Fig. 794 Guilford’s mastoid tip removal. After a canal wall–down mastoidectomy has been performed in an endaural approach and it has been recognized that the air cells and the pathology extend far down into the mastoid tip, a retroauricular incision over the mastoid tip is performed. The skin is elevated, and the mastoid tip is exposed by removal of the muscle fibers covering the mastoid tip. The air cells are exenterated using a large cutting burr. In the tympanic cavity, the incus is extruded, and the posterior part of the drum is elevated. The upper border of the endaural canal wall–down mastoidectomy cavity is indicated by a dashed line
Elevation of the periosteum and the muscle fibers from the mastoid tip are not absolutely necessary before drilling. Using a large diamond drill, the bone can be removed, leaving the periosteum and the muscle fibers attached.
The detached periosteum and the sternocleidomastoid muscle fibers are pressed onto the bone (Fig. 801), covering the most distal part of the mastoid tip. The wound is closed, whilst overlying and surrounding fibrous tissue covers the inner table of the mastoid process. The outer dressing presses the auricle medially, securing the inferior part of the cavity and the mastoid tip area. Of course, a tympanoplasty and a meatoplasty have to be performed to manage the upper part of the cavity as an open cavity: alternatively, an obliteration using a superiorly-based temporalis muscle flap can be performed.

Fig. 795 The mastoid tip cells are further exenterated, and all the cortical bone of the mastoid tip is exposed
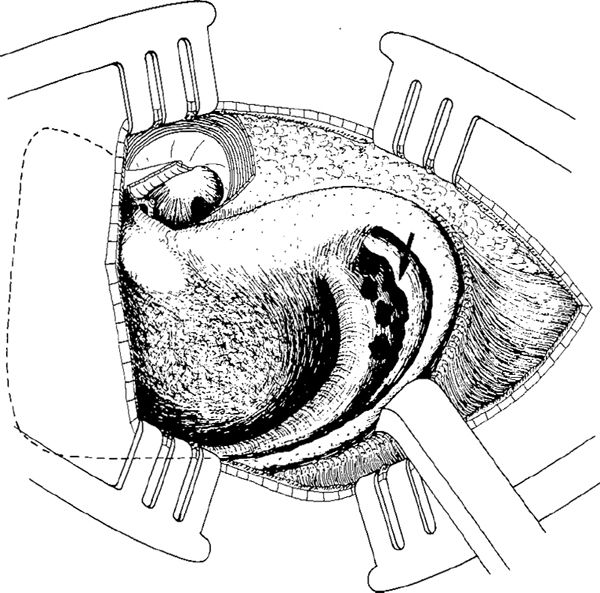
Fig. 796 The mastoid tip air cells are exenterated down to the digastric crest (arrow). There are still some deep cells between the sigmoid sinus and the digastric crest. Around the mastoid tip, the periosteum and muscle fibers are elevated with a periosteal elevator
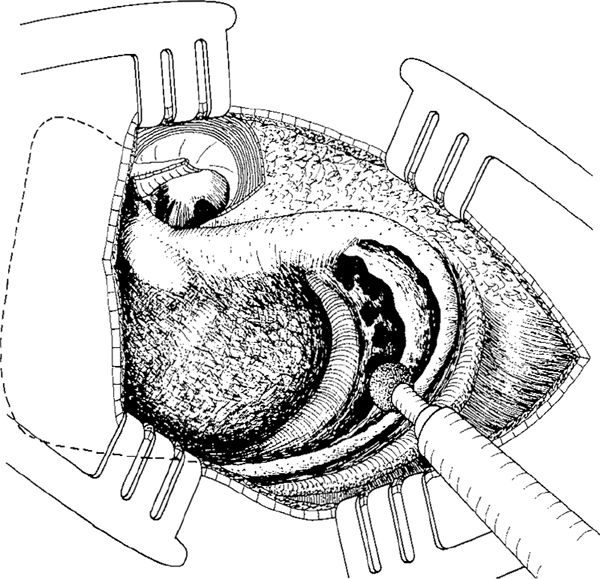
Fig. 797 The thin cortex of the mastoid tip is drilled away, starting with a large diamond burr at the posterior edge, and continuing down the tip
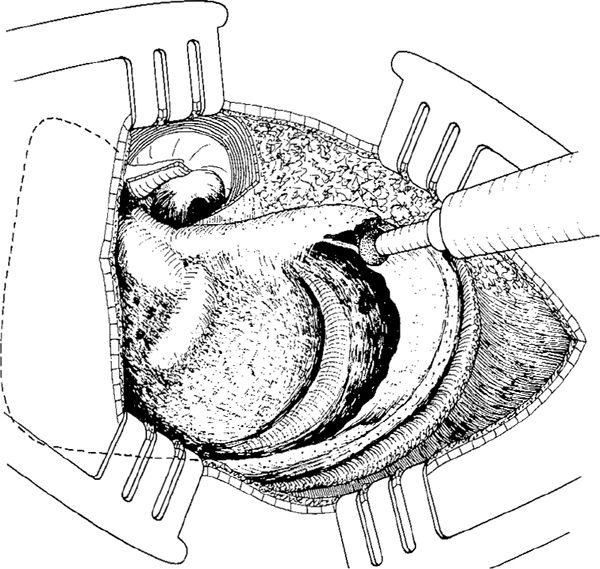
Fig. 798 The posterior and inferior cortex of the mastoid tip is removed. The drilling continues along the anterior border of the mastoid tip cortex
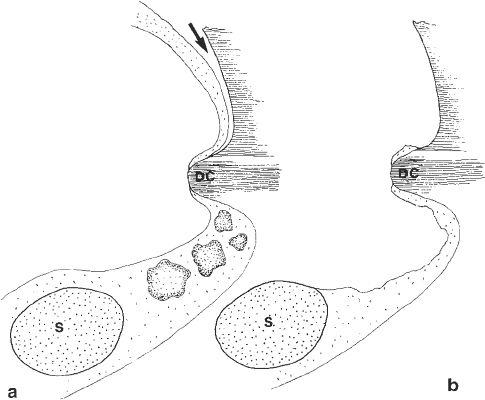
Fig. 799 Side view of the mastoid tip cortex. a After exenteration of the cells, the digastric crest (D) is exposed to a whitish area consisting of periosteum fibers. Laterally to it, the cortical bone of the tip is still in place, and the periosteum (arrow) is elevated from the cortical bone. Medial to the digastric crest, there are still some air cells between the digastric crest and the sigmoid sinus (S). b The cortical bone from the mastoid tip is removed up to the digastric crest, which is exposed. The cells located medially to the digastric crest and interiorly to the sigmoid sinus are exenterated
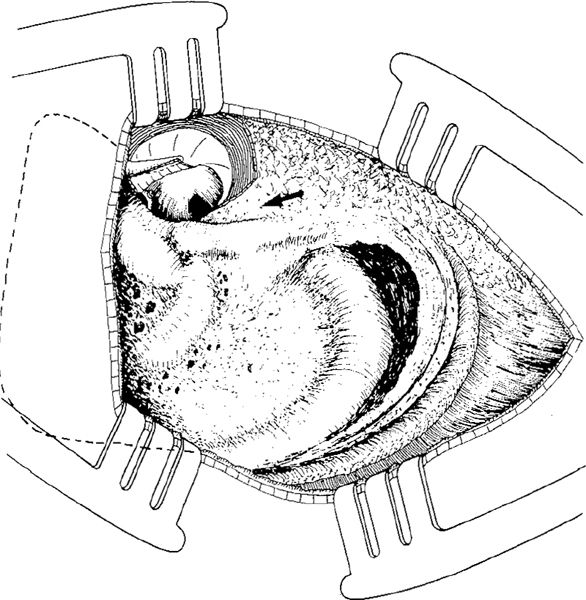
Fig. 800 All cortex from the mastoid tip is removed, and the facial ridge is maximally lowered and completely eliminated. The posterior part of the tympanic bone (arrow) is drilled away, making a gradual transition from the tympanic bone to the mastoid tip

Fig. 801 The detached musculoperiosteal tissue from the mastoid tip covers the digastric crest and the most inferior part of the mastoid tip area. A Gelfoam ball (or a free muscle graft) is placed in the deepest part of the cavity, between the digastric creast and the sigmoid sinus. S: sigmoid sinus; DC: digastric crest
Obliteration of the Mastoid Tip Area
If the mastoid tip area is deep, with exenterated air cells extending between the digastric crest and the sigmoid sinus, the cavity can be obliterated. The obliteration involves the entire inferior half of the mastoid cavity. Guilford (1960) used two flaps. The first flap is cut from the posterior region of the mastoid process, and is inferoposteriorly based (Fig. 802). Its superior part consists of fibrous tissue and periosteum. Its inferior part consists of splenius capitis muscle and transversus nuchae muscle fibers. In order to harvest the flap posteriorly, the skin has to be elevated extensively. The flap is placed in the posterior part of the cavity (Fig. 802).
In order to obliterate the anterior part of the mastoid tip, a piece of sternocleidomastoid muscle can be dissected as an inferiorly-based flap, and turned into the mastoid tip area (Fig. 803). Guilford placed a guide suture in the upper end of the flap to pull it through the cavity and the external auditory canal, in order to hold the flap in place while the retroauricular incision is closed with sutures.
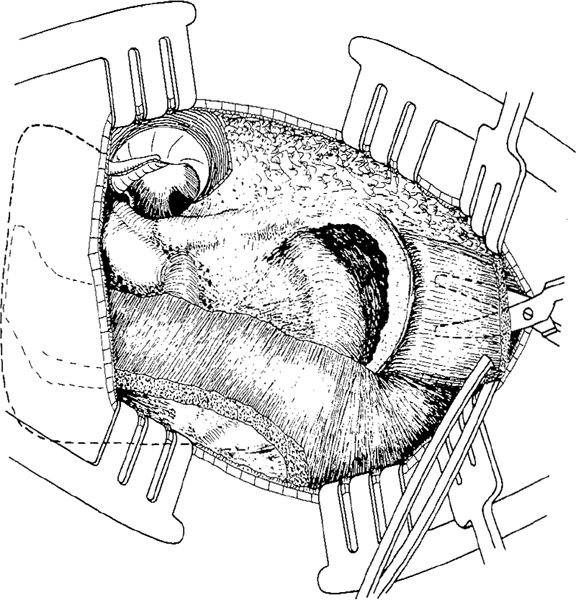
Fig. 802 Guilford’s obliteration of the mastoid tip area. An inferiorly-based flap, consisting of muscle fibers and fibrous tissue harvested from the region behind the cavity, is placed in the posterior part of the cavity. The flap is based inferoposteriorly. The present author covers the anterior part of the mastoid tip area with a small muscle flap, elaborated from the sternocleidomastoid muscle
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


