentalis soft tissue mound and its support. With aging, patients may develop ptosis of the soft tissue pad of the chin. In patients with open bite deformities and lip incompetence, hyperactivity of the mentalis muscles (“mentalis strain”) can occur (Fig. 32-1). For this reason, the dental occlusion should be carefully examined to determine whether orthodontics or orthognathic surgery is needed.

Radiographic evaluation of the chin routinely includes a panoramic radiograph (Panorex) and cephalometric radiographs in the AP and lateral views. The panoramic radiograph shows the cortical outline of the mandible and the vertical mandibular height (Fig. 32-2). The Panorex also delineates the position of the tooth roots and of the inferior alveolar canals and mental foramina. It is important to know the exact position of the mental foramen and canal preoperatively so intraoperative damage to the mental nerve can be prevented. The inferior alveolar nerve, a branch of the third division of the fifth (trigeminal) cranial nerve, travels through the mandibular canal and exits the mental foramen as mental nerve. The mental nerve supplies sensation to the skin and mucous membranes of the lower lip and chin. The mandibular canal is often located 2 to 3 mm below the level of the mental foramen.1 Bony osteotomies should therefore be performed at least 5 mm below the mental foramen to avoid injury to the neurovascular bundle.

If bony genioplasty is considered, AP and lateral cephalometric radiographs should be performed (Fig. 32-3). AP views allow detection and evaluation of transverse skeletal asymmetries of the chin. Transverse asymmetries are common in patients with Goldenhar’s syndrome or hemifacial microsomia, but they are also commonly seen in nonsyndromic patients considering aesthetic surgery. When transverse bony or soft tissue asymmetries are overlooked preoperatively in a patient with microgenia, augmentation with an alloplastic chin implant can accentuate the deformity.3

Lateral cephalometric radiographs allow detailed analysis of both the soft tissues and the facial skeleton. The cephalogram should be obtained at a standard distance with the head positioned so that the Frankfort horizontal line is parallel to the floor.6 From this standardized lateral radiograph, a series of soft tissue and skeletal points can be identified. This allows various analyses of the chin as described by Ricketts,7 Steiner,8 Burstone,9 Gonzalez-Ulloa and Stevens,10 and others. Ricketts’ analysis (Fig. 32-4) uses a tangent connecting the soft tissue pogonion (most projecting point) of the chin with the most projecting point of the nasal tip.7 In this system, the upper lip should lie about 4 mm behind the line, whereas the lower lip is ideally located 2 mm behind the line. While the Ricketts analysis correctly evaluates the lower face in profile, it places great importance on the projection of the nasal tip. The Steiner analysis uses the columellar inflection point(s) to identify the correct position for the chin point.8 This method places importance on the lip position. The Holdaway “H” angle (Fig. 32-5) relates the position of the soft tissue pogonion with important skeletal points on the mid and lower face. No single analysis is ideal, but each method attempts to determine the “ideal” positions for the soft tissues and skeleton of the chin because these structures relate to the remainder of the face.
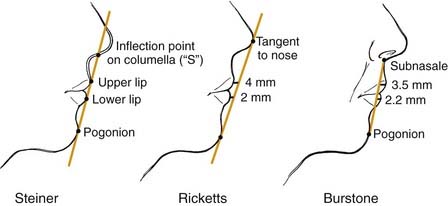

Figure 32-5. The Gonzalez-Ulloa and Stevens and the Holdaway analyses of the chin and lower third of the face.
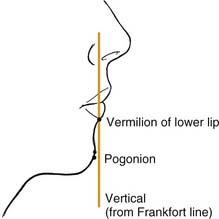
An accurate chin analysis using the lateral cephalogram involves dropping a vertical line from the Frankfort horizontal (porion-infraorbitale) through the soft tissue subnasale.11 With ideal horizontal chin projection, the soft tissue pogonion should lie approximately 4 mm behind this line (Fig. 32-6). The most frequently used evaluation of the chin drops a perpendicular line from the vermilion border of the lower lip and compares the AP position of this line with the soft tissue pogonion (the anterior-most projecting chin point) (Fig. 32-7). A general guideline for aesthetic chin position in this method is for the pogonion in a male patient to be positioned at the level of this vertical line and for the pogonion in a female patient to be just posterior to the line. If the position of the soft tissue pogonion is anterior to the proposed line, horizontal macrogenia is diagnosed, whereas microgenia is present if the chin is positioned posterior to the ideal line. Although this method is effective for AP deformities (microgenia or macrogenia), it does not account for vertical or transverse discrepancies. Because many surgeons primarily use this evaluation method, vertical or transverse chin problems are often overlooked.
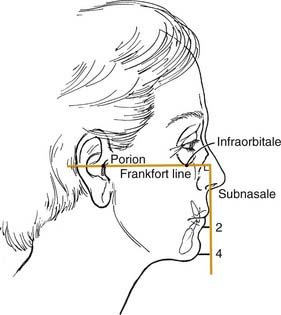
Figure 32-6. Horizontal relationships of the chin and upper and lower lips as they relate to the nasal perpendicular line.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


