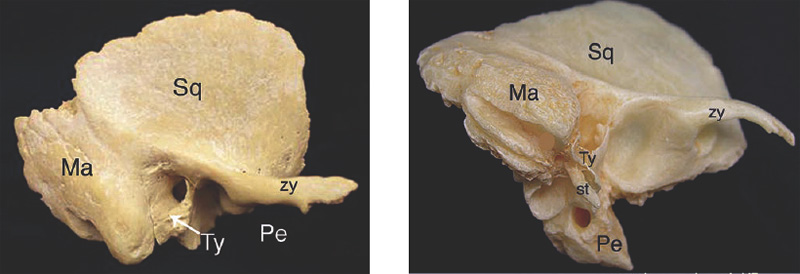
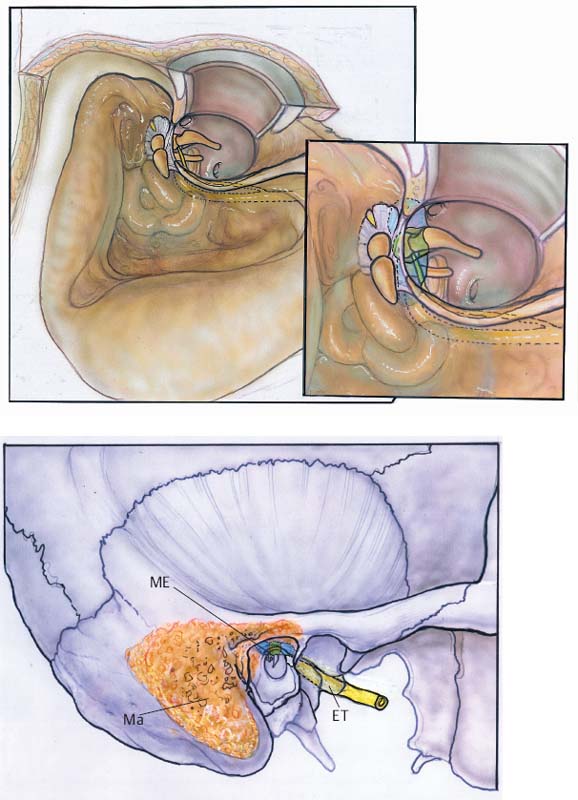
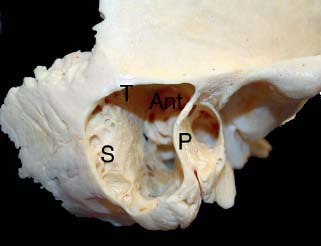
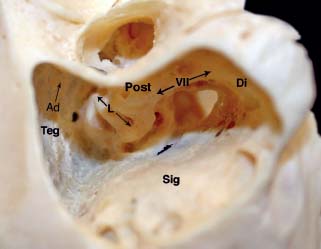
4 Mastoidectomy The temporal bone anatomically consists of four bones: the mastoid, petrous, squamous, and tympanic (Fig. 4.1A,B). The pneumatized portion of the temporal bone consists of a continuous air cell tract that includes the eustachian tube, the middle ear, and the mastoid air cells (Fig. 4.2). From the anatomical point of view, the mastoid contains one large air cell—the antrum—and the periantral cells that communicate with it. Mastoidectomy, therefore, is a surgical procedure that opens the air cells of the mastoid, using a drill to remove the outer cortex and to exteriorize the contents of the temporal bone. The mastoid has a triangular shape. The anatomical limits of the mastoid are the tegmen superiorly, the posterior bony canal anteriorly, and the sigmoid sinus posteriorly. The cellularity of the mastoid varies among individuals and can be well developed (“pneumatized”), diploic (marrow containing), or sclerotic (dense bone). Every mastoid, no matter how poorly developed, has a single large air cell called the antrum (Fig. 4.3). Lateral to the antrum is a thin plate of bone named the Korner septum. Anatomically, the Korner septum, also named the petrosquamosal septum, is an embryonic fusion plane of the squamous and petrous bones. At the base of the antrum is a dome of dense ivory bone (labyrinthine part of the otic capsule) formed by the lateral (or horizontal) semicircular canal (Fig. 4.4). This is the key surgical landmark in the temporal bone. The antrum communicates with the epitympanum (attic) superiorly, through the aditus ad antrum. The fossa incudus is the space just anterior and inferior to the aditus that houses the body of the incus. The mastoid tip is the most dependent group of air cells and is bisected by the digastric ridge, the indentation formed externally by the posterior belly of the digastric muscle forming the digastric groove. The incus points to the mastoid (vertical) segment of the facial nerve. The facial nerve is at the same depth (lateral to medial) as the lateral semicircular canal, and is encased in a layer of dense labyrinthine bone. The mastoid segment of the facial nerve describes a shape like a candy cane, beginning just anterior to the lateral semicircular canal at the second genu and traveling inferiorly toward the mastoid tip where it exits from the stylomastoid foramen. The pneumatized cell tract just lateral to the mastoid segment of the facial nerve is called the facial recess. The facial recess is bounded laterally by the chorda tympani nerve, superiorly by the incus, and medially by the facial nerve. The facial recess can be opened surgically to create a communication between the mastoid and the middle ear. Inferiorly, the facial nerve travels close to the digastric muscle, and its sheath becomes confluent with the periosteum of the digastric, forming a dense fibrous ring at the stylomastoid foramen. Fig. 4.2 The eustachian tube (ET), middle ear (ME), and mastoid air cell system (Ma) make up one continuous air-containing space within the temporal bone. Fig. 4.3 Mastoidectomy, right temporal bone. The limits of the dissection are the tegmen (T) above, the posterior canal wall (P) anteriorly, and the sigmoid sinus (S) posteriorly. The largest air cell at the base of the mastoid cavity is the antrum (Ant). The “solid angle” of bone in the center of the mastoid is formed by the three semicircular canals (Fig. 4.5). The lateral semicircular canal lies 30 degrees to the horizontal plane. The superior semicircular canal lies in an oblique plane and superiorly indents the tegmen to form the arcuate eminence. The posterior semicircular canal lies at right angles to the lateral semicircular canal. Medially the posterior and superior canals join to form a common crus (“crus commun”). The sigmoid sinus forms the posterior limit of the mastoid (although in a well developed mastoid a group of retrosigmoid air cells is often present). The sigmoid is so named because it describes an S-shaped course. Superiorly the sigmoid meets the tegmen mastoideum and becomes the transverse sinus. The air cells between the tegmen and the sigmoid form the sinodural angle (Fig. 4.5). At the depth of the sinodural angle (at the junction of the middle fossa and posterior fossa dura) is the superior petrosal sinus, which travels anteriorly to communicate with the cavernous sinus. Inferiorly, the sigmoid sinus turns in an anterior direction to enter the jugular bulb. The jugular bulb resides in the hypotympanum, but its location is variable, sometimes higher or lower, sometimes more anterior or posterior. The jugular bulb can be approached surgically through the retrofacial air cell tract, medial to the mastoid segment of the facial nerve. At the depth of the mastoid, anterior to the sigmoid sinus, is the posterior fossa dura. The endolymphatic sac resides within the posterior fossa plate as a double fold of dura (Fig. 4.6). The sac is sandwiched between the posterior fossa plate and an incomplete layer of bone called the operculum. Superiorly, the sac forms the endolymphatic duct, which travels through a bony channel, the vestibular aqueduct, to enter the labyrinth just medial to the posterior semicircular canal. Cholesteatoma is a disease process that invades the pneumatized spaces of the temporal bone. The goals of cholesteatoma surgery are to eradicate the disease, try to restore hearing, and prevent recurrence by creating a safe, dry ear. Mastoidectomy is needed in the majority of cases to expose the disease in the temporal bone, with the exception of those that are confined to the middle ear alone. The pattern of growth of cholesteatoma is determined by the mucosal folds described by von Troeltsch (see Chapter 1, Fig. 1.9).1 Cholesteatomas arise from retractions of the pars flaccida in the attic or the pars tensa in the middle ear and extend upward and backward to involve the mastoid.2 Early cholesteatomas may remain confined to the Prussak space; later on they will envelop the incus and malleus head and grow into the posterior and anterior epitympanic spaces. From there, they will extend through the aditus to fill the antrum, and eventually, all the mastoid air cells. The procedure needed to remove a cholesteatoma is determined by the extent of the disease and the size of the mastoid. Therefore, a preoperative computed tomographic (CT) scan is often helpful to plan the operation. In cases confined to the middle ear, a tympanomeatal flap alone may provide sufficient exposure. In cases involving only the Prussak space, a limited atticotomy can be suitable. When the disease extends to the mastoid but spares the middle ear, and the disease is lateral to the head of the malleus and body of the incus, a Bondy operation might be ideal, especially if the mastoid is sclerotic. Most cholesteatomas, however, will require a mastoidectomy, and the decision to leave the canal wall up or take the canal wall down will be determined by the disease, the anatomy, the presence of complications, and the reliability of the patient, as discussed further below. Cholesterol granuloma is a common condition that accompanies advanced cases of cholesteatoma and sometimes occurs by itself.3 The mastoid air cells are filled with inflammatory tissue with a yellow color and a fatty consistency, and there is brown fluid with the viscosity of motor oil (Fig. 4.7). The middle ear may have a bloody effusion, dark blue in color, which is referred to as idiopathic hemotympanum. Histologically, there is inflammatory granulation tissue with hemosiderin, cholesterol crystals, and areas of hemorrhage. Pathologically, the condition is believed to be caused by blockage of pneumatized cells, leading to hemorrhage and later degradation of blood products. The condition is irreversible and is treated by surgical exenteration of the involved cells with reconstitution of aeration of the middle ear, epitympanum, and mastoid. A myringotomy tube alone is rarely successful in treating the condition because the tube readily becomes blocked by the thick effusion, but a tube can be a useful adjunct at the time of mastoidectomy to provide aeration and prevent recurrence of the disease. The terminology for mastoid surgery is not uniform. Several terms have developed to describe the different forms of mastoidectomy, summarized in Table 4.1. Tympanomastoidectomy is the general term that appears in coding manuals, but it conveys no specific information about what was done to either the middle ear or the mastoid. For the sake of clarity, it is best to describe separately the type of mastoidectomy, tympanoplasty, and ossicular reconstruction. For example, the mastoidectomy can be classified as canal wall up or canal wall down; the tympanoplasty can be classified as using a cartilage or a fascial graft; and the ossicular reconstruction can be described explicitly (eg, type III, incus interposition, etc, as covered in Chapter 3). In general, mastoidectomy can be performed in one of two ways, canal wall up or canal wall down (Table 4.1). The Bondy operation is a type of canal wall down procedure that is done in a retrograde or inside-out fashion, and which attempts to avoid the middle ear. Atticotomy is performed when disease is confined to the epitympanum and can be done through the mastoidectomy or through the ear canal. The canal wall up mastoidectomy preserves the posterior bony canal wall and thereby results in normal ear canal anatomy, heals more rapidly, avoids the need for water precautions, and readily permits the use of a hearing aid. The virtue of this technique is that it avoids the problems of prolonged healing and postoperative maintenance of the mastoid bowl, but the closed cavity that results is a potential space for residual cholesteatoma to hide and for recurrent cholesteatoma to re-form. The canal wall down mastoidectomy exteriorizes the mastoid space, so that residual disease can be detected early and recurrence should (theoretically) not occur, but it carries the penalty of creating a cavity that may require periodic cleaning and water avoidance and that has the potential for drainage.
♦ Anatomy of the Mastoid
♦ Conditions of the Mastoid
Cholesteatoma of the Mastoid
Cholesterol Granuloma
♦ Surgery of the Mastoid
Classification
Canal Wall Up versus Canal Wall Down
Canal Wall Up (Intact Canal Wall) | Canal Wall Down |
Combined approach Closed technique Simple mastoidectomy | Atticoantrotomy, or Bondy operation Open technique Modified radical (or radical) mastoidectomy |
Canal Wall Up (Intact Canal Wall) Mastoidectomy
The canal wall up mastoidectomy is favored when the mastoid is very well developed, because taking the canal wall down might result in a large, troublesome cavity. When combined with a transmastoid atticotomy and facial recess opening, the canal wall up approach provides access to all areas of the mastoid and middle ear. In cases where there is no clear preference in advance for canal wall up or canal wall down, the canal wall up procedure can be performed as the initial approach and can be converted to canal wall down if the exposure proves to be limited.4 At the time of surgery, the surgeon can accurately determine the extent of the disease and the need to take the canal wall down for more complete surgical access.
The method of canal wall up mastoidectomy is as follows. The meatus should be inspected first using a microscope and speculum. The ear canal and postauricular skin are injected with 1% lidocaine with epinephrine through a small-gauge needle to provide hemostasis and hydroplane dissection. The opening of the cholesteatoma sac in the pars flaccida or pars tensa can be inspected and bluntly probed to confirm the diagnosis and to see where the disease tracks. Tympanomeatal incisions can be created at this time, or can be performed later through the postauricular incision. A limited tympanomeatal flap can be elevated to determine the involvement of the middle ear by disease. The integrity of the incus and stapes can also be determined at this point, and the incudostapedial joint can be separated before drilling the attic (to prevent vibrational trauma to the cochlea intact ossicular chain).
A postauricular incision is made and carried down to the avascular plane lateral to the temporalis fascia, and then is continued inferiorly at the same depth, creating a flap lateral to the mastoid periosteum and sternocleidomastoid muscle (this incision transects the postauricular muscles and skeletonizes the conchal bowl from behind). Once the posterior canal skin is reached, an incision is made in the mastoid periosteum along the linea temporalis (the inferior border of the temporalis muscle) and a counterincision is made down toward the mastoid tip. The periosteum is then elevated in all directions, exposing the mastoid cortex and bony ear canal. The canal skin is then bluntly elevated from the tympanic bone. Tympanomeatal incisions can be performed through the meatus with straight and angled blades, or alternately, a U-shaped incision can be made from posteriorly, perforating the skin at a midcanal level and bringing the cuts out to 6 and 12 o’clock to fashion a conchomeatal flap (ie, a laterally based flap pedicled on the conchal skin). (Some surgeons prefer to create a “vascular strip” incision, making vertical cuts at the tympanomastoid and tympanosquamous suture lines, and a horizontal cut adjoining the two through the canal skin overlying the tympanic ring).
Once the mastoid cortex is exposed, the external landmarks are confirmed. The linea temporalis (temporal line) corresponds to the tegmen mastoideum. The cribriform area of bone just behind the tympanomeatal spine (spine of Henle) called the MacEwen triangle demarcates the position of the mastoid antrum (Fig. 4.8).
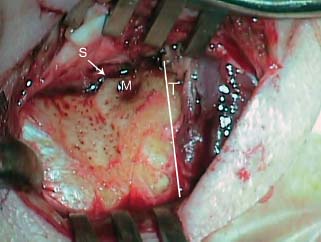
Fig. 4.8 After gaining soft tissue exposure, the external landmarks for mastoidectomy can be identified. These are the suprameatal (or Henle) spine (S), MacEwen triangle (M), and the temporal line (T, line) which is formed by the inferior border of the temporalis muscle.
A cutting drill is used with constant suction and irrigation to create cuts in the cortical bone just inferior to the temporal line and parallel to the posterior bony meatus, with the deepest point at the MacEwen triangle (Fig. 4.9). A triangle of bone is removed and progressively enlarged and deepened, removing the mastoid air cells until the Korner septum is reached (Fig. 4.10). The internal landmarks of the mastoidectomy are the tegmen superiorly, the posterior canal wall anteriorly, and the sigmoid sinus posteriorly—these structures should be skeletonized but not violated. The Korner septum is then opened with either burr or curette to enter the mastoid antrum.
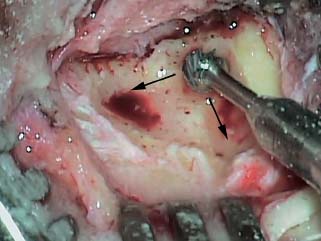
The cholesteatoma usually fills the mastoid antrum and, if the disease is extensive, it can involve the remaining pneumatized spaces of the mastoid down to the tip. Unless it is small, the cholesteatoma sac must be incised and its contents (debris) delivered before the deeper structures can be identified (Fig. 4.11A). The lateral semicircular canal resides at the base of the antrum; it is a dome-shaped structure formed of dense ivory bone (Fig. 4.11B). The lateral semicircular canal is the single most important landmark, because it “unlocks” the position of the other important structures. The lateral semicircular canal has a constant anatomical relationship to the facial nerve and stapes, and it defines the location of the facial recess opening. The mastoidectomy is then developed widely, exposing the tegmen plate superiorly and the sigmoid sinus posteriorly, and thinning the posterior bony canal wall inferiorly (Fig. 4.11B). All the air cells are removed down to the mastoid tip.
The attic should be opened by performing a transmastoid atticotomy (the option also exists of performing a transcanal atticotomy, described later, if the epitympanum is shallow). Generally, if the ossicular chain is intact, the incus should be disarticulated from the stapes before drilling. If extensive cholesteatoma is identified one may remove the incus at this time to further open the space and allow more exposure during the facial recess approach. The bone over the fossa incudus should be thinned to an eggshell and opened with a curette to avoid drilling on the incus. Placing a little saline irrigation in the floor of the antrum bends the light so that the incus can be spotted early. The amount of exposure gained depends on the height of the attic (ie, the distance between the tegmen tympani and the superior aspect of the bony canal). The tegmen is followed forward toward the zygomatic root (Fig. 4.12). The posterior bony canal is thinned down to the level of cortical bone but not fenestrated. The bony canal is shaped like a truncated cone rather than a cylinder, so that more room is gained as one progresses medially.
Once the atticotomy is completed, the incus and malleus head will be exposed (Fig. 4.13). When cholesteatoma is present in the attic and antrum, the sac is incised and its contents removed with cup forceps and submitted (Fig. 4.14A,B). The medial wall of the sac can be maintained until it is certain that there is not a fistula of the lateral semicircular canal. If the incus body is encased in cholesteatoma it is removed after detaching it from the stapes (ideally performed earlier) and malleus with a curved pick. The malleus head can be detached from the manubrium with a malleus nipper. The malleus is narrowest at its neck, just above the tensor tendon; the nipper is a delicate instrument and can only be successfully closed at that point. Occasionally the sac travels lateral to the malleus and incus and the ossicles can be preserved, but this is an infrequent occurrence.

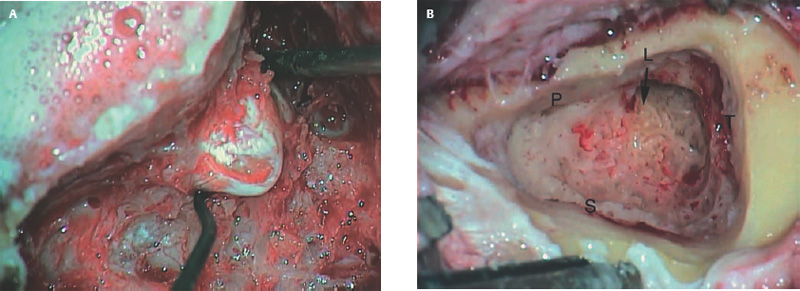
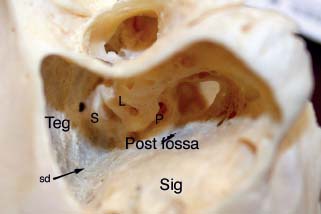
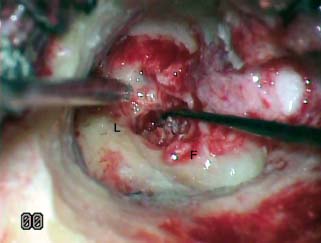
Fig. 4.11 (A) Cholesteatoma usually fills the mastoid antrum, and the sac must be incised and delivered before the deeper structures can be identified. (B) Once the antrum is opened, the lateral semicircular canal (L) can be identified in its floor, a smooth prominence of dense ivory bone. This is the key landmark to all the structures in the middle ear and mastoid. The margins of the mastoidectomy are the posterior canal wall (P), the tegmen (T), and the sigmoid sinus (S).
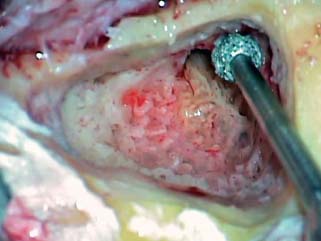
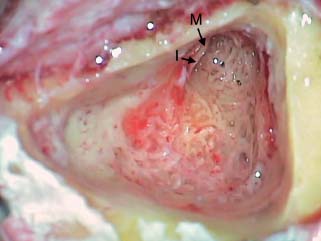
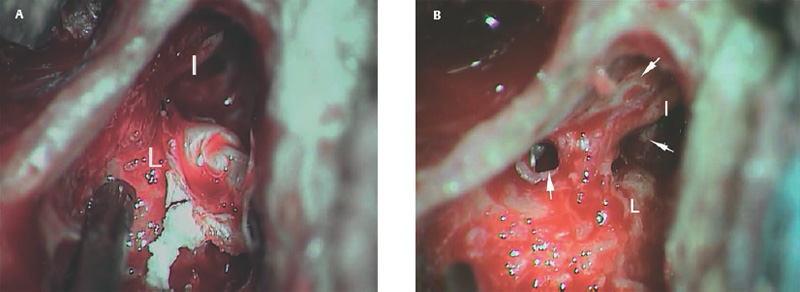

Fig. 4.15 In preparing to drill the facial recess, the facial nerve should be located, using available landmarks. The lateral semicircular canal (L) defines the medial-to-lateral depth of the facial nerve, and the incus (I) points to the facial nerve (dashed line). The facial recess drilling begins just lateral to the line of the facial nerve, at the level of the fossa incudus.
The anterior epitympanum is accessed by removing the “cog,” the bony bridge found anterior to the head of the malleus that divides the epitympanic space into posterior and anterior compartments. The cog can be perforated with a small diamond burr or curette. The anterior epitympanic space is capacious, roughly equal in volume to the posterior epitympanic space, and if disease is present there the canal wall will probably have to be removed to obtain adequate exposure.
The middle ear is accessed from the mastoid through the facial recess approach (synonymous with “posterior tympanotomy”). The facial recess is a triangular space bounded by the facial nerve medially, the chorda tympani nerve laterally, and the incus buttress superiorly. The mastoid segment (vertical portion) of the facial nerve is located at the level of the lateral semicircular canal and is encased in labyrinthine (dense ivory) bone (Fig. 4.15). Superiorly the incus points to the facial nerve. Inferiorly the facial nerve terminates at the digastric ridge.
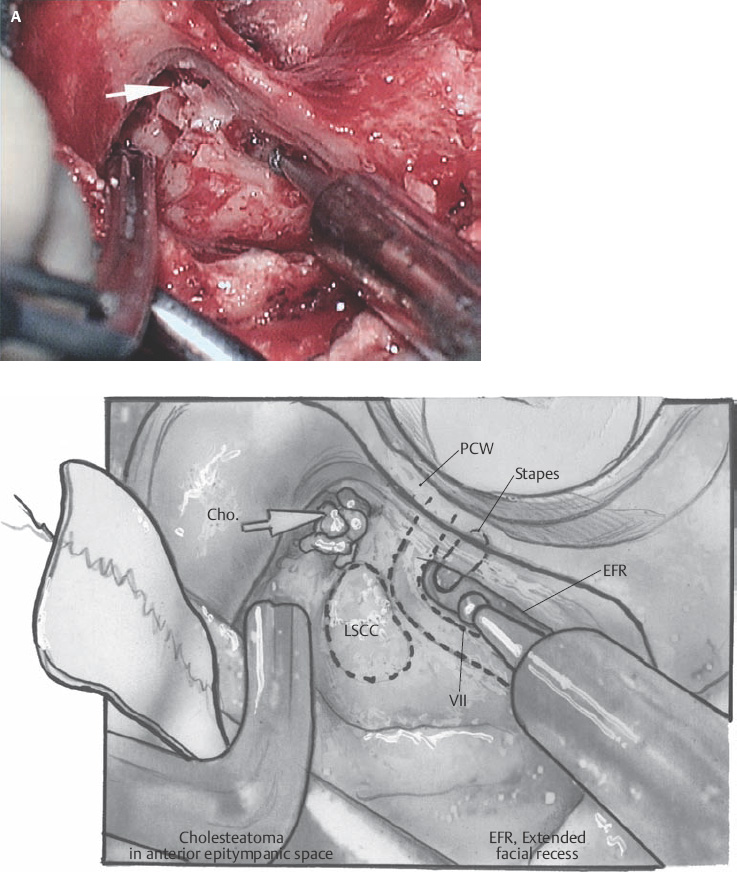
The facial recess is opened by drilling inferior to the fossa incudus, just lateral to the plane of the lateral semicircular canal, running the burr in parallel with the line of the facial nerve (Fig. 4.16A,B). The facial recess is an anatomically preformed air cell tract, gray in color and porous in texture, distinct from the ivory bone that envelops the facial nerve medially. The facial recess opening is widened in an inferosuperior direction, paralleling the facial nerve, and deepened in an anteromedial direction toward the middle ear. As drilling progresses, the burr is held at an increasingly vertical angle, describing an arc that follows the circumference of the facial nerve. The nerve should be skeletonized but not exposed, maintaining its protective bony covering. Once the middle ear is entered, the pyramidal process and round window niche will be identified (Fig. 4.17A,B). The facial recess opening can be enlarged vertically by drilling the bone anterior to the facial nerve, and by drilling laterally to the tympanic annulus. It can be enlarged superiorly by removing the incus buttress. If even greater exposure is needed, the facial recess can be widened inferiorly by transecting the chorda tympani.
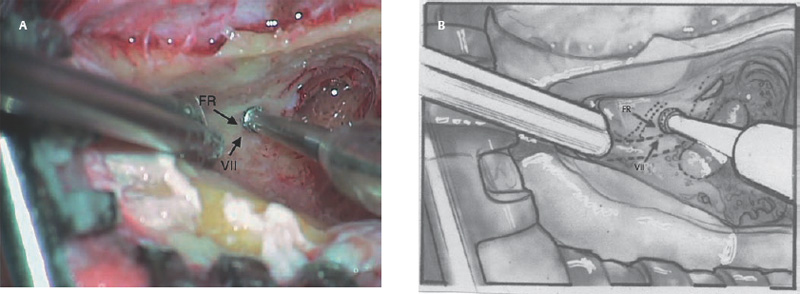
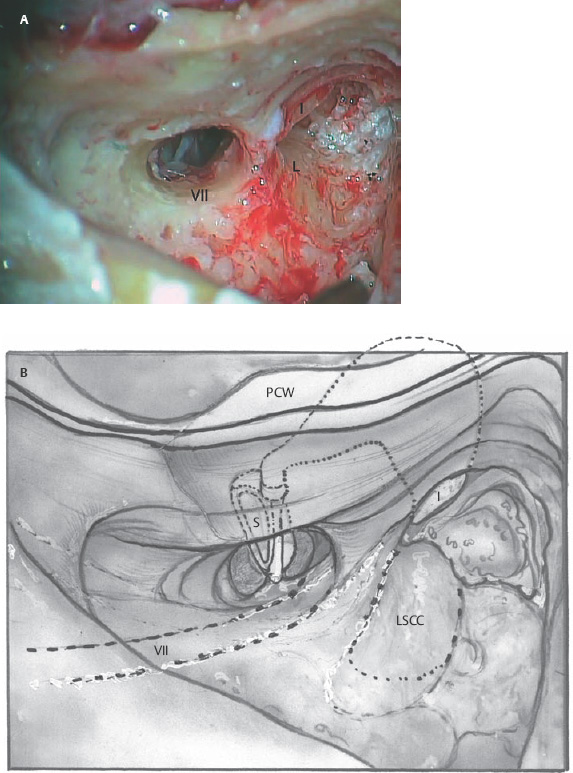
Fig. 4.17 (A,B) The completed facial recess opening allows access to the middle ear. Here, the facial nerve (VII) is skeletonized, and the relationship between the lateral semicircular canal (L), incus (I), and facial nerve is well demonstrated. Through the facial recess, the stapes, pyramidal process, and stapedius tendon can be seen. Extending the opening inferiorly would provide a good view of the round window niche.
An adequate facial recess opening allows the surgeon to clear disease from the middle ear under direct vision (Fig. 4.18A,B). The problem areas of the middle ear are the region of the facial nerve second genu, the stapes superstructure, the oval window, the sinus tympani, the round window niche, the hypotympanic cells, and the protympanum. Opening the facial recess, removing the incus, and removing the incus buttress creates an unobstructed view into the middle ear and allows the surgeon to access all these areas (Fig. 4.19A,B). In some cases, the facial recess will need to be extended downward by transecting the chorda tympani nerve.
It is important to remove the mastoid air cells of the tegmen mastoideum and tegmen tympani to eliminate secreting cells in the diseased ear. The remaining mastoid cells can be exenterated, if necessary because of the extent of the cholesteatoma, by removing the bone of the sinodural angle and opening the air cells in the mastoid tip down to the digastric ridge and anterior to the sigmoid sinus down to the posterior fossa dural plate. The retrofacial air cell tract can be safely opened once the mastoid segment of the facial nerve has been skeletonized. Radical removal of all the mastoid cells leaving only cortical bone (termed subtotal petrosectomy by Fisch)5 is not routinely performed but is necessary in cases of extensive mucosal disease, or in cholesteatosis, where the disease is poorly encapsulated and fills all the air cells.
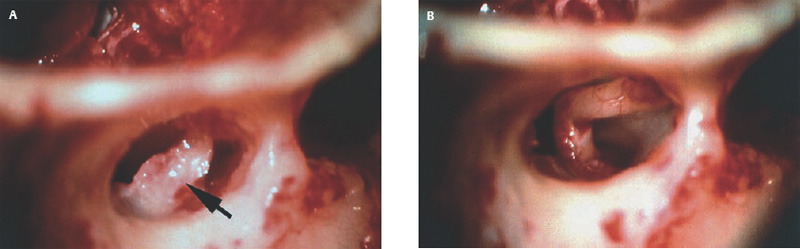
Fig. 4.18 (A) Facial recess approach to a cholesteatoma sac involving the left middle ear (arrow) before and (B) after dissection.
Surgical Decision Making: When to Take Down the Canal Wall
The decision to take the canal wall down can be made during the surgical procedure.4 The canal wall up mastoidectomy provides access to all areas of the mastoid, epitympanum, and middle ear, and any cholesteatoma can theoretically be removed by this approach. All these regions are visible after the attic and facial recess are widely opened and the incus and malleus head and cog are removed. Dissection of the disease requires working on both sides of the canal wall, so that the patient’s head will be tilted away from the surgeon during dissection of the mastoid and toward the surgeon when the surgeon is working in the middle ear. The bony canal is a barrier that can make the dissection tedious, however, and the completeness of the resection uncertain.
The primary goal of cholesteatoma surgery is the complete removal of the disease. The main disadvantage of canal wall up surgery is the chance that residual disease will remain hidden behind the intact canal wall and not be detected postoperatively. Residual disease can be left anywhere in the mastoid and middle ear cleft, but the most likely places for failure are the anterior epitympanic space, hypotympanum, and sinus tympani. More pneumatized mastoids and middle ear clefts are more dangerous because of the extension of the cholesteatoma into places that are difficult to reach. In cases with poor visualization or limited access, the canal wall will have to be removed.
The first decision point in mastoid surgery is when the attic is opened through the mastoid (transmastoid atticotomy). There must be adequate surgical exposure to completely dissect the matrix from the epitympanic spaces. As discussed earlier, the anterior epitympanic space can be quite large, and the distance between the tegmen and the bony ear canal is the limiting factor in obtaining adequate exposure. Taking down additional bone will result in an excessively large scutum defect, which can be an invitation for recurrence, even when repaired with cartilage (Fig. 4.20A–C). An alternative strategy in cases of anterior epitympanic cholesteatoma is to perform a transcanal atticotomy, removing the scutum widely to exteriorize the sac through the external canal. The result will be a large, shallow middle ear and the need to reconstruct the scutum with cartilage. It is often better to convert to a canal wall down mastoidectomy in these cases.
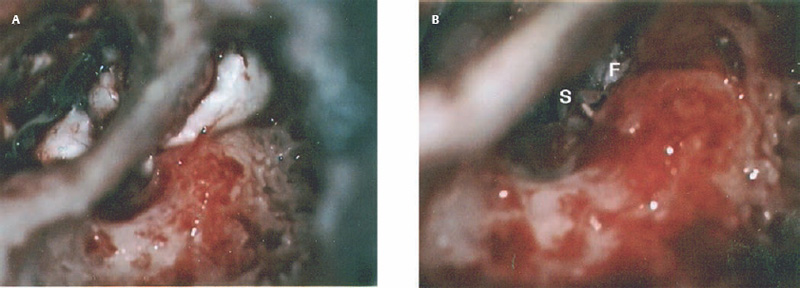
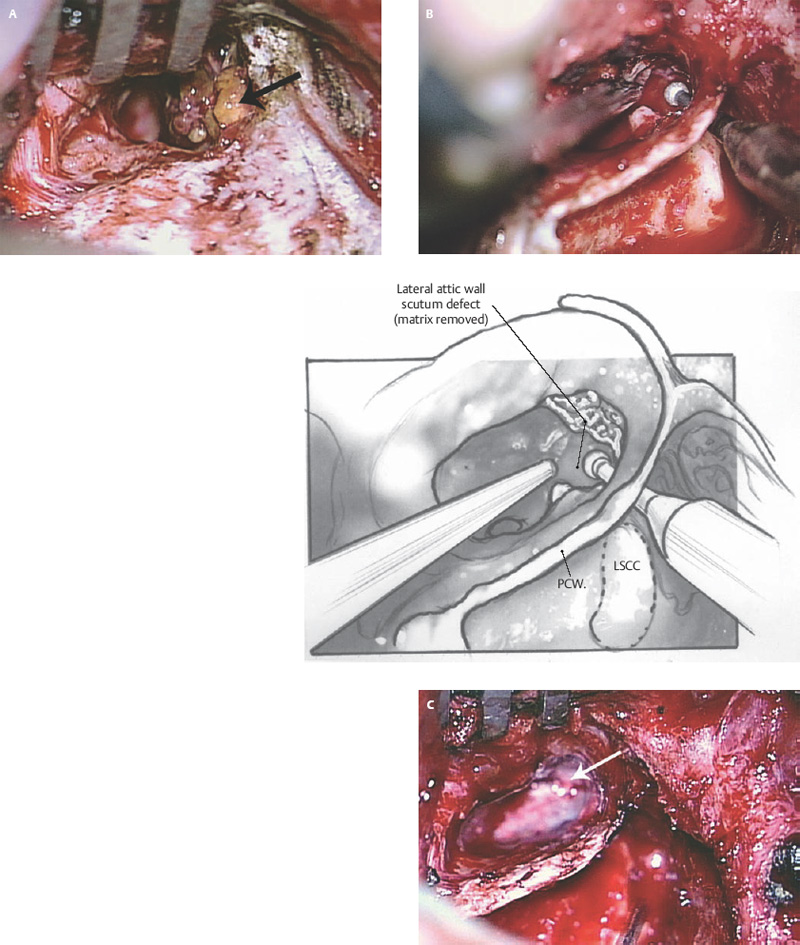
Fig. 4.20 A large scutum defect should be avoided, as it can provide a passageway for recurrent cholesteatoma to form. (A) An attic cholesteatoma that had eroded the scutum (black arrow). (B) A transmastoid atticotomy allows complete removal of the sac. The burr demonstrates the large scutum defect that remains. (C) A cartilage graft (white arrow) is needed to close the bony defect.
The second decision point is when the facial recess is opened to enter the middle ear. The sinus tympani is accessed through the facial recess opening, and exposure there too can be limited. Vertically widening the facial recess and removing the bone anterior to the facial nerve are ways to maximize exposure. In cases of posterior mesotympanic cholesteatoma, where the tympanic membrane is collapsed against the promontory, dissecting the sac out of the sinus tympani can be difficult, and if the sac epithelium ruptures, the likelihood of residual disease increases. Atelectasis of the posterior mesotympanum usually requires a canal wall down procedure because the posterior tympanic membrane will usually re-collapse into the middle ear space postoperatively, leading to recurrence (this is discussed further in Chapter 6, in the sections on Sinus Tympani Disease and Collapsed Middle Ear Space).
Canal Wall Down Mastoidectomy
Canal wall down mastoidectomy provides unrestricted surgical access to the middle ear and mastoid by creating an open cavity. It carries a lower rate of residual and recurrent disease than canal wall up surgery, and is generally more successful in creating a “safe” ear. However, the resultant cavity may be prone to drainage and may require periodic cleaning and “toilet” (maintenance in the office), which can be problematic, especially for children and for unreliable patients.
The canal wall down procedure is favored in certain situations: when the disease is extensive or cannot be completely removed, when the mastoid is small and sclerotic, when the patient cannot be relied upon for follow-up, when the canal wall is eroded by the disease, when the disease is recurrent, when there is a complication such as lateral semicircular canal fistula, when one is dealing with an only hearing ear.
The canal wall down procedure can be planned in advance or can be converted from canal wall up during the surgery (Fig. 4.21A,B). It can be performed from behind forward, or by following the disease from the attic back (inside-out or retrograde mastoidectomy). A canal wall down mastoidectomy can be performed with removal of the middle ear contents (radical mastoidectomy), in conjunction with tympanoplasty and ossicular reconstruction, or without entering the middle ear at all (Bondy operation).
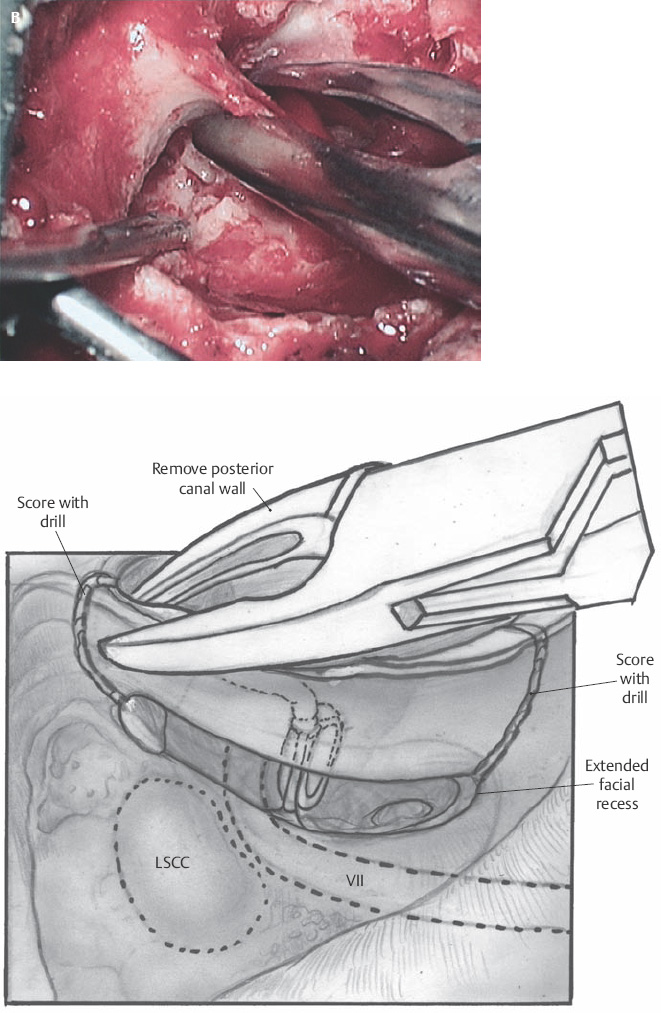
The back-to-front approach to canal wall down mastoidectomy begins with the canal wall up procedure already described. Once the mastoid landmarks are identified, the canal wall can be taken down with a cutting burr, beginning in the attic where the bony canal meets the tegmen, and progressively lowering the bone toward the mastoid segment (vertical portion) of the facial nerve. Alternatively, the facial recess can be opened first, and then the canal wall can be taken down en bloc (Fig. 4.21A,B). The latter approach has the following advantages: (1) the facial nerve is identified early and thus protected from surgical trauma; (2) the facial ridge is maximally lowered, resulting in a more manageable cavity; (3) the bony canal wall can be removed quickly using rongeur rather than drill; and (4) the bony canal wall can be saved and used later for cavity obliteration.
If the mastoid is well developed, it is important to exenterate all the air cells so that only cortical bone remains. Leaving pockets of cellular bone will result in postoperative mucositis and drainage. Measures that can be taken to reduce the size of the mastoid are described following here. If the mastoid is diploic, it may not be necessary to remove all the marrow-containing spaces. Often the cavity can be sculpted into a round, well-beveled shape, using a diamond burr to polish the bleeding edges. If the mastoid is sclerotic, the disease-containing spaces can be opened, and the remaining bone can be contoured to result in a round, compact cavity without removing the entire mastoid tip.
The canal wall down mastoidectomy can also be performed in a front-to-back, or inside-out, fashion. This method is ideal when it has been decided in advance that the canal wall will be taken down, such as in a sclerotic mastoid with disease localized to the attic and antrum. This inside-out method is used when one is performing the Bondy operation, described in greater detail later in the chapter, in which a small canal wall down cavity is created without entering the middle ear. It is also used in the technique of “retrograde mastoidectomy,” described by Dornhoffer,6 in which the disease is followed from its origin in the middle ear or epitympanum, to its posterior limit in the mastoid. In Dornhoffer’s method, a limited portion of the posterior canal wall is removed in the attic, and the mastoid is opened only as much as needed to expose the disease. The remainder of the canal wall is not removed, but the canal wall defect is repaired with a cartilage graft harvested from the cimbum concha to result in a closed cavity.
Creating a Manageable Cavity
Creating a manageable cavity requires four steps: (1) beveling the cavity edges; (2) lowering the facial ridge; (3) amputating the mastoid tip; and (4) creating an adequate meatoplasty.7 Careful attention to these steps will result in a compact but well aerated cavity that can be inspected and cleaned in the office without difficulty.
The edges of the cavity are beveled while the surgeon is drilling the cortical bone near the tegmen and behind the sigmoid sinus (Figs. 4.22A,B and 4.23A,B). The tegmen has a rounded contour, like the bottom of a boat, and laterally near the squamosa it turns upward. Removing the sharp ridge of bone will prevent tenting of the canal skin at this location. The position of the sigmoid sinus in the mastoid can be highly variable, and the retrosigmoid air cells can be very well developed and in some cases go all the way back to the lambdoid suture. Removing these cells can help prevent pockets that can be inaccessible in the postoperative cavity. The anterior epitympanic space is opened by removing the bony cog. The anterior canal wall bone should then be smoothed with a diamond drill, so that it becomes confluent with the anterior wall of the anterior epitympanum (Fig. 4.22A,B). Sometimes the temporomandibular joint is skeletonized during this step.
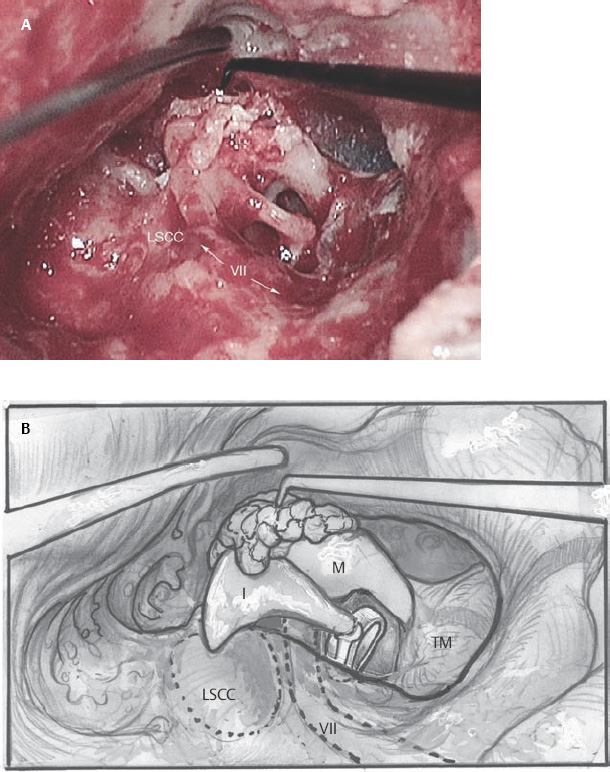
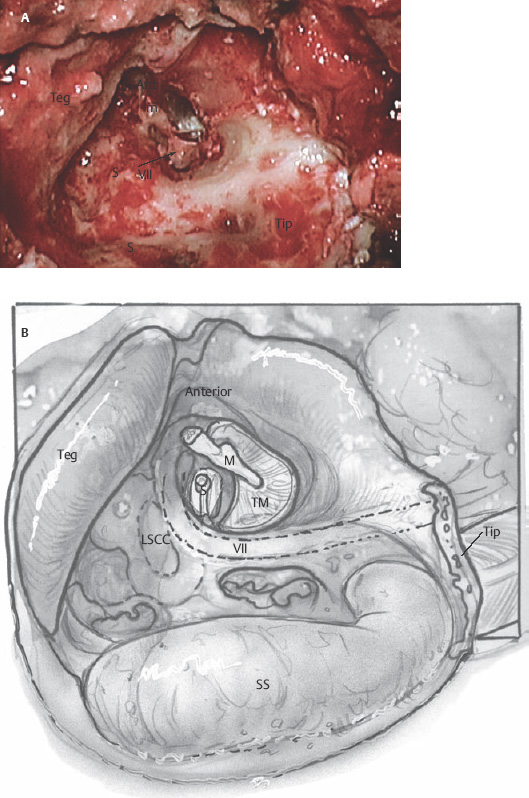
Fig. 4.23 (A,B) The canal wall down mastoidectomy, completed. The cortical bony edges have been beveled at the tegmen (Teg) and posterior to the sigmoid (S), and the inferior canal bone has been widened so that the base of the middle ear is confluent with the mastoid tip. (Tip). Note also that the facial ridge (VII) has been lowered and the anterior epitympanum (Ant) has been exteriorized, and all of the mastoid air cells have been exenterated.
Lowering the facial ridge is essential. As already noted, opening the facial recess prior to removing the canal wall ensures that this step is performed adequately. The facial nerve should be skeletonized, leaving a thin bony covering (Fig. 4.22A,B). Under high magnification and using constant saline irrigation, the nerve sheath, which is white in color and has a delicate vascularity, can be identified through a thin layer of bone. When the surgical plan does not call for entering the middle ear (eg, Bondy operation), the bone anterior to the nerve can be skeletonized with a diamond burr until the fibrous annulus of the drum is seen, while preserving the cuff of distal canal skin. At the end of the procedure, this skin can be draped over the facial ridge. In surgical cases in which the middle ear is entered, the bone anterior to the facial nerve should be removed, to gain maximal access to the sinus tympani. This is done by skeletonizing the nerve circumferentially into the middle ear space with the diamond drill and removing part of the pyramidal process if necessary. When this maneuver is completed, the round window niche, subiculum, and ponticulum should be visible.
The mastoid (vertical) segment of the facial nerve should be followed inferiorly toward the stylomastoid foramen as well, removing the triangle of bone that separates the mastoid from the hypotympanum (Fig. 4.23A,B). The goal is to avoid leaving a ridge of bone that prevents access to the mastoid tip cells postoperatively. The bony tympanic ring is usually quite thick, and so the bone that forms the inferior canal wall can be thinned aggressively with a coarse diamond drill. Ideally, the floor of the ear canal can be brought down as low as the mastoid tip, avoiding a dependent group of tip cells that could later collect debris and be difficult to clean.
Amputating the mastoid tip is important to ensure that there won’t be dependent cells that can drain postoperatively or harbor recurrence. In a well-developed mastoid, the mastoid tip is bisected by the digastric groove, which is formed by the posterior belly of the digastric muscle (Fig. 4.23A,B). A large diamond burr can be used to remove the tip cells lateral to the digastric. Once these cells are removed, the periosteum of the digastric can be exposed and be followed anteriorly where it merges with the facial nerve sheath to form a fibrous ring at the stylomastoid foramen. External to the mastoid tip, the tendinous insertion of the sternocleidomastoid muscle adheres tightly to the bone and should be stripped with a periosteal elevator. The remaining bony cortex of the tip can then be fractured with a rongeur. Once the tip is amputated, the muscles will collapse medially to obliterate this potential space. The sternocleidomastoid tendon can even be sutured to the digastric periosteum at the time of closure.
It may seem paradoxical that removing more bone will result in a smaller cavity. Beveling the cortical edges above the tegmen and behind the sigmoid, lowering the facial ridge and removing the triangle of bone between the hypotympanum and mastoid, and amputating the mastoid tip are all steps that allow the soft tissues to collapse medially, resulting in a smaller cavity (Fig. 4.23). Producing an adequate meatoplasty ensures that an open but compact cavity results that is easy to inspect and clean postoperatively (meatoplasty is discussed in detail in Chapter 5).
The Bondy Operation (Retrograde or Inside-Out Mastoidectomy)
The Bondy operation is an inside-out atticoantromy and is ideal for attic cholesteatoma in a compact mastoid. The principle of the Bondy operation is the exteriorization of disease to create a “safe” ear. The virtue of this operation is that it avoids the middle ear and potentially spares the hearing mechanism. Bondy first described his modified mastoid procedure in 1910,8 at a time when otologic surgery was performed without a microscope, a drill, or antibiotic coverage, and radical mastoidectomy was the standard of care. Bondy realized that some patients with good preoperative hearing have a cholesteatoma limited to the attic exclusively, not involving the entire mastoid and middle ear. In an attempt to preserve hearing that would be destroyed in a radical mastoidectomy, he developed the more limited Bondy procedure, opening the diseased attic but leaving the eardrum and ossicular chain intact.
Characteristic and Alternative to Canal Wall Up and Down Procedures
Today’s treatment for chronic otitis media with cholesteatoma has evolved from these early attempts at modification and perfection of surgical techniques and meticulous documentation of follow-up. Tympanoplasties with intact canal wall or canal wall down mastoidectomies have their indications, but modifications of these standard procedures continue to be an excellent alternative in certain subsets of patients. The distinct differences to the conventional mastoidectomies make the procedure unique.
Most important advantages of an intact canal wall are the “normal” postoperative anatomy, better hearing results, and the unrestricted lifestyle, especially for water restriction and follow-up cleaning. Especially in the pediatric population, limited mastoidectomies are favored over radical mastoidectomies due to the morbidity of leaving a mastoid cavity. But their limitation is reached when the disease process leading to a significantly contracted and sclerotic mastoid, posterior canal wall erosion, the presence of matrix over lateral canal fistula, and therefore limited mastoidectomies/atticotomies may be favorable.9 Many authors believe that a limited atticotomy will lead to wider than normal but self-cleaning cavity,10 an important factor in the pediatric population.
The inside-out approach described by Roth and Haeusler uses an extended Bondy technique if the cholesteatoma expands deep to the ossicles into the meso- or hypotympanum.10 The posterior canal wall is progressively drilled inferiorly, and the middle ear space is also included into the resection, as dictated by the extent of the cholesteatoma. Instead of drilling the entire mastoid bone they recommend only removing bone overlying the cholesteatoma. This stepwise approach starts with a Bondy operation and opening the mastoidectomy leading to a radical cavity in the worst case scenario, but leaving more inferior aspects of the mastoid untouched if they are not involved with cholesteatoma.
Technique of Bondy Operation
The procedure is usually done through a postauricular incision, although a transmeatal approach using endaural incisions can be performed in a sclerotic mastoid. The object is to first exteriorize the attic by removing the scutum, then follow the tegmen tympani posteriorly until the antrum is opened as well. This is accomplished while staying out of the middle ear space.
If a postauricular approach is used, the periosteum is incised along the linea temporalis as far forward as the zygomatic root, to have exposure of the entire tegmen. The cortical bone is then removed with a cutting or coarse diamond burr until the lateral edge of the tegmen is skeletonized. The tegmen is then followed medially, and, in so doing, the scutum is progressively thinned down to an eggshell. A curette can then be used to complete the atticotomy so as to avoid drilling directly on the malleus and incus. Once this is done, the tegmen can be followed posteriorly, removing the cellular or hypocellular bone until the antrum is exposed (Fig. 4.24). As the drilling progresses, the mastoidectomy that is created is kept in a round shape, paralleling (and enlarging) the curve of the posterior canal wall and beveling the posterior bony edges (Fig. 4.25). The posterior limit of drilling is defined by the posterior extent of the antrum—it is not necessary to expose the sigmoid sinus or remove the mastoid tip. It is necessary to create a round, well-beveled cavity, so once the antrum is opened, the cortical bony edges are smoothed widely and the cavity is contoured. The posterior canal wall is removed during the Bondy procedure, beginning at the antrum and progressing inferiorly and backward (Fig. 4.26). The lateral semicircular canal can be used as a landmark once the antral contents are exposed and mobilized. If a diamond drill is used, the cuff of posterior canal skin that is attached to the tympanomeatal flap can be redraped over the facial ridge at the end of the procedure (Fig. 4.27).
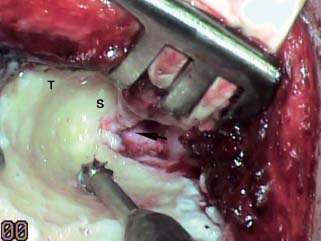
Fig. 4.24 Bondy procedure, right ear. The cholesteatoma sac grew from the posterior middle ear (arrow) toward the attic and antrum, and the mastoid was sclerotic. A drill is used to perform an atticoantrotomy, beginning at the tegmen (T) and thinning the scutum (S) to an eggshell, and enlarging the posterior bony canal wall to form a round, beveled cavity.
Functional Results and Recurrence
DeRowe et al11 reviewed 53 children having undergone an endaural atticotomy; even though 72% of the patients required an ossiculoplasty due to the extent of the cholesteatoma, 28% underwent a true modified Bondy mastoidectomy. Twenty-one percent of their patients needed a revision; of those, three quarters required resection of the ossicles at the first procedure. Even though the relative risk was not calculated, a trend is visible. Twenty-two percent complications were noted, of which 15% were retractions. Therefore Rakover et al stress the need for ventilation tubes at the time of surgery because they may significantly decrease the rate of recurrent cholesteatoma or the development of recurrent retractions.12
Bondy’s findings on hearing outcome after mastoidectomy from 100 years ago were confirmed even in today’s literature in a large review of more than 600 patients at the University of Berne.10 The postoperative hearing result is largely dependent on preoperative auditory conditions. Preservation of good preoperative hearing was noted after a Bondy operation when compared with a canal wall down procedure.13
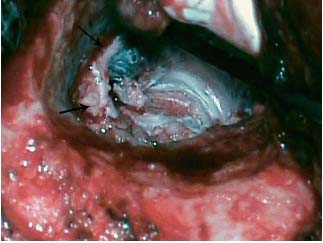
Fig. 4.27 The tympanomeatal skin is replaced (arrows), and used to reline the mastoid cavity.
Sanna et al reviewed their experience of 222 patients undergoing the Bondy mastoidectomy.14 Despite a low complication rate of 19%, which include 7% residual cholesteatoma, draining cavity 7.3%, and effusion 5.2%, the long-term hearing result was excellent. Eighty-eight percent of patients had stable or even improved hearing over a 5-year period. Similar excellent hearing results were found by Berrettini et al in 53 patients reviewed with 91% hearing preservation or improvement.15
Today’s Value of the Modified Bondy Mastoidectomy
Following Bondy’s description the indication for the procedure in 1910 remains unchanged today: attic cholesteatomas or deep retraction pockets with a normal middle ear and intact ossicular chain. Sanna et al14 summarized preoperative indications for the Bondy procedure:
• Epitympanic cholesteatoma in normal or good-hearing ear (preoperative air–bone gap, ≤25 dB) with an intact ossicular system and mesotympanum free of disease
• Epitympanic cholesteatoma in the better or only hearing ear
And intraoperative indications:
• Epitympanic cholesteatoma in the better or only hearing ear with slightly compromised but still transmitting ossicular chain
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


