Intermediate Uveitis
Dmitry Pyatetsky
Howard H. Tessler
Intermediate uveitis is a chronic condition in which the signs of inflammation are most pronounced in the vitreous. The term refers to the anatomic location of the inflammatory reaction, the middle of the eye, not to a particular disease entity. The anterior segment, retina, and the optic disc may also be involved. The amount of inflammation in other areas is less severe than the vitreous reaction, which is the predominant feature in intermediate uveitis. The inflammation may be secondary to an underlying systemic disorder, such as sarcoidosis or multiple sclerosis, or it may be isolated to the eye and idiopathic.
In the past several terms have been coined to describe intermediate uveitis, such as cyclitis,1 chronic cyclitis,2 vitritis,3 peripheral uveitis,4,5 basal uveoretinitis,6 and pars planitis.7 In 1987, the term “intermediate uveitis” was adopted to bring uniformity to the description of this clinical entity,8 and was further clarified by the Standardization of Uveitis Nomenclature Working Group in 2005.114 Unfortunately, any modern account of intermediate uveitis must include the following disclaimer: Much confusion has arisen from the previously nonstandardized terminology applied to this group of diseases and many reported statistics and comments about the disease etiology, presentation, and course should be taken with a grain of salt. The 2005 standardization of uveitis nomenclature will likely make careful study of intermediate uveitis more feasible.
Intermediate uveitis has been reported to have an incidence of 0.3 per 100,000 and a prevalence of 1.4 per 100,000.9 Patients with intermediate uveitis typically report blurred vision and floaters. They seldom mention pain and photophobia, in contrast to patients with anterior uveitis. In intermediate uveitis, the anterior segment either is clear or shows low-grade inflammation. The conjunctiva is typically white and uninflamed. The cornea may show endothelial dusting due to deposition of fibrin and a few inflammatory cells. Typically, keratic precipitates are absent or minimal. The anterior chamber may be quiet or show mild to moderate cellular reaction and flare. The iris is not involved, although focal posterior synechiae form in some cases. Children with intermediate uveitis may have a more significant anterior segment reaction and may complain of photosensitivity. The vitreous is the site where the inflammation is most heavily concentrated, and it shows varying amount of cells, fibrin, and cellular debris depending on the severity. In some cases (e.g., pars planitis), inflammatory and fibroglial exudates, called snowbanks, may form in the inferior vitreous base, over the peripheral retina, and the pars plana. The retina is often unremarkable, although retinal periphlebitis (i.e., sheathing), optic disc edema, and macular edema are present in some cases.
In most patients, intermediate uveitis is solely an ocular disorder. However, in a few patients, intermediate uveitis is part of a systemic disease. Systemic diseases that may present with intermediate uveitis include sarcoidosis, multiple sclerosis (MS), Lyme disease, Whipple’s disease, HTLV infection, Inflammatory Bowel Diseases and intraocular lymphoma.9,116
Pars Planitis
Pars planitis is the most common form of intermediate uveitis. The distinguishing feature of pars planitis is the presence of inflammatory and fibroglial exudates in the inferior vitreous base over the inferior peripheral retina, ora serrata, and pars plana. The term pars planitis is reserved for idiopathic disease only—intermediate uveitis with snowbanks secondary to sarcoidosis, multiple sclerosis, and so forth is not referred to as pars planitis.
Epidemiology
About 4% to 15% patients referred for uveitis have pars planitis.10,11,12,13,14,15,16,17 Pars planitis usually affects children and young adults.18 It seldom develops before age 5 or after age 30. Most cases develop in the teens and early 20s. Some reports10,18 show no racial predilection, but others11,13,16 show that whites are affected more frequently than blacks. There is no predilection toward either sex.10,18 Pars planitis is bilateral about 71% to 75% of the time.4,13,19 Familial cases of pars planitis and intermediate uveitis have been reported.20,21,22,23,24
Symptoms
The onset of symptoms is very gradual in pars planitis. The most common symptoms of pars planitis are blurred vision and floaters. Symptoms may be present for months to years before the patient seeks medical attention. At times, patients with pars planitis are asymptomatic, and the diagnosis is made on a routine ophthalmic examination. Patients with pars planitis rarely report redness, pain, or photophobia.
Signs
Externally, the eyes of patients with pars planitis do not appear inflamed. The conjunctiva and sclera are usually white without injection. The cornea is usually clear and appears uninvolved. In long-standing cases, band keratopathy may develop, most frequently in patients who developed pars planitis in childhood or their early teens.11,13 In some cases of pars planitis, small keratic precipitates and fibrin may be present on the corneal endothelium. Large keratic precipitates are not characteristic of pars planitis. The anterior chamber may be clear or show only mild cells and flare. The amount of inflammation in the anterior chamber is typically mild, rarely exceeding grade 2+.25 The iris may be uninvolved or show only one or two localized posterior synechiae. Extensive iris synechiae, seclusion of pupil, and iris nodules are not typically seen in pars planitis. The lens may be clear or may appear cataractous. In pars planitis, posterior subcapsular cataract is most frequently seen, and it may be the result of ocular inflammation or the chronic use of corticosteroids.
In pars planitis, the inflammatory signs are greatest in the vitreous cavity. The vitreous gel is syneretic and shows varying amount of fibrin, cells, and strands. The hallmark of pars planitis is the presence of exudates in the inferior vitreous base (Fig. 43.1). In early stages these exudates may appear as discontinuous yellow-white clumps (fluff balls or snowballs). However, as the disease progresses, these exudates may increase in number and size until they coalesce to form a fluffy white exudate over the inferior peripheral retina and pars plana. Later, the exudate organizes into a smooth white fibrous-appearing band. This membrane has been termed a snow bank because of its resemblance to white fluffy snow. The term pars planitis is reserved for intermediate uveitis in which snow bank is present. The amount of vitreous inflammation is usually symmetric in both eyes. However, in some cases, a prominent snow bank may be present in one eye but only a few fluff balls in the other. Scleral indentation is often required to visualize the snowbank (Fig. 43.2).7,26
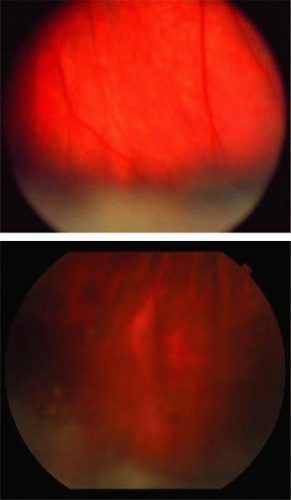 FIGURE 43.1 A: Pars planitis. White exudate in the deep vitreous over the inferior peripheral retinal and pars plana is typical of pars planitis. In the early stages, the exudate is white and fluffy and suspended in the vitreous, resembling cumulus clouds. In the late stages, the exudate becomes continuous and fibrous, resembling a snowbank. B: Pars planitis. Note vitreous snowballs adjacent to the snow bank. |
 FIGURE 43.2 Pars planitis. Scleral depression elevating the snowbank into view with indirect ophthalmoscopy. |
Retinal venules (periphlebitis), cystoid macular edema, and optic disc edema (Figs. 43.3 and 43.4). In cases of chronic cystoid macular edema, epiretinal membrane formation often occurs (Fig. 43.5).4,13,27
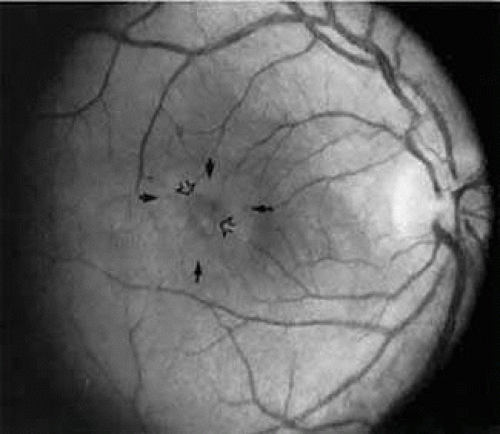 FIGURE 43.3 Pars planitis. Cystoid macular edema. Black arrows point to a halo of edema surrounding the macula. Open arrows point to cysts in the macula. |
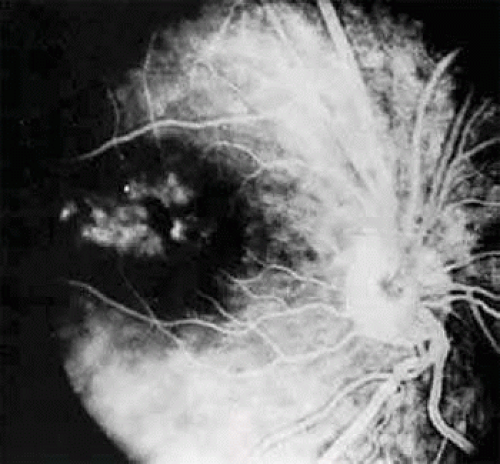 FIGURE 43.4 Pars planitis. Fluorescein angiogram showing a petaloid staining pattern in the macula. |
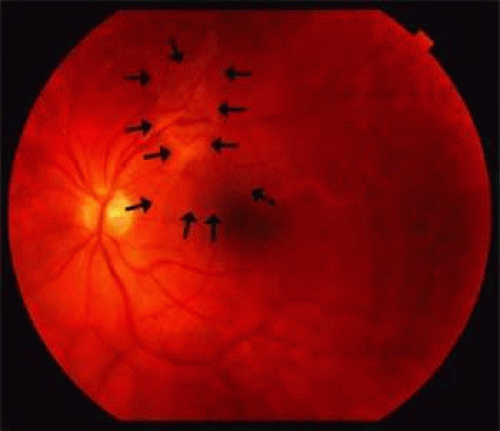 FIGURE 43.5 Pars Planitis. Color fundus photograph showing an epiretinal membrane, outlined by arrows. |
Fluorescein Angiography, Vitreous Fluorophotometry, and Optical Coherence Tomography
In pars planitis, fluorescein angiography shows diffuse leakage from the retinal venules and capillaries, without any predilection for the inferior retinal vasculature (Figs. 43.6 and 43.7).28 Similarly, vitreous fluorophotometry in patients with pars planitis also shows no predilection for vascular leakage in the inferior peripheral retina.29 These findings suggest that snow bank is most likely a gravitational sequela from ocular inflammation. The inferior peripheral retina is not the source of inflammation in pars planitis. Pars planitis is not a localized inflammatory response of the inferior retina. Optical coherence tomography (OCT) is useful in visualizing the cystoid macular edema and epiretinal membranes that frequently complicate the disease (Figs. 43.8 and 43.9).
 FIGURE 43.6 Pars planitis. Fluorescein angiogram showing diffuse venous and capillary leakage. |
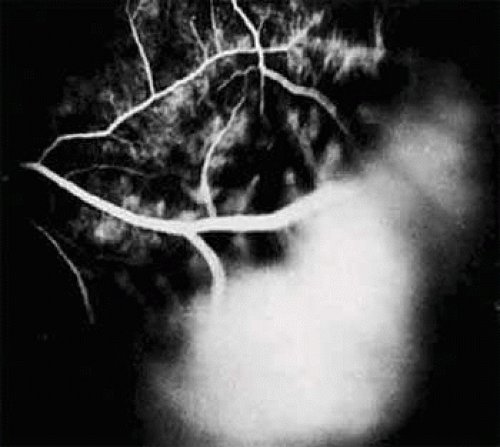 FIGURE 43.7 Pars planitis. Fluorescein angiogram of pars plana membrane showing diffuse leakage indicating neovascularization. |
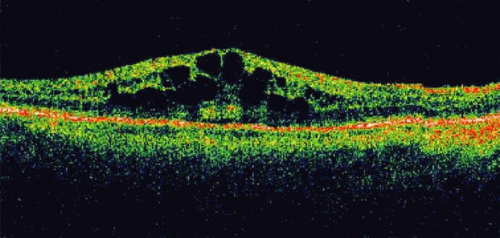 FIGURE 43.8 Pars planitis. Optical coherence tomograph reveals cystoid macular edema in the posterior pole. |
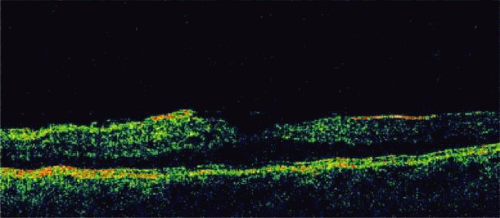 FIGURE 43.9 Pars Planitis. Optical coherence tomograph reveals an epiretinal membrane in the macula. |
Clinical Course
The clinical course is marked by chronic low-grade inflammation, which may be punctuated by episodes of exacerbation. In a study of 100 patients, Smith et al.13 divided the clinical course of their patients into three categories. The first group (10% of the eyes) followed a benign self-limiting course of gradual clinical improvement without episodes of exacerbation. The second group (59% of the eyes) followed a smoldering, prolonged course without episodes of exacerbation. The third group (31% of the eyes) followed a smoldering and prolonged course with episodes of exacerbation. About 4% of their cases underwent spontaneous remission.
In pars planitis, the severity of the disease has no correlation to the duration of disease. Cases that are unilateral at first presentation may become bilateral later. Pars planitis is bilateral about 71% to 75% of the time.4,13,19 Often there is asymmetry in severity between eyes. In our experience, unilateral cases tend to have a milder course than bilateral cases. The presence of snow bank may indicate more severe and prolonged vitreous inflammation and often is associated with cystoid macular edema.30 In the past it was thought that most cases of pars planitis enter remission before age 40. Today, it appears that the jury on this question is still out. A recent study by de Boer et al.115 supports the classic notion, but is not consistent with the conclusions of some of the previous reports.72 Many uveitis specialists recognize that the diagnosis of pars planitis represents a spectrum of disease severities. The disease may “burn out” in some cases, but in others a more severe course with significant visual disability may ensue.
Histopathology
Few pathologic reports of pars planitis have been described. Most cases are long-standing and chronic. Early changes have not been reported.
Histologically, the snow bank is composed of glial elements, type VI collagen, and laminin.31 Extensive fibroglial proliferation and fibrous astrocytic-like cells have been seen in the vitreous base.32,33 These cells can synthesize basement membranes and produce large-diameter collagen fibrils.32,33 Fibrovascular tissue may be present in the snowbank and consists of well-differentiated capillaries that probably originate from the peripheral retina.33
The vitreous is usually collapsed and detached posteriorly from the retina. Multinucleated giant cells and epithelioid cells have been demonstrated in the vitreous snowballs.34 There is cellular proliferation from the retina and hyperplasia of the nonpigmented ciliary epithelium.34 The choroid usually does not show significant inflammation.31,34
Lymphocytic cuffing and mural infiltration of the retinal venules can be present, consistent with periphlebitis and phlebitis, respectively.33 The retinal arterioles are spared.33 These lymphocytes are mostly T-helper cells.31 Histologic changes consistent with clinical cystoid macular edema may be present in the fovea.33
Etiology and Pathogenesis
The cause of pars planitis is unknown, and its pathogenesis remains unclear. As described in previous sections, inflammation in pars planitis is most prominent in the vitreous and seems to begin clinically in the inferior vitreous base, with formation of fluff balls during the early stages of disease. This suggests that the pathogenesis of pars planitis begins in the vitreous base. Snow banks, resembling those in pars planitis, have been produced in monkeys35 receiving multiple intravitreal injections of hyaluronic acid and in rabbits36 receiving intravitreal injections of crystalline egg albumin. Further, a predominance of T-helper cells has been demonstrated in the snowbank glial tissue in one eye.31 These findings suggest that deposition of foreign antigens in the vitreous may lead to pars planitis.
The predilection for the inferior vitreous base to form snow bank is perhaps due to the gravitational settling of cells and debris from the inflamed vitreous in pars planitis. However, the formation of snow bank may also be due to an increased number of cells in the inferior vitreous.37
Elevated serum levels of IgD have been reported in patients with pars planitis.38 Humoral and cell-mediated immunity against the photoreceptor S-antigen have been demonstrated in some patients with pars planitis.39,40,41 The presence of retinal immunity may represent an epiphenomenon that occurs after the initial insult to the retina.39 A similar epiphenomenon has been observed in patients with diabetic retinopathy; they also show elevated serum levels of anti-S-antigen antibody after undergoing retinal photocoagulation.42 However, even if not primary, retinal autoimmunity may exacerbate the inflammation in pars planitis. Class II antigen has been demonstrated on the vascular endothelium in eyes with pars planitis, indicating that the vascular endothelium may also be part of the immunologic process.31
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


