Infectious Retinitis
Igor Kozak
William R. Freeman
Retinitis refers to diseases that produce inflammation of the retina. This chapter deals primarily with infectious causes of retinitis and the differential diagnosis of these diseases. Each disease is described in detail including clinical presentations, pathophysiology, and diagnostic techniques. Therapeutic interventions including chemotherapy of each entity, as well as surgical interventions, are also discussed. Infectious causes of retinitis include diseases caused by viruses such as herpes simplex virus (HSV), varicella zoster virus (VZV), and cytomegalovirus (CMV). Less common viral agents that may cause disease of the posterior segment include subacute sclerosing panencephalitis (SSPE), West Nile virus (WNV) and Rift Valley fever virus (RVFV). Bacterial and fungal infections of the retina (endogenous endophthalmitis) are discussed elsewhere in this text; however, they are briefly discussed here because they are causes of retinitis.
Acute Retinal Necrosis Syndrome
The acute retinal necrosis (ARN) syndrome is classically described as a fulminant retinitis with moderate to severe uveitis that usually occurs in otherwise healthy patients. Mild forms of the disease1 and occurrence of ARN in immunocompromised hosts 2,3 have been reported. Since the first description by Urayama and colleagues in 1971,4 ARN has been shown to be due to viral infection of the retina. Specific antiviral therapy may improve the visual outcome as compared with the outcome in older reports.
Since 1971, various terms have been used to describe ARN including Kirisawa’s uveitis,4 necrotizing vaso-occlusive retinitis,5 peripheral retinal necrosis,6 and bilateral ARN.7 Behçet’s disease, a noninfectious retinal vasculitis with systemic involvement of mucous membranes including recurrent oral and genital ulcers, has an extended course with numerous exacerbations and remissions and for these reasons is a distinct entity. ARN classically consists of uveitis and peripheral necrotizing retinitis often with secondary retinal vasculitis and optic nerve inflammation. In Behçet’s disease, retinal vasculitis is the primary cause of retinal disease.
The ARN patient typically presents with progressive visual blurring in one or both eyes occurring over several weeks. These patients often are initially treated with corticosteroids, anti-toxoplasmosis drugs, and other medications before arriving at the correct diagnosis. Examination reveals a prominent anterior uveitis that may be granulomatous or non-granulomatous (Fig. 1). Inflammatory signs may be prominent and cause severe pain (Fig. 2). The uveitis may be diffuse and so severe that it causes proptosis. These signs, and the diffuse vitreitis that makes the view of the retina difficult, may contribute to the high degree of delay and/or misdiagnosis that occurs in the early stages of the disease. Significant vitreous cellular infiltration is seen in the presence of retinitis that is manifested by opacification of the retina, often most prominently in the periphery. Posterior pole involvement may include retinitis, as well as inflammation of the optic nerve head. Optic neuropathy might be the first sign of ARN with subsequent development of other retinal manifestations.8 Ultrasonography and computed tomography (CT) might be helpful in cases of ARN associated with optic nerve edema revealing enlargement of the optic nerve sheath.9 Even in ARN patients who are not immunocompromised and who have no clinical evidence of encephalitis, magnetic resonance imaging of selected cases has shown lesions of the lateral geniculate, optic tracts, and chiasma, which suggests that the virus spreads through the central nervous system (CNS) by axoplasmic transport from the retinal ganglion cells.10 A secondary retinal vasculitis is common, often accompanied by a mild number of retinal hemorrhages. Days to weeks after onset of the infection, the discrete peripheral lesions typically coalesce into a white or yellow ring of infected retina, and the associated vasculature is obliterated (Fig. 3). Necrotic retina desquamates into the vitreous resulting in vitreous sheets.3,6 Eventually, most untreated eyes can be expected to develop retinal detachment resulting from development of multiple full-thickness retinal breaks accompanied by traction or exudation.11 Giant retinal pigment epithelial tears have also been reported.12
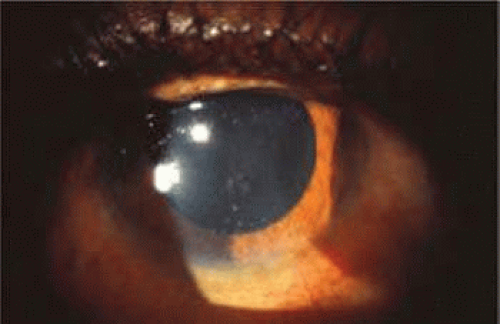 Fig. 1. Granulomatous keratic precipitates seen in a patient with acute retinal necrosis syndrome. |
 Fig. 2. Severe inflammation in a patient with acute retinal necrosis causing chemosis of the conjunctiva and lid edema. |
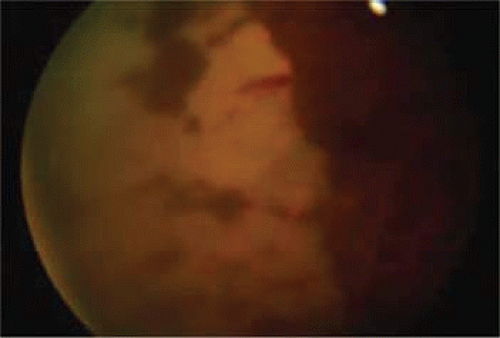 Fig. 3. Confluent peripheral retinitis seen in acute retinal necrosis. The perivascular lucent areas with some evidence of hemorrhage are typical of this disease. |
In 1994, the American Uveitis Society published its criteria for the diagnosis of ARN. These criteria (classified into mandatory and supporting categories) were dependent on the clinical signs of the disease, and no laboratory or investigative results were included in these criteria.
The required clinical criteria include the following:
One or more foci of retinal necrosis with discrete borders, located in the peripheral retina.
Rapid progression of the disease in the absence of therapy.
Circumferential spread of the disease.
Evidence of occlusive vasculopathy and arteriolar involvement.
A prominent inflammatory reaction in the vitreous and anterior chamber.
The supporting clinical criteria include the following:
Optic neuropathy or atrophy.
Scleritis.
Pain.13
A human leukocyte antigen (HLA) association between ARN and HLA-DQw7, HLA-Bw62 and DR4 has recently been demonstrated. An immunogenetic predisposition may explain why only some individuals who have been exposed to these ubiquitous herpesviruses develop the disease.14 In Japanese patients, the risk of ARN infection increases with HLA-Aw33, B44, and DRw6.15 No predilection for sex, race, or age has been identified. ARN has been reported in patients ranging from 9 to 89 years old.16 Before knowledge of the viral etiology, there was documentation of a variety of antecedent systemic viral or bacterial infections that were suspected to have a causal role.7,17,18 A history of prior exposure to herpesviruses, particularly VZV, may be elicited in some but not all cases. In some cases, unilateral ARN may be followed by involvement of the contralateral eye up to 10 years after the first episode. Recurrences in the initially involved eye may occur but they are rare.16,19,20,21
Both herpes simplex virus type 1 and herpes simplex virus type 2 (HSV-1, HSV-2) may cause ARN.20,21,22 In a single report, CMV particles were identified in and cultured from the retina of an enucleated eye of a non-immunosuppressed patient suffering from bilateral ARN.23 VZV has been reported most frequently as the viral etiologic agent of ARN.2,3,24,25,26,27 We have demonstrated herpesvirus family viral particles in endoretinal biopsy specimens taken from patients in the active stage of the disease who showed an enormous viral load (Fig. 4). These studies, combined with the failure of many enucleated eyes with ARN to demonstrate evidence of viral particles, indicate that the virus is present only in the active stages of the disease and that a gliotic retina will not demonstrate the etiologic agent.28
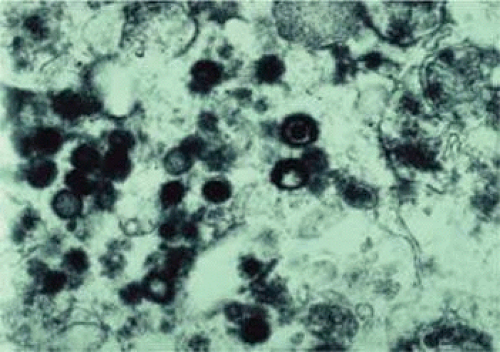 Fig. 4. An electron micrograph showing abundant herpesvirus particles from a retinal biopsy taken at the active stage of acute retinal necrosis. |
Some cases of ARN follow or precede zoster dermatitis,2,29,30 leading some to conclude that the retina is infected secondary to neural spread from sensory ganglia in the CNS. However, most patients with herpes zoster ophthalmicus do not develop ARN,3 suggesting that transmission of virus to the retina associated with trigeminal nerve reactivation is uncommon. The site of latency and mechanism of viral infection remain unknown.
The polymerase chain reaction (PCR) is a highly sensitive, specific, and rapid means of detecting small amounts of viral deoxyribonucleic acid (DNA) in intraocular fluid samples. Recently, PCR-based assays have been used as aids for the diagnosis of ARN and the determination of the specific virus causing the syndrome.31,32,33 Ganatra and associates conducted an interesting study about the viral causes of ARN using PCR-based assay of various viruses DNA in aqueous and vitreous. They found that VZV or HSV-1 cause ARN in patients older than 25 years, whereas HSV-2 causes ARN in patients younger than 25 years. In this study, VZV DNA was recovered in 15 out of 30 eyes. HSV-2 DNA was detected in six eyes, and HSV-1 was detected in seven eyes. CMV DNA was detected in only one eye, and no virus DNA was recovered in one eye in which the sample was taken after 6 weeks of acyclovir therapy. Also, no sample was positive for DNA from more than one virus.34
Light microscopic examination of these retinas reveals full-thickness necrosis and loss of the retinal architecture.25,30,35 Within the necrotic retina, macrophages, plasma cells, and other inflammatory cells are found in addition to cells containing eosinophilic inclusions. There is a sharp demarcation between affected and non-affected retina, suggesting cell-to-cell transmission of the virus. Arteritis manifests as endothelial cell swelling with occlusion of the vessel lumen, infiltration of the sub-endothelium with plasma cells, and inflammatory cell thrombi. When healing occurs, a thin glial scar replaces the necrotic neural elements. Herpesvirus capsids may be observed in electron microscopic specimens of actively infected retinal tissue but are not seen once healing has occurred and glial scar tissue replaces the necrotic retina.28,30
Given the evidence that most cases of ARN are due to VZV or HSV, acyclovir therapy is recommended.35,36,37,38 Acyclovir is taken up by infected cells and phosphorylated into a proactive form by virally encoded thymidine kinase. Subsequent phosphorylation by cell coded kinases results in formation of the active triphosphate form of acyclovir that inhibits viral replication by blocking DNA polymerase activity. Hung and coworkers39 demonstrated that oral administration of acyclovir (400 mg five times per day) to normal volunteers can produce mean plasma levels of 8.7 μm and mean aqueous levels of 3.3 μm.
Some strains of herpesviruses known to have caused ARN are inhibited only by acyclovir concentrations greater than the achievable aqueous concentrations after oral administration (400 mg five times per day) of acyclovir. Intravenous therapy with 1500 mg/m2/day in three divided doses achieves peak plasma levels of 30 to 40 μm without significant toxicity to the patient and is, therefore, the recommended regimen. Aqueous acyclovir levels of 8.7 to 11.2 μm are achievable using intravenous acyclovir (1500 mg/m2/day), and these levels are sufficient to treat most cases of ARN. Pro-drugs of acyclovir are available that yield serum levels after oral administration that are as high as serum levels after intravenous infusions such as valacyclovir 1000mg three times a day.
The duration of therapy is generally dependent on the response of the infection. Ten days is probably sufficient because progression of retinal lesions usually stops within several days of initiation of intravenous therapy.39 In cases that are deemed unresponsive to acyclovir, cultures of a retinal biopsy specimen may provide evidence of the presence of an acyclovir-resistant strain of VZV, HSV, or CMV, which is resistant to acyclovir but sensitive to ganciclovir.23,40
The use of steroid and/or anticoagulant therapy remains controversial. Optic nerve infiltration with inflammatory cells and occlusions of arteriolar vessels may result in optic nerve ischemia, which leads some to treat patients with oral prednisone at doses up to 120 mg daily.35,40 Some have suggested that sudden visual loss out of proportion to retinal findings is suggestive of optic nerve ischemia caused by mechanical compression and/or edema and have advocated optic nerve sheath decompression in selected cases.9 To avoid vaso-occlusion and because of a report of altered platelet aggregation in this disease,41 some investigators have advocated the use of aspirin (500 mg/day), heparin, sodium warfarin (Coumadin), or other anti-platelet agents as adjunct therapy to hopefully diminish the vascular complications of ARN.35 Finally, high-dose steroid administration, for example, methylprednisolone 250 mg intravenously every 6 hours, may diminish the generalized ocular inflammatory response resulting in less serum exudation and hence a decrease in the concentration of chemotactic agents in the vitreous that are responsible for causing migration of pigment epithelium cells. This would have the theoretic advantage of decreasing the chances for developing proliferative vitreoretinopathy. Controlled studies evaluating the efficacy of steroids in preventing proliferative vitreoretinopathy or comparing acyclovir versus acyclovir with anti-platelet therapy in preventing ARN-related optic neuropathy are lacking, and the evidence that corticosteroid use worsens the course of active herpetic corneal disease must be remembered.
A variable number of eyes, up to 75%, develop retinal detachments (Fig. 5). Prophylactic laser for demarcating the areas of active retinitis from normal retina has been advocated to create chorioretinal adhesions that prevent retinal detachments around sites of retinal break formation (which usually occur at the zone between affected and healthy retina). Han and associates42 reported five cases treated with prophylactic laserpexy in addition to antiviral, steroid, and anti-platelet therapy. After 15 months of follow-up, no retinal detachments were noted. Sternberg and coworkers43 described a 75% decrease in the rate of retinal detachment using prophylactic photocoagulation. Some have advocated the creation of a “new ora serrata” by applying confluent rows of laser burns posterior to the areas of retinitis. However, if traction forces from vitreous organization, epiretinal membrane (ERM) formation, or proliferative vitreoretinopathy develop as they commonly do, the contractile forces will be able to overcome any increased chorioretinal adhesion created by the laserpexy. McDonald and associates44 reported failure of prophylactic peripheral laserpexy to prevent retinal detachment in ARN patients. In addition, many cases of ARN result in a severe vitritis, limiting the view for a planned laserpexy (Fig. 6). Therefore, vitrectomy with endolaser and concomitant encircling of the eye with a scleral buckle to reduce traction may be required in some patients.45,46 Decisions relating to the need for scleral buckling to support retinal breaks and the use of silicone oil or long-acting gases to repair retinal detachments should be made by an experienced vitreoretinal surgeon.40,47 Selection of cases to undergo operation should be made with consideration given to optic nerve function, visual potential, and medical control of retinitis.
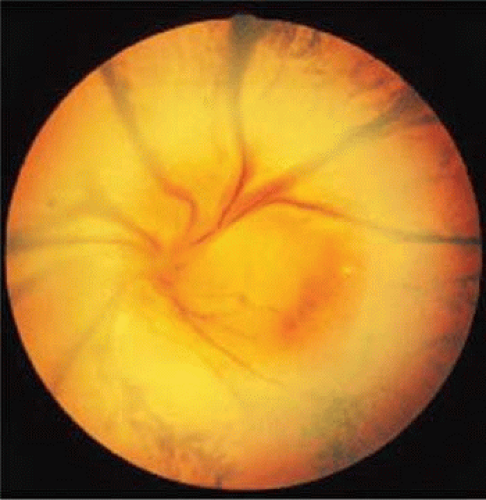 Fig. 5. A patient with funnel-shaped retinal detachment and proliferative vitreoretinopathy complicating acute retinal necrosis syndrome. |
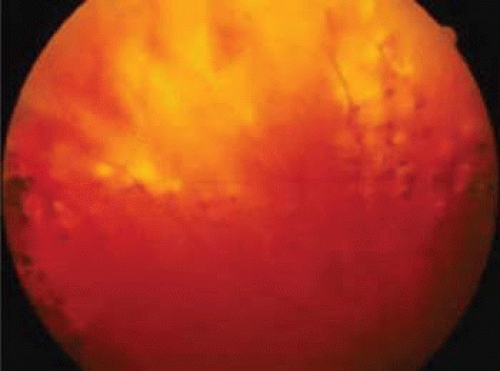 Fig. 6. Failure of prophylactic laser treatment to stop the progression of a retinal detachment associated with retinal necrosis resulting from viral retinitis with progression of the detachment beyond the line of laser demarcation. |
The ocular complications of ARN are myriad. During the active infection, uveitis is a prominent feature. Secondary glaucoma may develop because of inflammatory debris in the trabecular meshwork. Posterior synechiae may form with resulting pupillary block and occlusion of the angle by forward movement of the peripheral iris. Pupillary membranes and cataract development have been described. Optic nerve atrophy has been noted and may be due to loss of ganglion cell bodies in the retina or direct invasion of the nerve head by the virus with subsequent inflammation and swelling. Iris neovascularization and neovascular glaucoma may occur. Disc and retinal neovascularization with subsequent vitreous hemorrhage have also been noted.16,48 Finally, a blind painful eye may develop, necessitating retrobulbar alcohol injection or enucleation.
Recently, a mild variant of ARN was described in Japan that may represent a self-limited form of the disease.1 We recently reported a series of cases in which the retinitis was limited and in which the visual prognosis was significantly better than is commonly reported.49 These reports would seem to indicate that ARN manifested by limited peripheral involvement may portend a better prognosis, particularly when treated early with appropriate antiviral therapy.
Perhaps the most significant complication of a unilateral case of ARN is subsequent involvement of the fellow eye. Sternberg and associates16 reported the cases of six patients, four of whom went on to bilateral involvement anywhere from 3 weeks to 22 months following diagnosis of ARN in the first eye. Matsuo and associates1 described the onset of ARN in the fellow eye after a 3-year interval. In one case, a 10-year quiescent interval was reported between the onset of ARN in the first eye and involvement of the fellow eye. Culbertson and coworkers25 reported that 36% of their patients eventually had bilateral ARN syndrome. Interestingly, two independent laboratories studying the electrophysiologic aspects of ARN have found that the electroretinograms of unaffected eyes may be abnormal.50 The prognostic significance for eventual contralateral involvement has not been investigated. Prolonged oral acyclovir or valacyclovir therapy probably reduces the risk of fellow eye involvement.
In summary, ARN is primarily seen in otherwise healthy persons but has been reported in immunocompromised hosts as well; in HIV patients it is termed progressive outer retinal necrosis. Patients typically present with progressive visual blurring and may carry numerous prior misdiagnoses. The infection causes a severe retinitis, vitreitis, and uveitis that may result in numerous secondary ocular complications. Although the viral infection is treatable, preferably with intravenously administered acyclovir, eventual retinal detachment occurs in most cases. Hence, surgical interventions to preserve vision are usually warranted. Prophylactic laserpexy to wall off the area of infection and prevent total retinal detachment may be helpful if adequate visualization of the area to be treated is possible. However, for patients in whom adequate visualization of the retina is not possible or if retinal detachment is identified, pars plana vitrectomy with endolaser and possible scleral buckling should be considered. Most importantly, frequent dilated retinal examination of both eyes must be performed during the convalescent period and for several years thereafter.
Cytomegalovirus Retinitis
CMV is a ubiquitous, species-specific DNA-containing herpesvirus. Epidemiologic studies examining the temporal development of CMV antibody seropositivity in the general population reveal that approximately 1% of newborns contract CMV while in utero, and a larger group acquires the virus at birth through an infected birth canal or in early infancy. Thereafter a steady increase in the prevalence of antibody-positive individuals occurs from adolescence into adulthood. It is postulated that contact with CMV-contaminated urine, saliva, and semen is the major mode of transmission, because it has been demonstrated that crowding, sexual contact, and exposure of children to day care centers can result in conversion to antibody positivity.51 Eventually up to 90% of the general population develops antibody to CMV, suggesting widespread exposure to this agent.52
Despite a high prevalence of antibody positivity in the population, clinical ocular disease secondary to CMV infection in adults is rare or nonexistent in the absence of immunosuppression resulting from malignancies, autoimmune disease, acquired immunodeficiency syndrome (AIDS), or therapeutic intervention. Before 1970, only a small number of CMV retinitis cases had been described. In 1971, deVenecia53 elegantly documented the first histologically proved case of CMV retinitis. Since then, the increase in chemotherapeutic abilities and the emergence of AIDS as a leading cause of morbidity and mortality has caused the number of cases of CMV-related ocular disease to increase drastically.
Groups of patients at higher risk for contracting CMV-related disease include neonates born to CMV-infected mothers and immunosuppressed adults. In neonates, de novo infection with CMV during the last two trimesters leads to cytomegalic inclusion disease. Cytomegalic inclusion disease manifests as microcephaly, psychomotor retardation, hepatosplenomegaly, thrombocytopenia, and other systemic abnormalities in a small-for-gestational-age infant. In adults, the etiology and spectrum of CMV-related disease are less well defined. Secondary reactivation of primary latent infection has been documented and postulated to be a major source of CMV-related disease. The site of latency, however, has yet to be identified. De novo infection with a second strain of CMV has also been documented.54 Heterophil-negative mononucleosis manifested as lymphadenopathy, malaise, and atypical lymphocytosis is the most well-described CMV-related disease in otherwise healthy adolescents and is a relatively benign illness without retinal involvement. In contrast, in immunosuppressed persons and neonates, CMV-associated disease causes significant morbidity and mortality. For the ophthalmologist, CMV retinitis presents a formidable albeit treatable cause of blindness.
CMV retinitis was first described in 1959 by Foerster.55 Since then it has become obvious that a characteristic retinitis occurs in neonates with cytomegalic inclusion disease and in CMV-infected immunocompromised persons. In transplant patients, CMV retinitis may be the initial clinical manifestation of life-threatening viremia and indicates the need for immediate aggressive lifesaving intervention. For AIDS patients, CMV retinitis often is documented after other opportunistic infections, typically when the CD4 lymphocyte count falls below 100; however, CMV retinitis as the initial manifestation of AIDS has been well described.56 Early retinitis may present with small white lesions that may be confused with cotton-wool spots. However, unlike cotton-wool spots, which are seen in the nerve fiber layer, CMV retinitis is seen as granular whitening located deeper in the retina (Figs. 7, 8, and 9). These same areas of retinitis are often associated with intraretinal hemorrhage and vasculitis of nearby retinal vessels. Although the lesions of CMV retinitis are located in the posterior pole more often than in ARN, peripheral retinitis is not uncommon.57 The lesions can be multifocal as well, pointing out the need for thorough examination of the entire peripheral retina. The vitreous may be relatively quiet allowing excellent visualization of the underlying retina; however, significant vitreitis may occur. The pars plana is relatively spared,53,58 although it is unclear why this should be so, because the pars plana epithelium and the retina share a common neuroectodermal origin. On occasion, stellate keratic precipitates with cell and flare can be observed on the cornea and in the anterior chamber. In some cases a prominent retinal vasculitis may be seen posterior to the area of retinitis (Fig. 10).
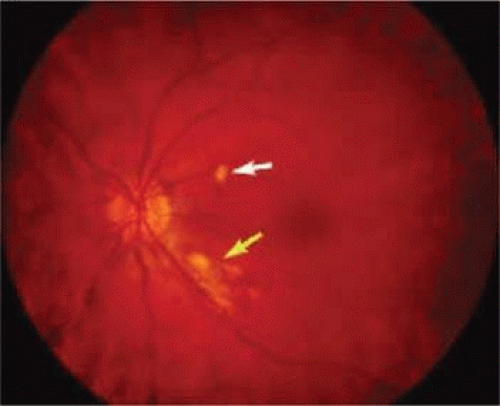 Fig. 7. A patient with cotton-wool spot (white arrow) and early cytomegalovirus (CMV) retinitis (yellow arrow). Note the granular pattern of the CMV lesion. |
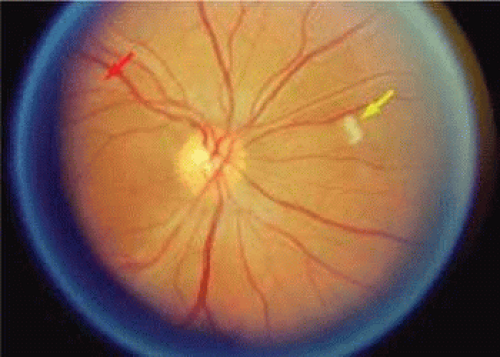 Fig. 8. A patient with cytomegalovirus (CMV) lesion superotemporal to the optic nerve (red arrow) and cotton-wool lesion (yellow arrow) superonasal to the optic nerve. The CMV lesion is granular and deep. |
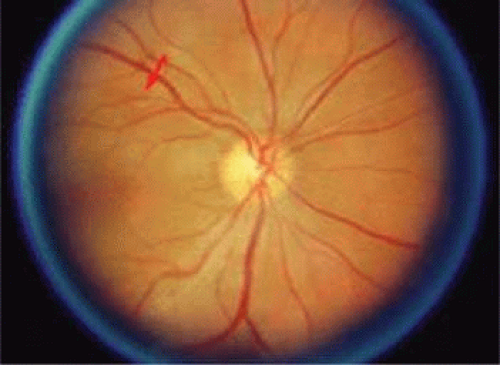 Fig. 9. Same patient as in Figure 8 seen 1 month later shows resolution of cotton-wool patch and some enlargement of the area of infectious cytomegalovirus retinitis (red arrow). |
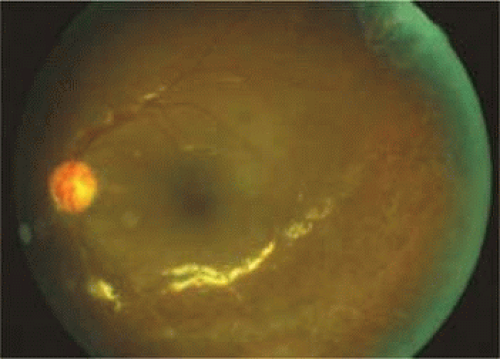 Fig. 10. A patient with vasculitis secondary to cytomegalovirus (CMV) retinitis. The vasculitis is typically along the veins draining the lesion. |
CMV retinitis occurs in 15% to 40% of AIDS patients57,60,61,62 and, in contrast to the noninfectious lesions of AIDS, demands aggressive treatment to prevent severe visual loss.59,62,63 Patients with active CMV disease may present with systemic symptoms of fever, arthralgia, leukopenia, pneumonitis, retinitis, or hepatitis. Blood cultures and urine specimens are usually positive for CMV. CMV infects the retina, as well as the CNS, the reticuloendothelial system, kidneys, adrenals, lungs, and gastrointestinal system.62,64 CMV retinitis is often the presenting sign of systemic CMV infection, and all patients should have a thorough systemic evaluation performed, including “buffy coat” culture of the blood and possible evaluation of bone marrow aspirates and cerebrospinal fluid. Thus, screening for CMV retinitis is very important in AIDS patients. Urine is culture positive for CMV in 50% of homosexual men and in most AIDS patients, and, thus, urine culture may not be of diagnostic value. Serology in AIDS patients is notoriously unreliable, and it is unusual to document rising CMV titers.59,62,64 CD4 cell count might be used as a practical test for screening because the risk of CMV retinitis increases at CD4 cell count below 50/mm3.65 Techniques for detection of CMV DNA based on PCR in ocular fluids have become more popular. One PCR-based study for the detection of CMV DNA in vitreous samples had an estimated sensitivity of 95% in detecting untreated CMV retinitis and a sensitivity of 48% in detecting CMV retinitis that had been treated with systemic ganciclovir or foscarnet or both.66 A variant of the Amsler grid has been used as a screen for central CMV retinitis within a 22-degree radius (3 disc diameters) of the fovea. This technique may detect up to two thirds of the cases of CMV.67 Recently, we reported the use of a new technique, entoptic perimetry, as a screening test in patients with CMV retinitis. This technique employs patient visualization of moving particles on a computer monitor. This test has a very high sensitivity and specificity (more than 90%) in detecting CMV retinitis within the central 30-degrees radius of fixation.68
The clinical presentation of CMV retinitis in AIDS is similar in many respects to CMV retinitis found in iatrogenically immunosuppressed patients and in infants with cytomegalic inclusion disease.56,69,70 Correlation of the clinical and typical pathologic findings at autopsy has been demonstrated.71 Specifically, it is known that CMV is a neurotropic virus with a tendency to infect neural tissues and the retina. Necrosis of the retina in AIDS-associated CMV retinitis is typical, with pathognomonic cytomegaly and only a few inflammatory cells in the lesions. Choroidal involvement is rare; however, retinal vascular endothelium may be infected. These lesions may also appear as noncontiguous patches rather than the contiguous, spreading lesion more commonly seen. Antigens to CMV have been found by immunofluorescence, immunoperoxidase staining, and DNA hybridization techniques (Fig. 11).64,72
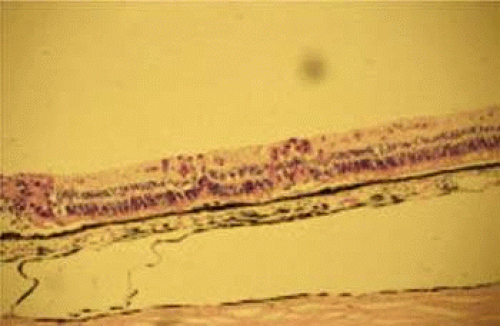 Fig. 11. Histopathologic specimen showing immunohistochemical staining (red areas) in retinal cells infected with cytomegalovirus (CMV). This is in an area approximately 1 mm posterior to an area of confluent retinal destruction seen at the left of the figure. The small lesions probably correspond to the white dots that are seen just beyond the area of confluent CMV retinitis clinically. These areas of cytomegalic changes are associated with retinal edema and opacification. They are approximately 200 to 300 μm and would be visible as small white areas of opacification. |
Progression of the retinitis generally occurs with a leading edge of active retinitis and a trailing region of thin gliotic retina. This pattern indicates cell to cell transmission of the virus. CMV is a slowly progressive, necrotizing retinitis that may affect the posterior pole, the peripheral retina, or both and may be unilateral or bilateral. Involved areas appear as white intraretinal lesions; areas of infiltrate; and often necrosis, along the vascular arcades in the posterior pole. In addition, prominent retinal hemorrhages are often seen within the necrotic area or along its leading edge (Figs. 12 and 13). Peripherally, CMV retinitis tends to have a less intense white appearance, with areas of granular, white retinitis that may or may not demonstrate associated retinal hemorrhage (Fig. 14). As the retinitis progresses, an area of atrophic, avascular retina may remain with underlying retinal pigment epithelial atrophy and/or hyperplasia (Fig. 15).56,57,59,61 Peripheral CMV retinitis may be the most common form of CMV retinitis seen. Patients may initially complain only of floaters with or without a visual field deficit.56 Wide-angle fundus photography and fluorescein angiography may be of benefit when the diagnosis is uncertain. These techniques may be used to document progression of retinitis, and fluorescein leakage in areas of retinitis may be helpful in confirming the diagnosis. Although peripheral CMV retinitis may not pose an immediate threat to vision, initiation of treatment should be seriously considered because several investigators have shown that untreated CMV retinitis is inexorably progressive and becomes bilateral in virtually all untreated patients.58,59,64,73,74,75 Occasionally, noncontiguous areas of new retinitis may be seen. As healing takes place, a thin glial scar replaces the necrotic retinal tissue. The transition from infected to non-infected retina is usually sharply demarcated and well seen during the active phase of the disease. When healing takes place, the transition zone is between a glial scar and normal retina and may be difficult to visualize. Clinically, the pigment epithelium tends to develop a characteristic spiculated granular appearance directly under the residual glial scar. The retina in the immediately adjacent uninvolved areas is thick in comparison to the glial scar, thus, differing light reflexes occur with indirect ophthalmoscopy. Using the pigment epithelium changes and light reflexes, one can define the extent of prior retinal involvement. More importantly, defining the edge of prior involvement allows one to predict with great accuracy the sites of new involvement, allowing for more effective monitoring of therapeutic efforts to control the infection. Other manifestations of CMV retinitis include retinal edema, attenuated vessels, perivascular sheathing, and exudative retinal detachment.76 In addition, vitreitis and anterior uveitis are often seen,69 and optic atrophy may occur as a late manifestation secondary to widespread retinal destruction. CMV may be demonstrated in vitreous biopsy specimens in these patients.64 The yield may be higher in the presence of marked vitreitis because CMV is a cell-associated virus. Other causes of retinitis, including herpes simplex retinitis,77,78 toxoplasmosis,79 Candida, Behçet’s disease, syphilis, ARN,7,28,80 and SSPE81 can usually be distinguished from CMV on clinical grounds. Cotton-wool spots are nonspecific and may be seen in diabetes mellitus, hypertension, severe anemia, systemic lupus erythematosus, dermatomyositis, and leukemia,82,83 as well as AIDS. It may be difficult to distinguish a small focus of non-hemorrhagic CMV retinitis from a cotton-wool spot corresponding to the area of peripapillary optic nerve fiber layer that was destroyed (Figs. 16 and 17). In eyes in which CMV infection initially involves the optic nerve head, the visual acuity may be normal early; however, the visual prognosis may be poor because these eyes often go on to loss of light perception (see Fig. 13). When retinitis is in close proximity to the optic nerve head or macula, a serous retinal detachment may be seen that will resolve with therapy.
 Fig. 12. A patient with a relatively nonhemorrhagic variant of cytomegalovirus retinitis. Note at the center of the lesion (oldest area of infection) the retina is atrophic and pigmentary changes can be seen. Peripheral to it the retina is edematous, and this is the area of active infection. |
 Fig. 13. A patient with hemorrhagic variant of cytomegalovirus (CMV) retinitis that affected the posterior pole and optic nerve. Hemorrhages are most often intraretinal, and white areas correspond histologically to intracellular and extracellular edema and necrosis of the neurosensory retina. Eyes with extensive optic nerve involvement secondary to retinal involvement may still retain good central vision unless the papillomacular bundle is involved. When retinitis starts in the optic nerve head, the prognosis for vision is poor. |
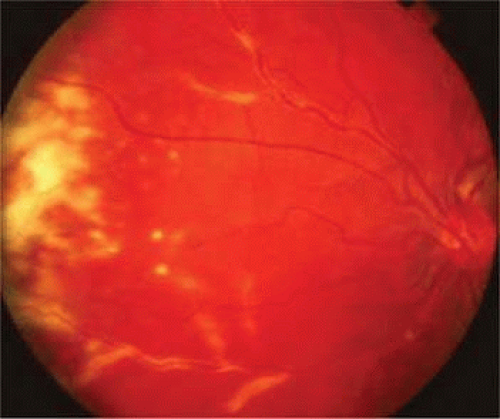 Fig. 14. Cytomegalovirus retinitis in the periphery may have minimal hemorrhagic components. |
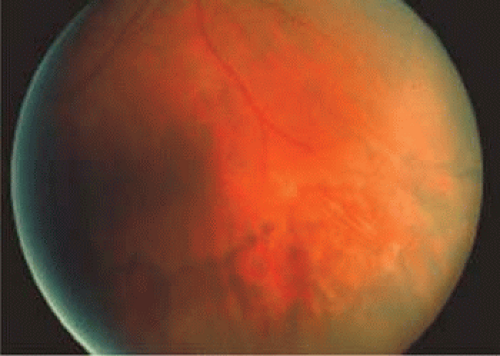 Fig. 15. Area of healed cytomegalovirus retinitis showing characteristic pigmentary changes. In the area of retinal necrosis, the retinal pigment epithelium (RPE) is also thinned and bare choroidal vessels are visible. |
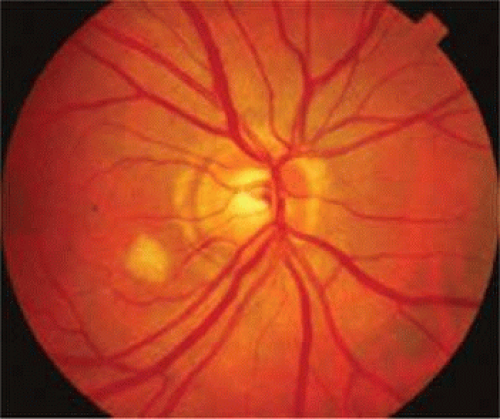 Fig. 16. A patient with cotton-wool spots near the optic nerve. The nerve fiber layer swelling obscures the details of retinal vessels. |
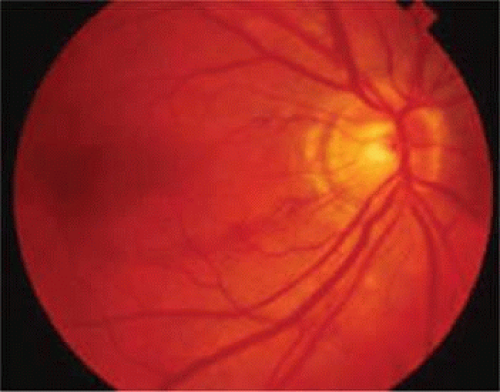 Fig. 17. Same patient (see Fig. 16) 6 weeks later showing disappearance of the cotton-wool spot. A residual nerve fiber layer defect is seen as are some small areas of residual vascular changes and hemorrhage. |
Histologic findings in CMV retinitis include the presence of typical cytomegalic cells with prominent intranuclear inclusions resulting in a pathognomonic “owl’s eye” appearance.56 Closer examination of the owl’s eye of infected cells reveals a dense central nuclear inclusion body with clearing of nucleoplasm immediately around the inclusion (Fig. 18). Inflammation, manifesting as mononuclear cell infiltration, is usually scant, and the choroid is spared. Endothelial cells of retinal vessels may be infected with CMV.53,58
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


