Chapter 34 Surgery of the Endolymphatic Sac
 Videos corresponding to this chapter are available online at www.expertconsult.com.
Videos corresponding to this chapter are available online at www.expertconsult.com.
Meniere’s disease is a clinical syndrome consisting of fluctuating-progressive hearing loss, episodic vertigo lasting 20 minutes to 24 hours, tinnitus, and aural fullness that is diagnosed when other diagnoses have been excluded. Surgical treatment of Meniere’s disease has been controversial and a focus of debate ever since Portmann1 first proposed opening the endolymphatic sac in 1927. Despite controversy, however, surgical manipulation of the endolymphatic sac to alleviate the debilitating symptoms of Meniere’s disease has been a mainstay of surgical treatment when conservative therapy has failed. The mechanism of symptomatic relief from shunting, decompressing, or excising the endolymphatic sac is also controversial.
For the purposes of this chapter, the definition of definite Meniere’s disease published by the American Academy of Otolaryngology–Head and Neck Surgery (AAOHNS) Committee on Hearing and Equilibrium in 19952 is used when referring to Meniere’s disease. The criteria given are as follows:
Meniere’s disease is difficult to study because of its fluctuant nature and the minimum 2-year time course over which results of interventions must be documented.2 The absence of a definitive test for Meniere’s disease necessitates diagnosis based on historical data. Whether or not placebo effect is the cause of success in the endolymphatic sac decompression is also controversial. Before discussing the techniques and outcomes of the endolymphatic sac procedures, we first consider the underlying anatomy and physiology.
ENDOLYMPHATIC ANATOMY AND EMBRYOLOGY
Scarpa (1752-1832) discovered and described endolymph and the membranous labyrinth in 1789,3 72 years before Méniere4 ascribed symptoms of the clinical syndrome to the inner ear. Understanding the embryology of the endolymphatic system may provide some clues to understanding Meniere’s disease. During the fourth week of embryogenesis, three buds of the primordial otocyst appear representing the pars superior, pars inferior, and endolymphatic duct, which eventually develop into the utricle and the semicircular canals, the saccule and the cochlear duct, and the endolymphatic duct and sac.5 The endolymphatic duct leaves the medial vestibule and courses dorsally through the bony vestibular aqueduct to terminate on the posterior surface of the temporal bone, enveloped within dural folds of the posterior fossa. The short, straight endolymphatic duct acquires its mature hook shape configuration by the fourth year of life.6,7 Histologic and functional maturation of sac elements may predate complete anatomic maturity. Potassium-rich endolymph fills the endolymphatic sac and duct, the saccule and utricle, the membranous semicircular canals, and the cochlear duct or scala media. These structures are interconnected by the smaller utricular duct, saccular duct, and ductus reuniens. The membranous endolymphatic structures are surrounded by the sodium-rich perilymph that fills the periotic spaces within the bony labyrinth.8
The position of the endolymphatic sac along the posterior fossa dura is relatively constant, but its size and the amount of bony covering by the operculum are variable.9 In most patients, 50% of the sac lies outside of the temporal bone, and 50% of the sac is intraosseous. Approximately 10% of sacs are completely extraosseous along the posterior fossa dura.10 The sac can extend posterolaterally to cover the lateral sinus.11 The morphology of the sac is also variable. The distal sac has a smooth open lumen within the dura mater. Its cuboidal epithelium contains light and dark cells.12 The lining of the intermediate portion of the sac shows more complex epithelial folds forming papillae and crypts of tall columnar light and dark cells. Cells of the intraosseous proximal rugose sac are intermediate between the taller, more distal cells and the squamous-to-cuboidal cells of the duct. The duct narrows at its isthmus to 0.1 to 0.2 mm in diameter. Luminal folding and transversely oriented tubules make the endolymphatic sac a more complex structure than it otherwise outwardly appears.13
The normal bony vestibular aqueduct is readily apparent on high-resolution computed tomography (CT) scanning of the temporal bone. It is funnel-shaped or tubular with the width of its external aperture averaging 6 mm.14,15 Radiographic observation of the affected ear in patients with Meniere’s disease showed a filiform narrowing of the external aperture averaging 2.2 mm.14 The amount of narrowing of the external aperture was also shown to be correlated with an increasing percentage of positive electrophysiologic measures in the affected ears of patients with Meniere’s disease.15 Statistically significant differences in the percentage of patients with enlarged summating potential-to-action potential (SP:AP) ratios by transtympanic electrocochleography were seen when correlated with the size of the external aperture of the vestibular aqueduct. An increased SP:AP ratio was noticed in 95% of ears with nonvisible external apertures, 91% when the aperture was less than 5 mm, 58% when the aperture was 5 to 7 mm, and 29% when the aperture was greater than 7 mm.
The endolymphatic duct and sac can be seen on high-resolution fast spin echo magnetic resonance imaging (MRI). The endolymphatic sac and duct were seen on MRI of 20 temporal bones in healthy subjects using strongly T2-weighted sequences and postprocessing software.16 A retrospective review of 42 ears with MRI data that underwent endolymphatic sac surgery correlated surgical findings with the ability to image the endolymphatic sac and duct.17 Surgical findings were classified as normoplastic in 17, atrophic in 14, and invisible in 11. Proton density imaging and T2 sequencing positively identified the endolymphatic duct and sac in 14 patients. The endolymphatic sac and duct were shown by proton density imaging alone in 14; neither proton density imaging nor T2 sequencing showed images in the remaining 14 ears. Findings at surgery showed statistically significant correlation with the ability to identify structures on imaging. Normoplastic surgical anatomy was identified on both imaging modalities; however, atrophic sacs were rarely seen on T2 imaging.
In another study using submillimeter MRI, the endolymphatic ducts were visualized in 29% of patients with Meniere’s disease and in 91% of healthy individuals. Temporal bone measurements between the posterior semicircular canal and the subarachnoid space, and the vestibule and the subarachnoid space were shorter in Meniere’s disease patients than in healthy individuals. It was noted anecdotally that endolymphatic shunt surgery was more effective in the few patients with visualized ducts compared with patients with nonvisualized ducts.18 Currently, the practicality of imaging in Meniere’s disease or for endolymphatic surgery lies primarily in ruling out retrocochlear pathology.
From a surgical perspective, the endolymphatic sac is generally approached through the mastoid bone, and is isolated on the lateral surface of the posterior fossa dura. When performing a suboccipital craniotomy, the sac can often be identified on the posterior petrous aspect of the temporal bone. Discussing the location of the endolymphatic sac, Gibson19 noted that the extraosseous portion is difficult to define surgically, appearing only as a thickened area of dura. He also noted that after splitting the layers of the endolymphatic sac no endolymph is seen, and usually no significant electrophysiologic changes occur. Huang20 attributed higher success in endolymphatic sac surgery to definite identification of the sac, with entry into the true sac lumen, and preservation of the sac anatomy. Amiratti and colleagues21 advocated preserving the integrity of the endolymphatic system, suggesting severe audiovestibular disturbances that may follow sac disturbance; however, our experience is that patients tolerate complete excision of the sac without hearing loss, whether incidental in other cranial base procedures, or intentional for complete endolymphatic sac ablation.
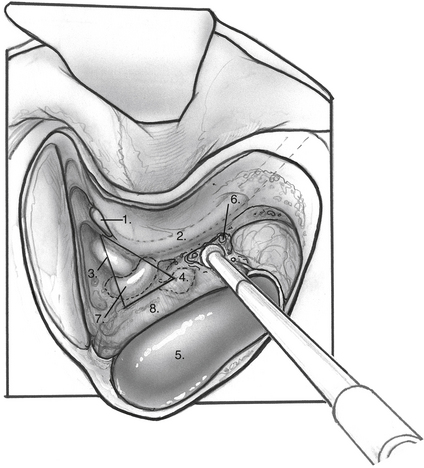
Important topographic landmarks for identifying the endolymphatic sac exist from the transmastoid or posterior fossa approach. The transmastoid extradural landmarks for localization of the endolymphatic sac and for preservation of labyrinthine structures include Donaldson’s line, which is an imaginary line drawn posteriorly through the plane of the horizontal semicircular canal (see Fig. 34-1), and measurements delineating the hard angle. The endolymphatic sac is generally found along the posterior fossa dura inferior to Donaldson’s line. Caution must be used when identifying the sac to avoid damage to the facial nerve and the posterior semicircular canal. Anatomic variants of normal temporal bone anatomy have been associated with Meniere’s disease. An understanding of potentially altered anatomy is important for surgical planning of sac procedures.22 Hypoplasia of the mastoid air-cell system, hypocellularity of periaqueductal cells around the endolymphatic duct and sac, reduction of the aditus ad antrum, and hypoplasia of the facial recess all have been described.
Intradural identification of the endolymphatic sac in relation to anatomic structures of the posterior fossa places the sac 10 to 15 mm lateral to the internal auditory meatus, and 11 to 17 mm posterosuperiorly to the eleventh cranial nerve in the jugular foramen.21 Typically, the thickening of the dura and the bony ledge of the operculum pinpoint the location of the sac.
ENDOLYMPHATIC SAC PHYSIOLOGY
Surgical shunting of the endolymphatic sac was proposed soon after the initial anatomic observations of hydrops in the endolymphatic compartments to alleviate inferred dysfunction.1,23 The presumed longitudinal flow of endolymph from the stria vascularis to the endolymphatic sac and the role of the sac as a primary resorptive organ have long been assumed.24 Radial flow of endolymph has also been shown, however.25 Endolymph is produced by dark cells located largely in the stria vascularis, but also in vestibular ampullae, within the maculae of the saccule and utricle, and along the endolymphatic duct. Maintenance of a potassium-rich endolymph produces the endocochlear potential, a DC voltage gradient, to drive the transduction process important in the detection of sound, motion, and position.26,27 This is a pH-sensitive process and is based on an active transport system in the vestibular dark cells by a sodium–hydrogen ion exchange system.27,28 Local production concentrated within strial dark cells and radial movement of endolymph with local chemical exchange throughout its course maintain a chemical balance and gradient that promote physiologic endolymphatic function, and may promote a slow linear flow toward the sac.25
Other theories of endolymphatic fluid homeostasis exist. Salt29 stated that direct measurements of the dispersal of markers in endolymph fail to support dynamic flow theories, and suggested that, in the normal state, there is negligible flow. The ionic component of endolymph is maintained through single cell transport of ions. This local control theory is overridden when endolymph volume is abnormally high or low, with the endolymphatic sac acting as a regulator of bidirectional flow in response to volume needs. The endolymphatic sac functions as the master volume regulator by numerous observed characteristics. In contrast to endolymph throughout the inner ear, a gradient exists along the duct leaving the electrolyte state in the endolymphatic sac high in sodium and low in potassium.30 An active equilibration of ions creates an osmotic potential that may influence the transepithelial flow of fluids. Higher concentrations of Na+,K+-ATPase are seen in the endolymphatic sac, but diminish proximally along the endolymphatic duct.31
Several other findings suggest an active role of the endolymphatic sac on endolymph fluid homeostasis.32–34 Aquaporin 2, vasopressin type 2 receptor, and transient receptor potential channel vanilloid (TRPCV), subfamily type 1 and 4, were found in the epithelial lining of the endolymphatic sac, but not in other extracellular tissues, although TRPCV 1 was seen in the surrounding vasculature. Similar findings are seen within the kidneys, suggesting a parallel role in fluid filtration and resorption.32 A unique protein, saccin, secreted by the endolymphatic sac, acts within the kidney as an endogenous inhibitor of sodium reabsorption. Intracellular morphology of the endolymphatic sac chief cells possesses organelles capable of endocrine function, and cellular ultrastructure consistent with merocrine activity also is observed.33,34
Biochemical and cellular findings within the endolymphatic sac support its functional role in phagocytic, immune, and allergic responses of the inner ear.35–39 Volume may also be regulated by the functional mechanical entity of an extracellular matrix of interstitial cells that support the endolymphatic duct, and take part in the control of inner ear fluid dynamics and endolymph resorption.40 As new techniques are developed to detect and monitor minute fluid volumes and changes, and to evaluate the chemical composition and cellular characteristics of the endolymphatic sac, a better understanding of the physiologic role and pathophysiologic state of the endolymphatic system in Meniere’s disease will be achieved.26,41
ENDOLYMPHATIC HYDROPS: PATHOPHYSIOLOGY
It was not until the histopathologic observation of Hallpike and Cairns in 193842 that a proposed malfunction of the endolymphatic system was correlated with the clinical syndrome. These authors showed dilated endolymphatic spaces in temporal bone specimens from two patients with the clinical symptoms of Meniere’s disease who died after neurotomy of CN VIII. These findings showed end organ changes of the inner ear in patients with hearing and balance symptoms. The hydropic state of the inner ear has been confirmed in other temporal bone studies and described as the primary pathologic correlate of Meniere’s disease.43–45
The underlying cause of the hydropic state is at present unknown, although many theories exist. Hydrops is seen more often in the cochlea and saccule, structures derived from the later developing pars inferior.43 Congenital insults or developmental aberrations later in the course of embryogenesis could presumptively account for this difference. A familial connection is seen in the history of 20% of patients clinically diagnosed with Meniere’s disease.44 This connection, in consideration of the embryologic and anatomic findings associated with Meniere’s disease, suggests a multifactorial predisposition to developing endolymphatic hydrops. Whether this precondition is genetic or related to shared environmental factors or insults is yet to be determined.
The pathophysiologic state of the endolymphatic system has been partially modeled in mice by experimental destruction and obstruction of the sac or duct in attempts to pinpoint the underlying mechanism of the hydropic condition.46,47 Although these experiments were able to reproduce hydrops and audiometric findings similar to Meniere’s disease, vestibular dysfunction or vertigo was noticed only after placing the animals in a head-down position theoretically by inducing additional pressure within inner ear fluids.48
The predominant theories that could explain the symptom complex of Meniere’s disease are based on the observed pathologic and induced experimental evidence of hydrops. The various temporal bone findings are summarized succinctly by Costa and associates,49 and include ruptures of the membranous labyrinth, fistulas of the membranous labyrinth, collapse of the membranous labyrinth, obstruction of longitudinal flow, vestibular fibrosis, sensory lesions, and neural lesions. Schuknecht50 proposed the rupture theory. He reasoned that distention of the endolymphatic space with eventual membrane rupture could cross-contaminate perilymphatic spaces and toxify delicate sensory hair cells with the potassium-rich endolymph. In the distention theory, Paparella51 described decompensation of radial flow as the perilymphatic spaces ebb, leading to largely longitudinal flow along the hydropic membranous pathway with the saccule acting as a reservoir for the excess endolymph. As the dilated saccule encroaches on the confines of the vestibule, mechanical interference of cochlear and vestibular function occurs by inhibition of traveling waves and physical contact with the crista ampullaris.
The drainage theory, as presented by Gibson and Arenberg,10 suggests that obstruction of a narrowed endolymphatic duct divests the sac of endolymph. The endolymphatic sac responds by secreting glycoproteins and saccin. Glycoproteins act osmotically by “pulling” endolymph toward the sac, and saccin stimulates secretion of endolymph from dark cells that distend the endolymphatic spaces “pushing” against the obstruction toward the sac. The obstructing debris ultimately and suddenly passes, and the resultant rapid flow of endolymph purportedly brings on an acute vertiginous episode. Gibson and Arenberg suggested that patients with Meniere’s disease with larger vestibular aqueducts could experience resolution of auditory symptoms as in Lermoyez’s syndrome after clearance of the obstructing debris. Patients with Meniere’s disease have been shown to have widening of the vestibular aqueduct aperture, but, although enticing to establish a mechanism of pathology, patients with Lermoyez’s syndrome have not been shown to have wider vestibular aqueducts than other patients with Meniere’s disease. Gibson and Arenberg also theorized that Tumarkin crises could be the effect of a membrane rupture in the overdistended endolymphatic space.
MENIERE’S DISEASE
Epidemiology
Arenberg and colleagues52 have suggested that incidence and prevalence estimations reported in Meniere’s disease are inaccurately low by not recognizing the early or atypical cases, or cases misdiagnosed by lengthy remissions drawing out the episodic nature. The definition of Meniere’s disease may alter prevalence and incidence numbers. The 1995 AAOHNS Committee on Hearing and Equilibrium recognized that the 1985 diagnostic criteria for Meniere’s disease were rigid to the point of precluding patients who were most likely Meniere’s cases. Current criteria are listed at the beginning of this chapter.2 These gradations may alter the epidemiologic accounting of Meniere’s disease because they allow for inclusion of patients who may be early in the course of their disease, and patients who may have milder symptoms of the disease. Several retrospective reviews have shown the prevalence of Meniere’s disease to be 10 to 20 per 100,000 in various populations around the world.49 Using 1995 committee criteria for diagnosis, a more recent study in the Finnish population showed 43 cases per 100,000 population, and an annual incidence of 4.3 per 100,000.53
Costa and associates49 described in detail the epidemiology of Meniere’s disease. It generally manifests in the fifth decade of life. The incidence in childhood is thought to be 1% to 7% of all Meniere’s cases.54 Of 14 children diagnosed with definite Meniere’s disease, 5 were shown to have secondary disease manifesting 5 to 11 years after a history of Haemophilus influenzae meningitis, mumps, temporal bone fracture, and congenital and embryopathic complications.55 Nine of the 14 children had idiopathic disease. These 14 children represented 1% of the combined Meniere’s population of four neurotologic clinics. There is a slight female preponderance. In women with definite Meniere’s disease who were pregnant, a clear decline in symptoms was associated with delivery.49 No socioeconomic, occupational, or racial effect has been consistently shown, although there are statistically increased numbers in married individuals and anxious individuals, and decreased numbers in obese individuals.
Diagnosis
Electrophysiologic tests, including electrocochleography, cochlear microphonics, and vestibular evoked myogenic potentials, have been used as adjuncts in diagnosis, and to monitor the efficacy of treatment in Meniere’s disease.44,56 In 2002, Ge and Shea57 reported a 10-year experience using transtympanic electrocochleography. Transtympanic electrocochleography was performed in 2421 ears of 2140 patients with Meniere’s disease. These authors concluded that electrocochleography is a reliable test to detect the presence of endolymphatic hydrops in Meniere’s disease using parameters of an enlarged SP:AP ratio greater than 0.4, a broadened action potential waveform (>3 ms), and a prolonged action potential latency (>0.2 ms). Combined click and tone burst responses yielded an enlarged SP:AP ratio in 81.7%, and a prolonged AP latency was found in 62.2% of ears with Meniere’s disease. An enlarged SP:AP ratio significantly correlated with stage and duration of disease. The SP:AP ratio was found to be elevated in 71% of stage 1 Meniere’s disease, 82% of stage 2, 85% of stage 3, and 90% of stage 4. The SP:AP ratio was elevated in 43% of patients during their first year of diagnosis and in 100% of patients with the disease for more than 30 years.
Cochlear microphonics were also used to assess the presence of hair cell survival, and were found to be present in 69% of ears with pure tone averages greater than 40 dB. It has been suggested that large cochlear microphonics in patients with Meniere’s disease indicate hearing loss resulting from altered cochlear mechanics, whereas severe hearing loss with small cochlear microphonics represents a hearing deficit resulting from hair cell loss.58 Electrocochleography has been shown to have a low sensitivity (57%), but is specific for endolymphatic hydrops (94%).44 In patients with an elevated SP:AP ratio in the immediate preoperative period, a statistically significant intraoperative reduction of the SP:AP ratio has been reported after endolymphatic sac incision and drainage.59
Vestibular evoked myogenic potential is used to assess the vestibulocollic or sacculocollic reflex. This test selectively assesses saccular function and integrity of the inferior vestibular nerve. It is being explored in Meniere’s disease for its potential in identifying endolymphatic or saccular hydrops.60 Vestibular evoked myogenic potential testing may aid in identification of active Meniere’s disease,60 and may help identify ears more prone to develop contralateral Meniere’s disease.62,63 Vestibular evoked myogenic potential may also offer information complementary to electronystagmography,64,65 and provide a way to measure severe saccular dysfunction, a finding associated with Tumarkin crisis.66 These tests show promising diagnostic potential. Further testing experience and validation are necessary.
Treatment
Medical Treatment
Dietary measures include reduction or restriction of caffeine, alcohol, and salt. Medical therapy is aimed at affecting fluid dynamics through diuretic therapy. Although many nutritional, vitamin, and medical therapies have been advocated for the treatment of Meniere’s disease, the combination diuretic Dyazide (triamterene and hydrochlorothiazide) is currently the only medical treatment that has shown in a randomized, placebo-controlled trial a statistical decrease in the vestibular symptoms of Meniere’s disease.70 Breakthrough episodes are managed symptomatically with a choice of several options of different classes of vestibulosuppressants. In-depth medical treatment of Meniere’s disease is addressed elsewhere. The work-up and treatment of other processes that secondarily produce Meniere’s syndrome, alone or in conjunction with standard medical treatment of endolymphatic hydrops, are usually successful at alleviating symptoms.



