Chapter 4 Malignancies of the Temporal Bone—Radical Temporal Bone Resection
Primary malignancies of the temporal bone were first recognized in the late 18th century and histologically first confirmed in the 1850s. These lesions are uncommon, with only 250 cases having been reported in the English literature by 1974.1 The overall prevalence in the general population is 6 cases per 1 million.2 Because of their infrequent occurrence, these tumors are often misdiagnosed and treated as chronic external otitis or chronic mastoiditis. They are usually discovered at a later stage, when more radical treatment is required. The infrequent occurrence of the disease poses a challenging obstacle to any attempt at a clinical study regarding treatment.
DIAGNOSTIC EVALUATION
Cerebral blood flow evaluation is indicated when involvement of the ICA is present. Patency of the anterior and posterior communicating arteries on angiography is an inadequate evaluation for collateral flow. Our current method of preoperative carotid artery testing is described.3 A 30-minute temporary balloon occlusion of the ICA allows identification of patients who would most likely tolerate carotid artery sacrifice. Transfemoral introduction of a nondetachable intravascular balloon, inflated in the ICA, is performed in the patient while sensory, motor, and higher cortical functions are assessed.
SURGICAL PROCEDURE
Incisions vary according to the extent of the tumor (Fig. 4-1). For lesions contained within the temporal bone, a C-shaped incision extending from the temporal fossa postauricularly into the neck is used. A blind-sac closure of the EAC helps contain the specimen. When tumor invasion of the conchal cartilage or periauricular skin is suspected, an appropriate skin island is incorporated into the overall design. The EAC skin is sutured shut to avoid tumor spillage. The outline of the incisions should preserve the blood supply to the remaining auricle. The anterior and posterior skin flaps are elevated (Fig. 4-2A). The superficial temporal fat pad is elevated with the anterior skin flap in a subperiosteal plane over the zygomatic arch. The superficial temporal and middle temporal arteries are ligated.
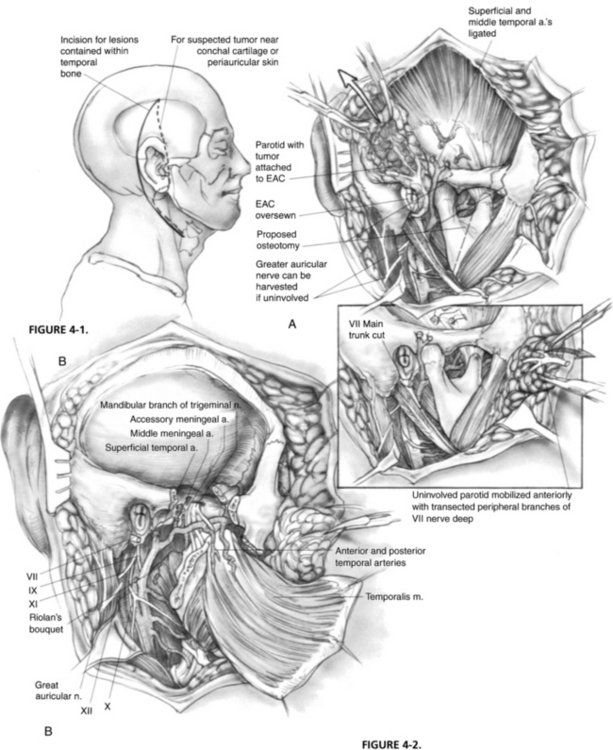
The masseter is detached from the zygomatic arch, allowing exposure of the zygoma and mandible. Zygomatic and mandibular osteotomies (see Fig. 4-2A) can then be performed. The meniscus of the temporomandibular joint is separated from the glenoid fossa, and the chorda tympani nerve emerging from the petrotympanic fissure is divided. The stylomandibular and sphenomandibular ligaments are divided and allow removal of the mandibular segment (Fig. 4-2B). The temporalis muscle is elevated in a subperiosteal fashion and reflected inferiorly. The temporalis muscle must be separated from the lateral pterygoid muscle, and care should be taken not to injure the deep temporal arteries supplying blood to the temporalis muscle. The lateral and medial pterygoid muscles are resected either en bloc with the specimen or separately, depending on tumor invasion.
The stylohyoid, stylopharyngeus, and styloglossus muscles (Riolan’s bouquet) are detached from the styloid process, which is then rongeured away. The branches of the external carotid artery are dissected in the infratemporal fossa. The anterior tympanic and deep auricular branches of the internal maxillary artery are often divided before identification, and may require bipolar coagulation. The internal maxillary artery is preserved up to the branches of the deep temporal artery. When the internal maxillary artery must be sacrificed, brisk backflow from the anterior stump indicates that the temporalis muscle may derive its blood supply from reversed flow via the pterygoid system. If brisk backflow is not observed, the temporalis muscle cannot be relied on to reconstruct the surgical defect, and microvascular free flap options must be considered. The cartilaginous eustachian tube is divided, and the anterior end is sutured closed to prevent postoperative cerebrospinal fluid rhinorrhea (Fig. 4-3A).
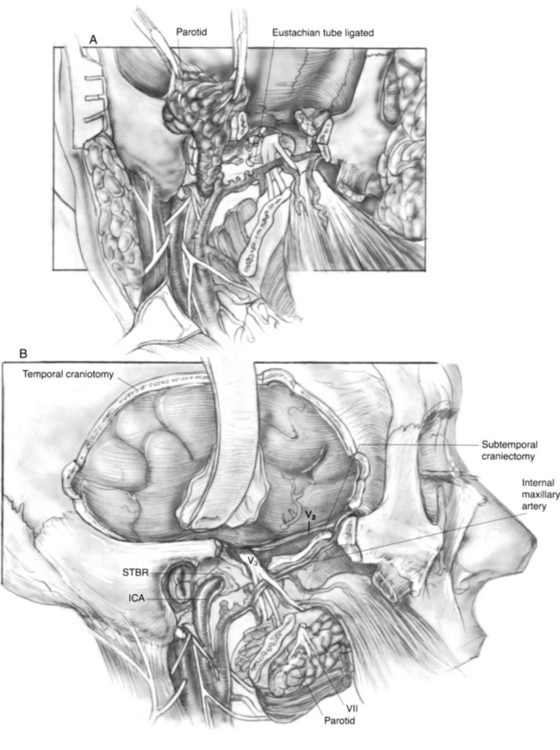
The ICA is dissected toward the carotid canal, and care is taken not to injure CN IX, which crosses its anterior surface. Kerrison rongeurs are used to uncover the vertical and horizontal petrous segments of the carotid artery (Fig. 4-3B). Occasionally, bleeding from the pericarotid venous plexus requires bipolar coagulation. The caroticotympanic artery is also divided when the petrous carotid artery is separated from the specimen. The extent of petrous carotid mobilization depends on whether STBR or TTBR is performed. When STBR is performed, the vertical petrous carotid artery is mobilized from the carotid foramen and canal. When TTBR is performed, the vertical and horizontal petrous carotid artery is mobilized out of the carotid canal to the foramen ovale.
A temporal craniectomy is performed, and the intracranial portion of the middle meningeal vessels is coagulated (see Fig. 4-3B). The patient is hyperventilated to keep the Pco2 at 25 mm Hg for adequate brain relaxation. Mannitol and furosemide can improve brain relaxation. Subtemporal dural elevation proceeds in a posteroanterior direction. The greater superficial petrosal nerve and accompanying petrosal artery are coagulated and divided to lessen traction on the geniculate ganglion. The lesser petrosal nerve and superior tympanic artery are similarly divided. Subtemporal dural elevation proceeds as far medially as possible to expose the superior petrosal sinus. When carcinomatous involvement of the middle fossa dura is suspected, an intradural approach keeps the involved dura attached to the specimen.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


