Herpes Simplex Keratitis
Denis M. O’Day
Infection of the cornea with Herpesvirus hominis can present the ophthalmologist with a number of challenging and difficult problems. Much of what is known of the virus and its relationship to humans, its natural host, has been accumulated as a result of intensive research in the fields of virology and immunology. Gaps in our knowledge still exist and as these gaps narrow, our principles and methods of treatment will change.
In Western countries, infection with herpesvirus is almost universal. By early adult life, neutralizing antibodies are present in up to 90% of the population. Peaks of primary infections occur during infancy and adolescence, but sporadic cases are seen in the neonatal period and throughout adult life. In the majority, the primary infection is subclinical or goes undiagnosed. The disease usually runs a self-limited course but occasionally has a fatal outcome. With healing of the primary infection, the body is apparently free of disease; however, the virus has not been eliminated. Instead, having established a foothold, it persists permanently in an almost perfect symbiotic relationship that is marred by recurrent disease when the virus is reactivated from its apparent latent state.
Primary ocular herpes usually occurs as an acute follicular conjunctivitis with regional lymphadenitis and usually with vesicular ulcerative blepharitis. Most patients also have an epithelial keratitis, which persists somewhat longer than the conjunctivitis. Only rarely is there significant stromal involvement.
Recurrent episodes are a different problem. In these, the cornea is the principal target tissue. Males are infected twice as often as females, and attacks, although occurring all year, tend to be more frequent in autumn and winter. The most common form is the morphologically characteristic epithelial keratitis (dendritic, geographic, or punctate). Initially, there may be no serious sequelae to infection, but with repeated attacks, stromal keratitis, and associated uveitis may appear. Alternatively, disciform keratitis or other more heavily infiltrated stromal keratitis may develop without apparent preceding epithelial herpetic keratitis. When stromal keratitis supervenes, permanent structural damage to the cornea and to the rest of the eye exacts a heavy toll on vision. It is this effect, coupled with chronicity and resistance to treatment, that makes herpes simplex one of the most important viruses to affect the eye.
HERPES SIMPLEX VIRUS
MORPHOLOGY
Herpes simplex virus (HSV) is a member of the Herpesviridae family. The virion is 180 nm in diameter. It is composed of four principal components: the core, the capsid, the tegument, and the envelope (Fig. 1).
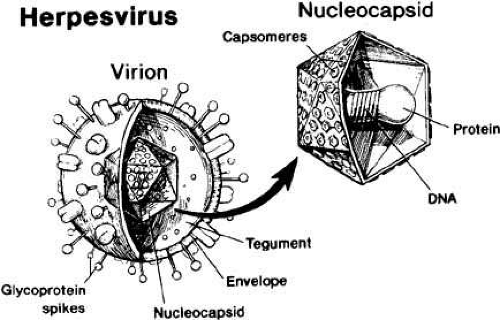 Fig. 1 Schematic morphology of herpes simplex virus. (Published courtesy of Liesegang TJ: Biology and molecular aspects of herpes simplex and varicella-zoster virus infections. Ophthalmology 99: 781, 1992) |
Core
The viral core contains double-stranded DNA used for viral replication. The viral genome has a molecular weight of 100 × 10,1,2 large enough to encode approximately 70 proteins and 72 genes.3 The viral DNA molecule is arranged as a double helix composed of two chains of repeating units of deoxyribose and phosphate, with purine and pyrimidine bases extending sideways from the sugar. The purine bases are guanine and adenine, whereas the pyrimidine are cytosine and thymine. The chains are linked together by the pairing of protruding bases to form the double helix. All the information required for virus replication is inscribed on the DNA molecule in a code constructed according to the order of repetition of the four bases. The physical form of the DNA of the virion in the replicating and latent virus is different. In the virion form of the virus, the DNA is linear but after infecting a cell it becomes circular. The viral DNA contains several classes of genes that encode regulatory proteins, structural proteins, and enzymes that are spread in a highly regulated fashion during the replicative cycle.4 Latency-associated transcripts (LATs) represent limited transcription of viral DNA during latency and serve as a marker for latently infected cells.3
Capsid
The viral DNA is enclosed within a protein shell with an icosahedral shape called a capsid. The capsid is composed of 162 five- or six-sided subunits called capsomeres.3 In addition to protecting the viral genome, the capsid allows entry of the viral DNA into the host cell.
Tegument
Outer Envelope
An essential component of the infective particle is the outer envelope. The envelope is composed of lipoproteins, carbohydrates, and lipids that have been derived from the host cell and have been modified by the viral protein.3,4 Embedded within the envelope and projecting from the external surface are glycoprotein subunits called peptomers, which play a role in viral attachment and penetration into the host cell.2,3
PATHOGENICITY
The virus shows a tropism for human tissues of ectodermal origin. In addition to the ocular infection and the well-known skin and mucous membrane lesions, herpes is responsible for a meningoencephalitis and has been associated with trigeminal neuralgia. In disseminated infections, it may replicate in liver, adrenal, and lung parenchyma.
REPLICATIVE CYCLE
HSV is an obligate intracellular parasite. Although it contains the genetic material necessary to induce its own replication, it does not have the metabolic machinery necessary for biomolecular synthesis. It enters the host cell and uses the host cell metabolic pathways, often causing destruction of the host cell. The replicative cycle has three phases: entry, eclipse, and envelopment and release.
Entry Phase
The host cell and the virus come in contact and bind by means of specific cell surface glycosaminoglycans, principally heparan sulfate.2,6 Lytic genes are expressed, and the virus enters the cell fusion of the virion envelope with the cell’s plasma membrane. It then penetrates the host cell cytoplasm in a pinocytotic vesicle, where the envelope is removed. Enzymatic digestion results in uncoating of the capsid. The bare viral capsid moves to the host cell nuclear pore, where it is disassembled and the viral DNA released.
Eclipse Phase
The eclipse phase of the replicative cycle is characterized by intense molecular activity within the host cell nucleus and loss of recognizable viral morphology. The viral DNA unwinds and is transcribed by messenger RNA, which in turn directs viral protein synthesis within the ribosome. Enzymes, structural proteins, and regulatory proteins are produced. Most of the proteins are returned to the nucleus. DNA replication and capsid reassembly occur there.
Envelopment and Release
Within 6 hours of entry, fully enveloped particles are detectable in the cells. The new viral particle is enclosed by the envelope, which is primarily derived from a nuclear membrane as it leaves the nucleus and enters the cytoplasm. The mature infected virus negotiates the cell membrane by a process of reverse phagocytosis to reach the extra cellular space. The cycle is now complete.7
SEROTYPES
On the basis of site of isolation from the body and cell culture characteristics, two types of herpes simplex virus can be distinguished. HSV-1 characteristically produces oral, facial, and ocular lesions. It is responsible for 85% of ocular isolates. HSV-2 serotype has conventionally been associated with the sexually transmitted form of the disease. It is responsible for ocular disease in neonatal herpes simplex keratitis but in only minority of adult ocular infections. Simultaneous keratitis infection with both HSV-1 and HSV-2 has been described in a patient with acquired immune deficiency syndrome (AIDS).8
HERPES SIMPLEX VIRUS INFECTION
EPIDEMIOLOGY
Humans are the only natural host of HSV, although experimental infection can be produced in a variety of animals, including rabbits, mice, and primates. Persons infected with the virus constitute the sole reservoir of infection. Humans are extremely susceptible to infections with Herpesvirus. Given this highly susceptible host, poor sanitary conditions and overcrowding greatly predispose to infection. Studies of the presence of neutralizing and complement-fixing antibody within different socioeconomic groups as an index of infection have underlined this relationship. In the lower socioeconomic groups in the United States, 80% of individuals have antibodies. This contrasts with 50% of those more economically advantaged.9 As standards of living increase, an increase in the number of susceptible adults can be anticipated, with a subsequent increase in the incidence of adult primary herpes simplex.
Transmission of HSV-1, which is responsible for the vast majority of facial and ocular herpetic infections, occurs either from direct contact or via contaminated secretions. It has been shown that virus particles are shed intermittently or chronically in tears,11 saliva,12 and respiratory secretions,13 as well as from the genital tract in the absence of overt disease.
Mechanisms of spread from the portal of entry are not known precisely, but a viremia appears likely and has been demonstrated in severe conditions on a number of occasions. The incubation period of HSV-1 is 3 to 9 days.14 The overwhelming majority of primary infections occur in infancy and adolescence, but sporadic cases of primary infection occur among susceptible individuals throughout adult life. The primary infection is subclinical in 85% to 90% of cases.15 A positive titer of serum-neutralizing antibodies is noted by 1 week after the primary infection. The titer then diminishes but remains positive throughout life. Complement-fixing antibody follows a similar pattern but is more variable during asymptomatic periods. Occasionally, primary HSV-1 is ocular and causes lid vesicles, ulcerative blepharitis, keratitis, and conjunctivitis.
Infected persons become carriers of the disease by transneuronal spread of the virus into the neural ganglia. The virus persists there in a quiescent state called latency that may be interrupted by periods of localized recurrence. A variety of endogenous and exogenous stimuli, such as strong sunlight, fever, menstruation, and psychiatric disturbances can serve as triggers of reactivation. In addition, reactivation in the cornea can be precipitated by local factors, one of which has been shown to be exposure to excimer laser irradiation during refractive surgery.
Ocular herpetic involvement is less common than systemic infection. Projections from a prevalence study in the northern United States to the whole country suggest a total of approximately 20,000 new cases per year and 400,000 with a diagnosis of ocular herpes simplex.18
Herpes simplex infection is the most common cause of corneal blindness in developed countries.
PATHOGENESIS AND LATENCY
The pathogenesis of human herpes simplex ocular infection exhibits two critical features: complexity and diversity. This is demonstrated in the marked differences in pathogenesis between primary and recurrent ocular disease. It is also apparent in the many different forms of ocular disease that result from the complex interplay of viral replication, host defense systems, and tissue reparative responses. Further confusion arises for the ophthalmologist in the management of herpetic eye disease: appropriate therapy for one clinical form of disease may be absolutely contraindicated in another clinical form.
The natural history of HSV-1 infections in humans is generally characterized by an initiating childhood infection, which may present as a nonspecific upper respiratory infection or may be totally asymptomatic. Goodpasture20 in 1929 and subsequently others21,22 postulated that the virus gained access to the central nervous system during the primary infection by moving centripetally along sensory nerves to the sensory ganglia. In 1973, Cook and Stevens24 confirmed the concept of retrograde axonal transport and latency in ganglia.
The process leading to latency is now understood to occur in three stages: Entry, Spread and Establishment of latency. Entry defines the time of the primary infection. Spread is the phase during which the virus moves to the terminal axons of the sensory neurons and then, by retrograde axonal transport to the neuronal cell bodies in sensory and autonomic ganglia where there may be further viral replication. In the final stage, Establishment of latency, lytic gene expression is suppressed and virions cannot be detected. However, the viral genome persists in the neuron.
Under the influence of various stimuli, control of latency breaks down and viral replication begins again in the ganglia with spread to peripheral sites where replication may also occur.25
The mechanisms by which the virus maintains latency and is ultimately altered to cause recurrent disease are only partially understood. While in the latent state, viral gene expression is suppressed almost totally. Viral structural component and infectious viral particles are not produced, although virus can be detected by cell culture explantation techniques. However, viral RNA molecules called LATs3,5,26 are transcribed. The LATs serve as useful markers for latent HSV infection. LATs may play a role in reactivation.
There is also evidence to suggest that latent infection can occur at ocular sites such as endothelial cells or keratocytes.27,28,29,30 This has raised the question of whether extraganglionic latency occurs within the cornea. HSV-1 DNA sequences have been identified in some human corneas that do not have any history of herpetic eye disease5,27; however, the existence of corneal latency has not been firmly established. The possibility of corneal latency has important clinical ramifications for it would allow for viral reactivation and replication within the cornea without ganglionic HSV reactivation.
Recurrent clinical disease apparently occurs when local host defenses in the eye are unable to control the virus, or there is a break in the epithelial barrier function. It is clear that recurrent clinical disease occurs despite systemic humoral and cell-mediated immunity against the virus.
Interactions
Strain variations in HSV appear to affect reactivation. Certain strains are associated with high recurrence rates.31 Genetic differences among strains appear to affect the clinical manifestations of infection, including the morphology of an epithelial dendrite. Certain strains are more likely to produce stromal disease and this has been correlated with the amount of glycoprotein produced during infection.32,33 The impact of corticosteroids on the course of the epithelial infection also appears to be strain related.34 Corticosteroids may lead to an increased duration of herpetic disease by interrupting the immune system, but it is unlikely that they induce viral reactivation.
The host response to the virus plays a role in the disease process. However, the importance of individual host differences in determining the course of infection is unclear. For unknown reasons, herpetic infection does appear to be more common in patients with atopic disease.15
MANAGEMENT
Treatment of herpes simplex keratitis should be tailored according to the clinical form of herpetic disease that is present. Purely epithelial herpes simplex keratitis is typically managed with topical antiviral agents with or without debridement. The management of stromal and disciform endotheliitis is more complex and usually involves both antiviral and anti-inflammatory measures. Surgery may be necessary in more severe forms of this disease. Specific therapy for each of these entities is discussed in detail in the following sections.
In general, a rational approach to therapy for ocular herpes simplex disease should include:
Minimize permanent ocular damage from each recurrent episode.
Avoid iatrogenic disease.
Counter the socioeconomic effects of a chronic debilitating disorder.
Such an approach is possible only if the ophthalmologist maintains a clear perspective of the chronic, recurring, progressive course of this disease. The nature of herpetic keratitis is such that these aims are often in conflict. The topical antiviral agents used are inherently toxic and the vigilance needed to manage the patient carefully for protracted periods of time is demanding, as well as potentially socially and economically crippling. Only currently established methods of treatment are included here. Controversial therapies and drugs, given the experimental stage of development, are not discussed.
Antiviral Measures
MECHANICAL DEBRIDEMENT
At one point, mechanical debridement was the only effective means of treating epithelial herpes. Even with the advent of antiviral agents, it remains a useful, safe, and sometimes preferred alternative.35 The removal of virus-replicating epithelium abolishes the source of infection for other cells and eliminates an antigenic stimulus to inflammation in the adjacent stroma.
Debridement should be performed at the slit lamp or operating microscope, with the use of topical anesthesia. Controlled removal of the lesion is best achieved by gentle debridement along the margins of the epithelial ulcer with a tightly rolled cotton-tipped applicator. With this technique, known as minimal wiping debridement, the virus-infected cells are removed while healthy epithelium is left intact.36 Sharp knife blades should not be used because of the risk of creating a portal of entry into the stroma through damage to underlying Bowman’s layer. Recrudescence of viral replication occasionally occurs and can be treated by repeat debridement or administration of an antiviral agent. Chemical virucidal agents, such as phenol 10%, have been advocated to sterilize the freshly debrided ulcer margins but are unnecessary. Scrubbing the bare surface is injurious, and iodine is damaging, especially to diseased corneal stroma.
CHEMOTHERAPY
Idoxuridine (IDU), the first antiviral drug to become available for topical ophthalmic use, is a substituted pyrimidine nucleoside that resembles thymidine (Fig. 2). It is phosphorylated to the nucleotide and incorporated into the DNA of all cells, where it interferes with DNA interactions.
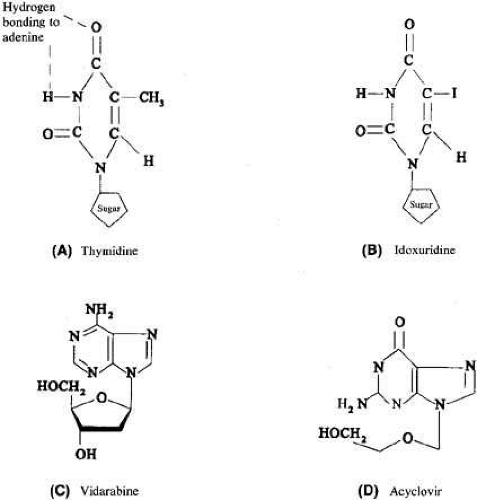 Fig. 2 Chemical structures of A thymidine, B Idoxuridine, C vidarabine, and D acyclovir. |
Disadvantages include poor corneal penetration,37 lack of selectivity for virus-infected cells, and toxicity. In the majority of patients, the earliest signs of toxicity are recognizable after 2 weeks of therapy. These include punctate keratoplasty, burning, injection, irritation, lacrimation, hypersensitivity, and punctal stenosis (Table 1).
TABLE 1. IDU Toxicity* | |||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||
Vidarabine, first synthesized in the early 1960s, is a purine nucleoside analogue with in vitro activity against Herpesvirus and certain other DNA viruses. Cellular enzymes convert vidarabine to the triphosphate form, which acts as a competitive inhibitor of DNA polymerase. Corneal penetration is poor but better than that of IDU. Because vidarabine does not selectively inhibit virally induced enzymes, there is potential for cellular toxicity. It is probably less toxic than IDU. Vidarabine is available as a 3% ophthalmic ointment, and the usual dose is five times per day. Collaborative studies have indicated that vidarabine is effective in the therapy of epithelial herpetic disease.38 As with IDU, resistant strains exist, but cross-resistance has not been observed. Hypertrophic epithelial changes similar to those seen with IDU occur, and some hypersensitivity reactions have been reported.
Trifluridine, a thymidine analogue that inhibits thymidylate synthetase, is incorporated in both viral and cellular DNA. It is semi selective, interfering with viral metabolism in preference to normal cellular metabolism, and is thus less toxic than IDU. Trifluridine is 10 times more soluble in water than IDU and is available as a 1% drop. Studies have shown the healing time for active epithelial ulcers to be better than that with IDU and comparable to that with vidarabine.12 When used in higher doses for prolonged periods of time, toxicity does develop, producing changes similar to those seen with IDU, although not as severe.
Acyclovir is an acyclic analogue of guanosine and is the prototype of the generation of specific antiviral drugs that are activated by a viral thymidine kinase to become potent inhibitors of viral DNA polymerase. The selectivity of acyclovir for virus-infected cells is approximately 200 times that for normal cells. Its antiviral spectrum is limited to the herpes group and excludes vaccinia, adenovirus, and RNA viruses.39 Acyclovir is available in the United States in oral and intravenous forms, and as a topical dermatologic ointment. Topical 3% acyclovir ointment for ophthalmic use (not commercially available in United States) can penetrate the cornea to reach the anterior chamber.40,41 It has been shown to be effective in the treatment of HSV epithelial keratitis.40,41
Oral acyclovir in a dosage of 400 mg five times per day results in therapeutic levels in the aqueous42 and tear fluid.43,44
In a recent analysis of 97 randomized treatment trials for herpes simplex epithelial keratitis comparing the efficacy of topical or oral antiviral agents with or without debridement, Wilhelmus45 concluded that vidarabine, trifluridine and acyclovir are effective and nearly equivalent. In contrast to treatment with idoxuridine, treatment with vidarabine, trifluridine or acyclovir resulted in a significantly greater proportion healing in one week. The combination of a nucleoside and debridement seemed to hasten healing.45
Valcyclovir is the L-valyl ester prodrug of acyclovir with enhanced bioavailability and significantly greater plasma concentrations of acyclovir than can be achieved with oral acyclovir.46 Although there are reports of animal studies, no case series or controlled trials have been published.
Anti-inflammatory Measures
Administration of topical corticosteroid is contraindicated in the treatment of herpes simplex epithelial keratitis. In the management of HSV stromal and disciform endotheliitis, topical corticosteroid therapy combined with prophylactic antiviral cover is a typical form of treatment. Controversial aspects of corticosteroid therapy is discussed in detail below.
It is logical to limit inflammatory response in the cornea, because this is largely responsible for the destructive effects of herpetic infections. This inflammation has an immunologic basis and might therefore be combated by systemic and local immunosuppressive measures. For herpetic disease, the disadvantages and the dangers of systemic immunosuppressive therapy make its use undesirable.
Corticosteroids can modify the immune response in a number of ways. Applied locally in the cornea, their effect seems to be chiefly on the efferent arc, possibly inhibiting chemotaxis and degranulation of polymorphonuclear leukocytes. Although they also inhibit local antibody production to some degree, their influence on the afferent arc and central responses is probably less important. Corticosteroids appear to have more effect on hypersensitivity reactions mediated by humoral antibody than by cell-mediated immunity, although their action in controlling corneal allograft reactions suggests that they may block such reactions by causing destruction of sensitized lymphocytes.
Steroids are associated with a number of complications that tend to diminish their effectiveness and at times prohibit their use:
Enhancement of viral replication. Steroids clearly foster Herpesvirus replication in the corneal epithelium once this has been initiated. For this reason they must never be used in the treatment of epithelial herpes. The demonstration of replicating virus in corneal stroma and deeper ocular tissues by electron microscopy suggests that steroids may also enhance virus replication in these tissues. There is as yet no conclusive evidence of this, and experiments in animals have yielded conflicting results.47 Nevertheless, in the absence of an antiviral agent that can effectively penetrate the corneal stroma, the possibility of enhancement of virus replication must cause concern.
Secondary infection. The immunosuppressive effects of steroids may allow bacteria and fungi to proliferate in the absence of specific therapy.
Elevation of intraocular pressure. Prolonged administration produces an elevation in intraocular pressure in some patients. In our experience, the latent period before the pressure begins to rise can be quite variable and may be prolonged. The effects of an unrecognized pressure elevation in an already diseased eye are devastating.
Cataract formation. Posterior subcapsular cataracts that may progress to complete lens opacities have been associated with systemic steroids. However, prolonged local administration is also a risk factor for cataract.
In the presence of an inflammatory stimulus such as residual herpes simplex antigen, a rebound in the inflammatory response almost invariably follows the cessation or too rapid reduction in the topical steroid therapy. As a consequence of the removal of steroid, immature leucocytes proliferate and produce antibody in large amounts. Antibody complexes with antigen and the resulting inflammatory cascade leads to invasion of the cornea by a new wave of polymorphonuclear leucocytes. This inflammatory rebound may lead to rapid deepening of corneal ulceration and perforation. Clinically, the exacerbation in corneal inflammation may be mistaken for deteriorating underlying disease.48
It is clear that steroids are dangerous preparations in inexperienced hands because they introduce new hazards to an already complex and difficult situation. Nevertheless, they are the only effective anti-inflammatory agent available. It is mandatory that the clinician be constantly aware of these hazards. The haphazard administration of steroids in poorly monitored patients contributes significantly to the disastrous sequelae of this disease.
PRIMARY HERPES
CLINICAL MANIFESTATIONS
Primary ocular herpes is predominantly a disease of infants and young adults, but it can occur sporadically at all ages. Neonatal infection is caused by HSV-2 in approximately 80% of cases. The scant emphasis that primary herpetic infection has received in the literature is regrettable in view of its importance as a cause of follicular conjunctivitis or keratoconjunctivitis.11 These conditions remain largely unrecognized, therefore, affected patients may be exposed unwittingly to the hazards of corticosteroid administration.
Although this section is principally concerned with the keratitis that often follows primary follicular conjunctivitis, it would be unrealistic to consider it as an entity distinct from the primary syndrome. Symptoms of infection appear 2 to 12 days after contact with an infected individual (although not necessarily one with an active lesion). In contrast to the recurrent form of the disease, there is mild malaise and fever, indicating a constitutional illness. Conjunctival injection, irritability and watery discharge are typically unilateral and rarely severe. The patient or parents, whose chief concern may be the skin lesions adjacent to the eye, may not even mention the ocular disease.
The follicular conjunctivitis of primary herpes is associated with a regional adenitis. Typically, the ipsilateral preauricular lymph node is slightly enlarged and a little tender. Swollen lids and a primary skin lesion are often readily apparent (Figs. 3 and 4), but on occasion only a careful search will reveal the single or grouped vesicles of crusted ulcers (Figs. 5 and 6) hidden among the lashes or in the intermarginal strip. Similar lesions may be located elsewhere on the face or at the mucocutaneous junction of the mouth, in the nose, or on the trunk, and they may be easily missed unless a specific search is made. In nearly one fourth of cases, no cutaneous lesions are present.35 The conjunctiva is injected and edematous. Follicles develop, especially in the fornices, and extend to the tarsal areas (Fig. 7);they rarely occur at the limbus. Small subconjunctival ecchymoses are not uncommon and phylectenule-like lesions may develop on the globe (Fig. 8).
 Fig. 3 Child with primary ocular herpes. (Courtesy of Dr. S. Darougar) |
 Fig. 4 Primary herpetic blepharoconjunctivitis in an adult. |
 Fig. 5 Herpetic ulcer on lid margin in a patient with primary herpes. (Courtesy of Dr. S. Darougar) |
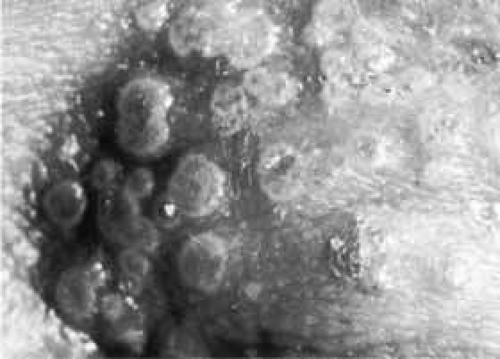 Fig. 6 Umbilicated primary herpetic lesions at the inner canthal area. (Courtesy of Dr. S. Darougar) |
 Fig. 7 Acute follicular conjunctivitis in primary herpetic infection: A Upper tarsus, B Upper fornix, C Lower fornix. (Courtesy of Dr. S. Darougar) |
 Fig. 8 Chemosis and ecchymosis of bulbar conjunctiva. (Courtesy of Dr. S. Darougar) |
Within 2 weeks, approximately half of these patients develop corneal lesions associated with only relatively minor symptoms: a little grittiness, photophobia, and blurring of vision. Initially these lesions are epithelial and present a variety of appearances.
A fine punctate epithelial keratitis, consisting of tiny white flecks in the superficial layers that stain poorly with fluorescein and variably with rose bengal, may be present. These are transient spots, only rarely progressing to larger lesions. As the flecks desquamate, fluorescein stains the flecks more intensively during the healing stages.
A coarse punctate epithelial keratitis presenting a variety of shapes (circles, ovals, irregular elongated areas, and stellate figures) may appear. Any of these lesions may progress to macroscopic dendritic figures. They consist of slightly raised, closed clusters of opaque epithelial cells, those in the periphery often being the most regularly arranged. These swollen white cells stain well with rose bengal but poorly with fluorescein. Typical herpetic intranuclear inclusions can be demonstrated in these cells (Fig. 9). Initially, there is no stromal reaction, but within 2 to 3 weeks, and sooner if the lesions are peripheral (and regardless of epithelial healing), subepithelial infiltrates appear.35
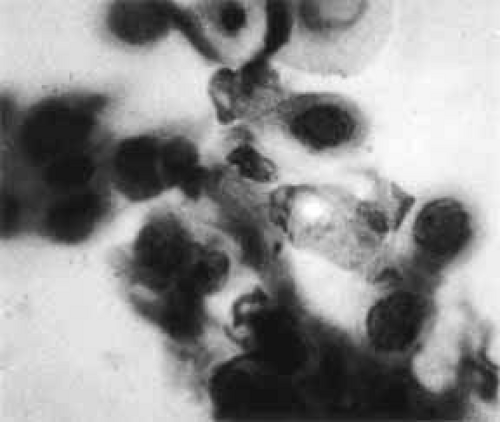 Fig. 9 Corneal epithelial cells stained in vivo with rose bengal in a child with coarse punctate corneal epithelial lesions of primary Herpesvirus infection. The cells were subsequently removed and counterstained with hematoxylin. Many stained cells are swollen and show eosinophilic intranuclear inclusions with margination of chromatin. |
DIAGNOSIS AND DIFFERENTIAL DIAGNOSIS
The diagnosis can be made on clinical grounds alone in patients with typical cutaneous lid lesions or typical herpetic corneal lesions. In the absence of such lesions (approximately one fourth of all patients with primary herpetic conjunctivitis), laboratory investigations are essential for diagnosis. The differential diagnosis includes:
Keratitis with lid lesions: zoster, chickenpox, molluscum contagiosum, and ulcerative blepharitis with keratitis caused by staphylococcal infection.
Keratitis without lid lesions: vaccinia, adenoviral infections (types 3, 7, and 8 and 19), chlamydial infections, herpes zoster and Epstein-Barr keratitis.
LABORATORY INVESTIGATIONS
In most cases, laboratory confirmation of the clinical diagnosis is unnecessary. In the remainder, an attempt should be made to isolate the virus from untreated active lesions in skin and cornea and from the conjunctiva. Positive cultures may take from 2 to 5 days to develop.
Typical viral multinucleate giant cells may be demonstrated in Giemsa-stained scrapings of the base of cutaneous lesions on the lid. These are also seen in varicella or zoster.
The appearance of neutralizing and complement-fixing antibodies a week after the onset, followed by a rising titer for the next few weeks, is useful confirmatory evidence. The cytology of cornea and conjunctival scrapings is useful in conjunction with antibody levels but is not diagnostic.
MANAGEMENT
Therapy must be directed toward the elimination of virus from the cornea and adjacent skin lesions. It is essential that lid vesicles and ulcers be treated concurrently with the corneal disease because they are a potent source of virus that, being continually shed, can reinfect the cornea and vastly prolong the keratitis.
Trifluridine is instilled into the conjunctival sac fives times per day. An antiviral ointment (acyclovir) can be applied to the eyelid and adjacent skin lesions. Topical corticosteroids are contraindicated.
Systemic administration of acyclovir is recommended for neonatal infections because of the enhanced risk of systemic disease as a result of viral dissemination. In this age group, administration of eye drops can be difficult. The addition of systemic therapy has the added benefit of ensuring adequate therapeutic concentrations in the eye. In older children and adults with a primary infection, systemic therapy is usually unnecessary.
Since the advent of topical antiviral agents, debridement of the corneal epithelium is seldom performed but it remains an effective method of healing the corneal lesions. Solitary vesicles on the lids may be removed by general debridement with a cotton-tipped applicator moistened with phenol.
A cycloplegic may be prescribed when indicated to relieve photophobia or ciliary spasm. The use of Atropine should be avoided because of the risk of hypersensitivity. Scopolamine hydrobromide 0.25% twice daily or cyclopentolate hydrochloride 1% to 2% three times daily is usually effective. Patching is undesirable. However, wearing sunglasses may give symptomatic relief.
A return visit is advisable within 2 to 3 days in all but the mildest infections. Thereafter, patients can be seen weekly, provided recovery is uneventful. The administration of an antiviral agent must be continued until corneal and lid lesions are healed. Hospitalization is rarely necessary, except in patients with severe bilateral and secondary infections.
The following steps are necessary only when the diagnosis is in doubt.
VIRAL ISOLATION
Cornea
Gently swab the surfaces of the lesion with a dry, sterile, cotton-tipped applicator. Place the applicator in a viral transport medium for later inoculation into tissue culture. If cell lines of the culture are not immediately available, the specimen can be frozen at -4°C.
Conjunctiva
Gently swab (or preferably scrape) the conjunctiva in a similar manner.
Lid lesions
Unroof ulcers and vesicles with a fine needle tip prior to taking the specimen with a cotton-tipped applicator.
CYTOLOGY
Gently scrape the opaque cells of the corneal lesion onto a glass slide, using a platinum spatula, Beaver blade, or Bard-Parker knife. This is best done under magnification, preferably at the slit lamp. Stain with Giemsa.
ANTIBODY TITERS
On initial presentation, blood is drawn for neutralizing antibody titers. Two to 3 weeks later, another sample is assayed to determine whether the titer has risen.
BACTERIAL CULTURES
Cultures of the eyelid lesions and conjunctival sac are desirable. They should be accompanied by direct smear if bacterial infection is suspected.
NATURAL COURSE AND VARIATIONS IN CLINICAL PRESENTATION
The epithelial lesions tend to heal, but additional crops may appear if active herpes persists untreated on the lids. The superficial stromal infiltrates may persist for several weeks before gradually resolving. Healing may be accompanied by superficial scarring in these sites. Occasionally, these stromal lesions progress to a frank disciform keratitis indistinguishable from the type usually associated with recurrent herpes.
Primary herpes uncommonly presents as a bilateral ocular disease, except in atopic individuals, who tend to have a more florid form of disease.49 In rare instances, the course of primary infection is severe: widespread herpetic infection in the face and trunk, often pustular and accompanied by a severe systemic illness, may supervene and is characteristic of Kaposi’s varicelliform eruption. Encephalitis and hepatitis occur rarely but can be lethal, especially in infants.
COMPLICATIONS
Secondary bacterial infection occasionally supervenes. The appropriate antibiotic, the selection of which is made from the results of culture and sensitivity testing, best treats it locally. Severe cellulitis of the lids may require systemic antibiotics. Prophylactic antibiotics are unnecessary and may confuse the clinical picture. In atopic individuals, management can be difficult, because topical antivirals may not be tolerated. Careful debridement of the lesions is an alternative in these situations.
Permanent damage to the cornea is uncommon. Most of the opacification in the stroma seen during active infection is probably caused by temporary edema rather than scarring. Should stromal keratitis develop, it is treated in accordance with the principles of management of recurrent disease (discussed later). Transient superficial stromal infiltrates do not require treatment.
PROGNOSIS
Most primary infections respond rapidly to antiviral therapy with little or no sequelae and no loss of vision. Occasionally, the development of antiviral toxicity necessitates cessation of the drug therapy. Complications occur mainly in undiagnosed or ineffectively treated cases.
RECURRENT HERPES SIMPLEX
Recurrent HSV infection occurs as a result of reactivation of the virus in latently infected ganglia. Recurrent ocular HSV infection is thought to be caused by reactivation of the virus in the trigeminal ganglion. The virus travels down the nerve axon to the sensory nerve endings, where it is transferred to corneal epithelial cells and keratocytes. If favorable conditions exist in the epithelium, viral replication and cell lysis ensue, producing clinical disease. HSV-specific nucleic acid sequences have been detected, and HSV has been organ-cultured from corneal buttons excised from patients with chronic stromal keratitis. These patients had no active disease at the time that penetrating keratoplasty was performed. These data suggest that the human cornea may also be a site of latency and a potential source of recurring clinical ocular disease.50
There are several different types of recurrent ocular HSV infection, including dendritic and geographic epithelial keratitis, interstitial and necrotizing stromal keratitis, disciform endotheliitis, and uveitis.
EPITHELIAL KERATITIS



