Chapter 22 Laser Stapedotomy
 Videos corresponding to this chapter are available online at www.expertconsult.com.
Videos corresponding to this chapter are available online at www.expertconsult.com.
The surgical treatment of otosclerosis has been evolutionary in nature. Multiple techniques are now available to accomplish the same goal, which is illustrated by the number of chapters devoted to this subject in this book. The small fenestra technique evolved as a less invasive method to accomplish stapedectomy.1 It allows a smaller opening into the inner ear with the potential for less surgical trauma. Many techniques have been used in the past to accomplish a small fenestra, including a manual pick method, a hand drill, a microdrill, and a laser technique.2 The laser technique was developed by Perkins3 in the early 1980s. Several different lasers have been used to perform the small fenestra, including argon, KTP, and CO2.4–6 A hand-held fiberoptic probe or a micromanipulator can be used to deliver the laser beam, and each method has its champions.7
PREOPERATIVE EVALUATION
The surgical candidate should have a conductive hearing loss on audiogram and confirmed by tuning fork of at least 15 dB. Acoustic reflexes can be used as a simple screening tool for conductive hearing loss owing to superior canal dehiscence, and should be absent. The tympanic membrane should be intact, and there should be no evidence of ongoing infection in the ear. The patient should not have evidence of cochlear hydrops (see the section on pitfalls). The patient should have no medical contraindications to a short surgical procedure performed under local anesthesia. See Chapter 21 for indications and contraindications of stapes surgery.
SURGERY
Operating Room Setup and Preparation
A support bar (Fig. 22-1) is attached to the operating table to keep the drapes off the patient’s face. By attaching the bar directly to the table, the bar moves in conjunction with the table. Using a floor-mounted device, such as a Mayo stand, does not allow the coordination of movement between the two items and can result in limitations of table movement. The operative site is prepared by surrounding the ear with a plastic drape (1030; 3M) that keeps the hair out of the operative field. The ear and a margin of the plastic drape are prepared with povidone-iodine (Betadine) solution, and the povidone-iodine solution is allowed to fill the ear canal. Intravenous midazolam (Versed) is used for sedation. This medication is given in 0.5 mg increments until the patient is sleepy and relaxed. Typically, the patient requires 4 to 5 mg. Intravenous meperidine (Demerol), given in 12.5 mg increments, can be used to supplement the midazolam. An antiemetic such as ondansetron (Zofran) is also administered during surgery. The amount of sedation is titrated to the point that the patient is somnolent, yet appropriately responsive. At this point, 3 mL of blood is drawn and transferred to the scrub nurse.

Surgical Technique
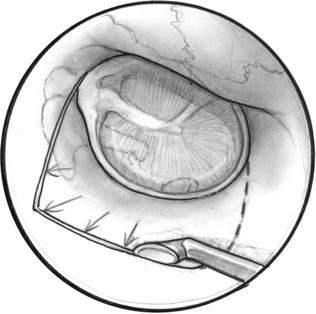
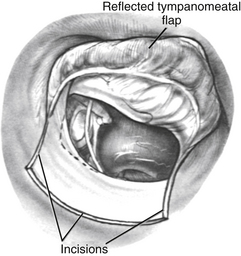
A tympanomeatal flap is incised using disposable tympanoplasty blades (7200 and 7210 BD Beaver). These disposable blades result in a sharp incision and rapid healing of the ear canal. Two incisions are made tangential to the annulus, one beginning adjacent to the short process of the malleus and following the tympanosquamous suture line. The second is adjacent to the tympanic annulus starting at approximately the 6 o’clock position and extending posterosuperiorly in the canal. These two incisions (Fig. 22-2) are connected with a transverse incision approximately 5 mm posterior to the tympanic annulus. The flap length is approximately the width of two Sheehy weapons (3 mm round knife). An excessively long flap would result in more bleeding, and can be difficult to fold forward in a narrow ear canal because of the bulk of the flap.
The flap is elevated inferiorly to allow visualization of the round window (Fig. 22-3). It is elevated superiorly until the neck of the malleus is visualized. The chorda tympani nerve is adherent to the posterosuperior bony tympanic annulus. It is separated from this bone, and separated from the undersurface of the malleus. Separating the chorda tympani allows mobilization of the nerve inferiorly for good visualization of the stapes, and prevents injury during curetting.
Posterior external auditory canal bone is removed with a curette to visualize the oval window. Initial curetting occurs several millimeters posterior to the edge of the tympanic annulus (Fig. 22-4). Initial curetting on the edge can result in displacement of the curette into the middle ear with dislocation of the incus. The posterior curetting allows for the bone to be weakened by creating a trough in this area. When the bone is weakened, the edge of the bone can be cracked off with the curette and little force is needed. The bone should be removed posteriorly to allow visualization of the stapedial tendon and pyramidal process (Fig. 22-5). For a right-handed surgeon working on a right ear, the bone should be removed superiorly so that half of the diameter of the horizontal fallopian canal can be visualized. For a right-handed surgeon working on a left ear, more curetting is necessary to introduce instruments in the middle ear, and bone should be removed so that the entire diameter of the horizontal fallopian canal can be visualized. At the conclusion of the curetting, all of the resultant bone chips should be removed from the ear canal to prevent postoperative healing problems.
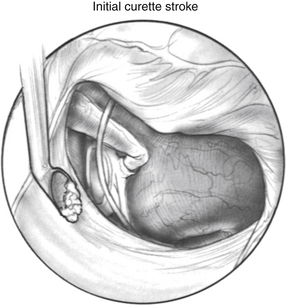
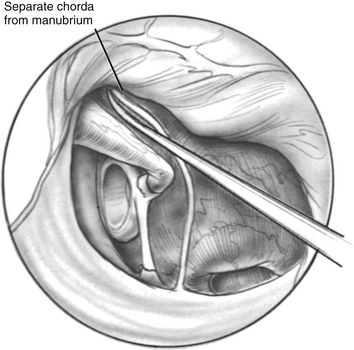
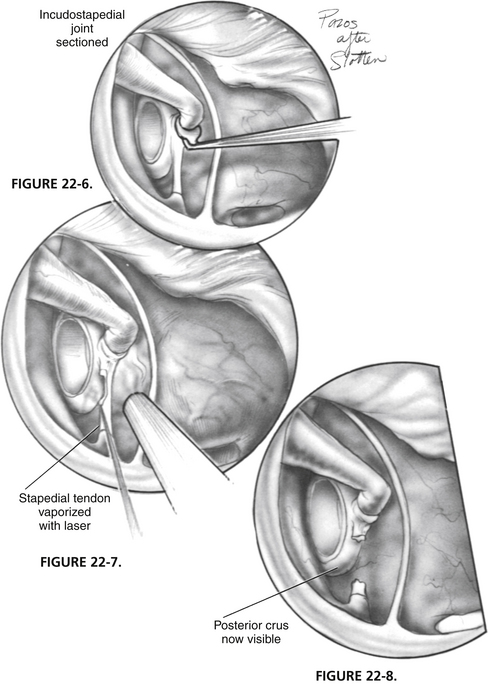
FIGURE 22-5 Completed curetting exposes stapedial tendon, pyramidal process, and horizontal fallopian canal.
The incudostapedial joint is separated with a joint knife (Fig. 22-6). The joint is typically 1 mm medial to the undersurface of the incus and can be identified by pushing the incus slightly forward and laterally. The joint is separated with a side-to-side motion by the knife. When the joint is separated, the malleus mobility is tested to rule out idiopathic malleus head fixation. The stapes is tested for motion, and the anterior oval window is inspected visually for evidence of otosclerosis. Otosclerosis can reliably be seen in this area and appears to be bright white bone with prominent vessels on it. The adjacent normal otic capsule bone looks slightly gray compared with the otosclerotic bone. If otosclerosis is not visualized, one must be quite confident that the stapes is not mobile before proceeding (see the section on pitfalls).