CHAPTER 157 Implantable Hearing Aids
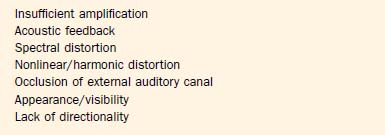
Hearing aids are the principal means of auditory rehabilitation for patients with sensorineural hearing loss (SNHL). Hearing aids may also play a role in the management of patients with conductive hearing losses (CHL), particularly losses that result from pathologies that are not amenable to medical and surgical treatment. Improvements in signal processing capabilities and increasing miniaturization of hearing aids have increased their acceptance among patients. Hearing aids remain a “tough sell” to many patients who could potentially benefit from them, however, owing to lack of sufficient perceived benefit, expense, complications of external auditory canal occlusion, and cosmetic concerns. In a restaurant, multiple competing sound sources, such as conversations, the ventilation system, and music, can undermine the ability to detect and resolve speech cues. Many other patients simply cannot wear a hearing aid because of problems with the external auditory canal, chronic infections, or extreme discomfort. Although newer hearing aid technologies have tried to address many of these difficulties, many patients still find that hearing aids fall short in meeting expectations in a variety of situations (Box 157-1). Partly for these reasons, less than one in eight eligible adults actually use a hearing aid.1
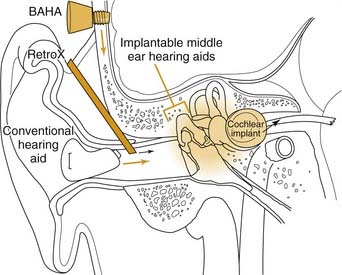
These inherent limitations in hearing aids, combined with the social stigma of their use, have led to the development of implantable hearing aids (Figs. 157-1 and 157-2). Implantable hearing aids offer patients with hearing loss several potential advantages over conventional hearing aids, including increased gain and dynamic range, reduced feedback, reduced maintenance, improved appearance, and freedom from ear canal occlusion. These potential benefits must be weighed against the possible downsides of their use, including the risk of surgical implantation, difficulty of maintenance, and increased initial device cost (Table 157-1). Complicating this risk-benefit calculation is the uncertain future of corporations marketing and supporting various implantable hearing aids. Before discussing each of the implantable hearing aids currently available or in development, it is important to review in more detail why there is a desire for their implementation in the first place.
Limitations of Auditory Rehabilitation Using Traditional Hearing Aids
Physical Factors
Insufficient Gain
For patients with severe to profound hearing loss, sound amplification (or gain) is a primary concern. For a patient with air-conduction thresholds of 80 dB hearing level (HL) to perceive quiet sounds at a normal threshold of 0 dB HL, a hearing aid must amplify sound intensity by 80 dB, generating a 10,000-fold increase in sound pressure wave amplitude and a 100,000,000-fold increase in sound power intensity.2 This represents the limit of existing traditional hearing aids. The maximum amplification at 1 kHz for a behind-the-ear (BTE) Phonak SuperFront PPCL4 power digital hearing aid is about 75 to 82 dB.3 Gain generally scales with hearing aid size, so that cosmetically less obtrusive hearing aids offer less gain. The maximum gains for digital in-the-ear (ITE), in-the-canal (ITC), and completely-in-canal (CIC) hearing aids currently are about 55 to 65 dB, 45 to 55 dB, and 35 to 50 dB.3
Poor Appearance
Many patients reject hearing aids because of the social stigma of being seen as old or infirm. Eight percent of hearing aid candidates wearing the less noticeable ITC hearing aids listed poor cosmetic appearance as a major contributing factor in their decision not to use a hearing aid.4 Hearing aids are difficult to conceal in patients who are balding or who wear their hair short. Miniaturization of electronics continues to improve hearing aids in this regard, and CIC hearing aids are essentially invisible to the casual observer. Miniaturization comes at the cost of lower gain, more feedback, and higher cost, however. Ultimately, battery size becomes the limiting factor, with smaller batteries costing more and requiring more frequent replacement.
Poor Transduction Efficiency
Loss of energy because of impedance mismatching and transduction losses is another inherent drawback of conventional hearing aids. The mechanical impedance (change in pressure for a given displacement flow) of the air-filled external auditory canal differs from that of the fluid-filled cochlea. Without a middle ear mechanism, most of the acoustic energy striking the stapes footplate reflects back into the air. When the tympanic membrane and ossicular chain are functioning normally, they act as an impedance-matching transformer by virtue of the relative areas of the tympanic membrane and stapes footplate, and by the lever action of the ossicular chain.5 The relatively large-displacement, low-pressure movements of air against the tympanic membrane are transduced to the relatively small-displacement, high-pressure movements of the footplate. Except for bone-conducting hearing aids, all traditional hearing aids use a speaker to output an (amplified) acoustic wave into the air of the external auditory canal. When this middle ear apparatus is malfunctioning, as occurs in otosclerosis, tympanic membrane perforation, or a canal wall down mastoidectomy, traditional hearing aids must overcome the impedance mismatch. The result is reduced effective gain, increased distortion, or both.
Human Factors
Recruitment and Compression of Dynamic Range
A primary source of frustration of patients with SNHL is reduced speech intelligibility. The common complaint, “I can hear, but I cannot understand,” underscores this point. This problem relates to abnormal frequency resolution and aberrant patterns of growth in loudness, each of which reduces speech intelligibility in challenging listening conditions such as noisy surroundings.6,7
SNHL also imposes severe constraints on the dynamic range of perceived sound. For normal listeners, the dynamic range from sensing soft sounds to the loudest tolerable noise is more than 100 dB. Within this wide dynamic range of hearing lies an approximately 35-dB dynamic range of conversational speech. In contrast, the dynamic range of patients with SNHL is often narrowed by an increase in the threshold of audibility and a lowering of the ceiling of tolerance to high-intensity sounds. This compaction of dynamic range leads to “recruitment,” an abnormal growth in loudness as sound intensity increases.8,9 What sounds normal for someone with normal hearing may be too soft for someone with recruitment, whereas what is too loud for someone with normal hearing is also too loud for a patient with recruitment. In effect, there is a much narrower range of sound intensity that a patient with recruitment can tolerate. Further adding to the difficulty, recruitment is observed in frequencies that are most impaired, in the high frequencies, which also carry crucial information for speech understanding.
Recruitment remains one of the principal challenges of hearing aid rehabilitation, and is responsible for a common phenomenon most clinicians dealing with hearing loss have witnessed or experienced: At average speaking levels, an individual with recruitment may ask a speaker to talk more loudly, yet with even a slight increase in intensity the speech becomes intolerably loud, and the speaker is told not to shout. Although many hearing aids can be programmed to prevent sound from amplifying into a range that is uncomfortable, even the most advanced aids cannot fully replicate the complex, nonlinear response patterns of a healthy cochlea.9
Disordered Perception of Pitch and Sound Localization
All of the aforementioned factors play a role to various degrees in patients, and combine to increase the noncompliance rate in hearing aid users. For most patients, these are the principal reasons why hearing aids are unacceptable.10 With all these challenges concerning conventional hearing aids, it is not surprising that many hearing aid users feel frustrated when hearing aids fail to perform to expectations.
Promise of Implantable Hearing Aids
It is widely accepted that implantable hearing aids should provide distinct advantages over conventional hearing aids, including better cosmetics, improved fidelity, broader frequency response, less distortion, reduction or elimination of feedback, and better speech understanding, without reducing residual hearing, limiting patient activities, or predisposing patients to infection.11,12 In other words, implantable hearing aids should be at least as good as, and preferably better than, the best available noninvasive method of hearing rehabilitation: binaural amplification with the best available aid.13
Although significant strides have been made in many of these areas, implantable hearing aids have yet to deliver on all these features. There also remain questions regarding candidacy for implantation and willingness of patients to accept the costs and surgical risks. As noted by Junker and colleagues,14 the number of patients in a fairly typical population of hearing-impaired individuals who would be considered realistic candidates is limited, on the order of 0.09%. The market for implantable hearing aids may not be sufficiently large to support the current array of device manufacturers. The 2002 financial failing of Symphonix Corp., the first company to gain U.S. Food and Drug Administration (FDA) approval and market their implantable middle ear hearing aid in the United States, strongly underscores this point, as do the subsequent withdrawal of the Soundtec and TICA devices described subsequently in the review of technologies.
Middle Ear Implants
Basic Design Features
Transducer Design
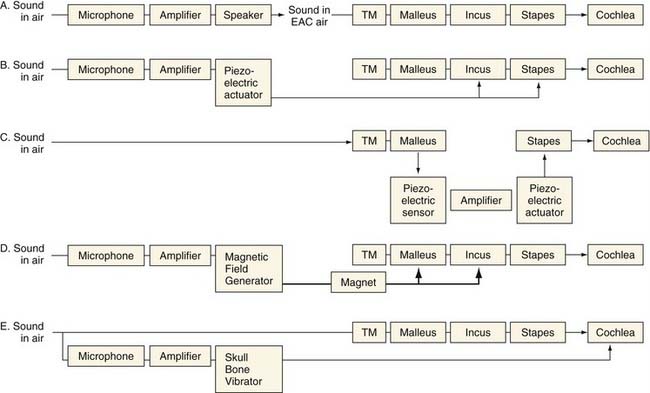
Conventional hearing aids function by receiving acoustic energy through a microphone, processing and amplifying the signal (in either an analog or a digital fashion), and transmitting the signal through a speaker adjacent to the eardrum. This amplified sound travels through the normal auditory pathway of the tympanic membrane and ossicles to the inner ear. Implantable middle ear hearing aids also employ a microphone that senses sounds and a signal processor that amplifies and alters the sound signal, just as in a conventional hearing aid. From here, they differ from conventional hearing aids. In one of several mechanisms unique to each device, the implantable middle ear hearing aids convert the electric signal into a mechanical energy that is coupled directly to the ossicular chain (see Fig. 157-1).The critical components of these systems are the transducer, which enables the device to output a signal that can be received by the ossicles, and the mechanism by which the transducer is coupled to the ossicles, which can either be a direct or indirect contact.15 Variations in these critical components distinguish the various implant designs (see Fig. 157-2). Goode and colleagues11 previously outlined the history of the development of implantable middle ear hearing aids.
Implantable middle ear hearing aids may also incorporate an electromagnetic transducer. These transducers generate a magnetic field using a coil carrying a current that encodes the microphone output. This magnetic field from the coil can cause motion in a ferromagnetic substance that is nearby, causing it to vibrate.15 As applied to middle ear implants, sound received from a microphone is converted by the signal processor, amplified, and sent to the electromagnetic transducer. The electromagnetic field that is set up vibrates a ferromagnetic unit coupled directly to the ossicles. In contrast to the piezoelectric unit that must be in direct contact with the ossicles, electromagnetic transducers need only to be near the ossicles, which have attached to them the ferromagnetic device that transmits the auditory signal to the ossicles.
These two types of amplification have different advantages for use in an implantable hearing aid. Electromagnetic transducers do not directly contact the ossicular chain, but rely on electromagnetic transmission to a ferromagnetic unit that is attached to the ossicles. Electromagnetic transducers can be packaged in a smaller housing, an important factor in the ear. In contrast, piezoelectric devices are larger and couple directly to the ossicular chain. The advantage of this type of transducer is its ability to deliver more distortion-free amplification directly to the ossicular chain.15 In either event, to accommodate patients with moderate to severe SNHL in the 55- to 90-dB hearing level range, any implant, whether electromechanical or piezoelectric, should be able to deliver a maximum mechanical stimulation output equivalent to 120 to 130 dB sound pressure level (SPL).16,17 How each implant achieves this output level is described subsequently.
Ossicular Coupling
As noted by Huttenbrink,18 to obtain optimal efficiency in implantable hearing aids, they must adapt to the mechanics of the middle ear and ossicular chain. As the third ossicle in the chain, and the one in continuity with the inner ear, the motion of the stapes is crucial in sound transmission. The stapes moves in a piston-like fashion.19 The ideal motion of the stapes by a prosthesis would be in this piston-like fashion. Any implant that directly attached to the stapes would function best by mimicking this motion.20,21
Electromagnetic Middle Ear Implantable Hearing Aids
Vibrant Soundbridge
The Vibrant Soundbridge is a semi-implantable hearing aid that was first introduced in 1997 (Fig. 157-3). Since its introduction in 1997, more than 2300 patients have been implanted worldwide.14 The device was approved for commercial availability in Europe in 1998, and in the United States in 2000. The electromagnetic transducer uses a proprietary vibrating ossicular prosthesis (VORP), which typically is attached to the long process of the incus. The VORP contains a rare earth magnet surrounded by a receiving coil, a demodulator package, a conductor link, and a proprietary floating mass transducer (FMT).22,23 The transducer was developed by Ball, and incorporated prior conceptual work performed by Goode and colleagues.11,22,24 The VORP is electrically connected to the internal receiver.25 These internal components are coupled to the audio processor via a telemetry link, similar to a cochlear implant. The processor, which is worn behind the ear, contains the microphone, audio processing electronics, magnet, telemetry transmission equipment, and room for a standard 675 zinc battery to power the implant.
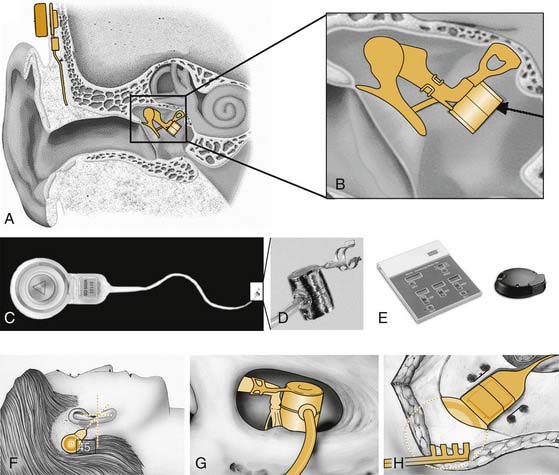
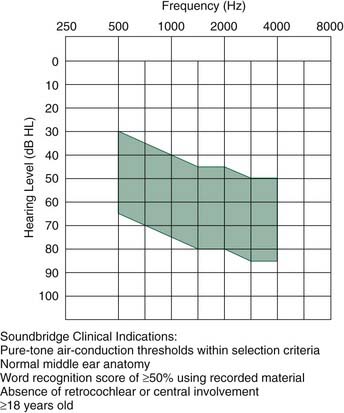
The Vibrant Soundbridge is indicated in patients with moderate to severe SNHL and desire for an alternative to an acoustic hearing aid (Fig. 157-4).23 Studies have indicated that it may be suitable for patients with hearing loss of 70 dB pure-tone average (PTA) hearing thresholds.26 When first introduced, the externally worn audio processor was an analog device that incorporated a wide dynamic range compression. Because of inadequate gain of the device, particularly at lower frequencies and with low sound levels,27 a newer, more powerful digital audio processor was introduced in 1999. Studies done shortly after its introduction failed to show superior hearing results compared with conventional aids, although patients preferred the device, in part because of ability to wear it for a much longer time without discomfort.26
The device typically is implanted using a standard transmastoid, facial recess approach to the middle ear. The VORP is crimped into the long process of the incus. The internal receiver is placed in a bony trough in the retrosigmoid bone several centimeters behind the ear, in a location similar to the receiver placed during cochlear implantation. One potential drawback of this design concerns the size of the VORP. Because of the confined space between the eardrum and the incus, the dimensions and mass of the FMT are limited, restricting its output.28 A second potential drawback is erosion of the incus long process, owing to ischemia at the clip attachment site. Modifications of the typical surgical approach allow treatment of mixed hearing losses resulting from otosclerosis or ossicular erosion or agenesis through direct placement of the VORP on the stapes superstructure, round window, or oval window.29–32
Owing to its primacy in regulatory approval processes and patient availability, to date more clinical data are available for the Vibrant Soundbridge than for all other middle ear implants. Results from the phase III clinical trial of 53 patients were sufficiently favorable to merit FDA approval of the device (phase I trials typically test feasibility and safety in a small group of subjects, phase II trials typically test effectiveness in a slightly larger group, and phase III trials assess safety and effectiveness in a large group).23 Patients in the study were analyzed with conventional analog hearing aids, digital hearing aids, and the Vibrant Soundbridge. Standard audiologic tests included pure-tone air-conduction and bone-conduction thresholds (250 to 8000 Hz), functional gain, speech recognition tests, the Profile of Hearing Aid Performance, and the Hearing Device Satisfaction Scale.
Although one patient had a shift of 18 dB after device placement, the effect of implantation on residual, native hearing was believed not to be significant (<10 dB PTA at 500 to 2000 Hz). This finding corroborated earlier studies that showed little to no effect of the presence of the FMT on hearing sensitivity.33
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


