Chapter 59 Extreme Lateral Infrajugular Transcondylar Approach for Resection of Skull Base Tumors
The extreme lateral infrajugular transcondylar (ELITE) approach was born out of the anatomic constraints and operative challenges presented by the cranial base. The transcondylar approach was first devised as an avenue for access to the foramen magnum and ventral medulla.1,2 In 1986, Heros3 described the extreme lateral inferior suboccipital approach for access to vertebral and vertebrobasilar artery lesions. The ELITE approach is a special transcondylar and transjugular tubercle skull base approach developed and elaborated in Germany and Japan in 1987.4,5 After years of refinement, this has become a very useful and well-described approach for this region of the skull base.
Paragangliomas of the temporal bone were first identified as a unique entity in 1945.6 Attempts at characterization and ultimate surgical resection were initially fraught with high morbidity and mortality because of their location amidst complex anatomic structures. Primary treatment with radiation therapy soon became the mainstay for therapy with the hopes of limiting complications. Radiation therapy has been shown to be superior to observation of these lesions; however, the long-term risks of malignancy and radiation morbidity limit its success.7–10 Definitive surgical resection remains the mainstay for attempted cure.
Attempts at surgical resection and cure led to the development of tumor classification strategies to help guide surgical planning and to improve communication of results. Two main classification schemes were devised and remain in use today, primarily in the otology/neurotology literature—the Fisch11 and Glasscock-Jackson classifications.12 The Fisch scheme is as follows:
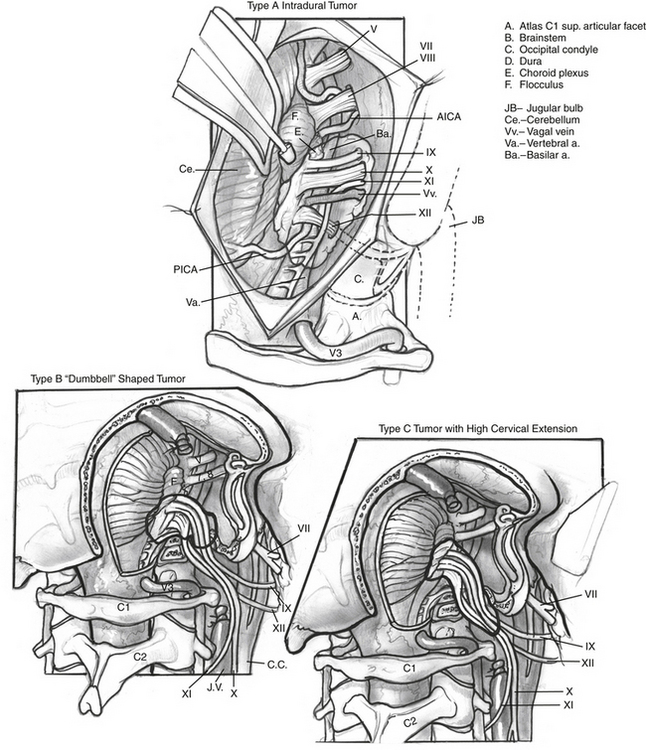
The authors have used a simpler classification of tumors in this location, and modifications and additions to the ELITE approach—including transsigmoid, transjugular, infrajugular, and high cervical approaches—are tailored to provide needed exposure for tumor resection (Fig. 59-1):
SURGICAL PROCEDURE
A preoperative arteriogram and embolization are performed 48 hours before the surgical procedure.13 Facial nerve monitoring is carried out in all cases. The surgeon may consider additional monitoring, including auditory brainstem evoked potentials, somatosensory evoked potentials, motor evoked potentials, and monitoring of CN X, XI, and XII. An electromyographic endotracheal tube can be used for CN X monitoring, and electrodes placed directly into the sternocleidomastoid muscle and the tongue can be used for CN XI and XII monitoring. Before the incision, perioperative antibiotics and corticosteroids are administered.
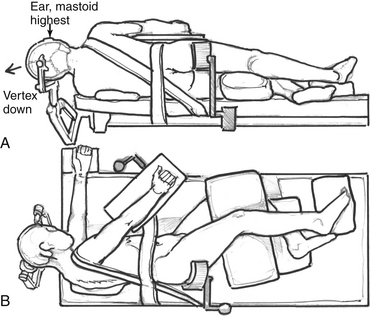
Patient positioning and incision differ for the dorsolateral and anterolateral modifications. For the dorsolateral ELITE procedure, the patient is placed in a lateral decubitus position (Fig. 59-2A and B). For the anterolateral approach, the patient is positioned in a supine fashion with the head displaced away from the side of the lesion. A shoulder roll is placed to aid with the high cervical portion of the procedure and to raise the shoulder on the side of the lesion. Obese patients and patients with very short necks may be placed in a lateral position if necessary. The patient should be padded and secured for ease of rotation of the table throughout the case.
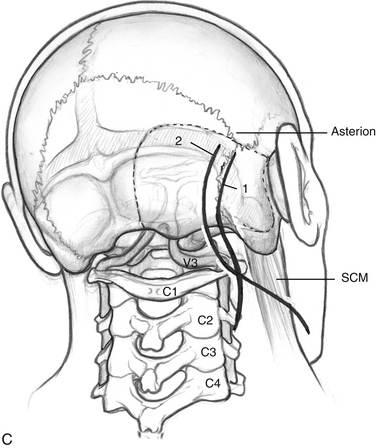
Incisions are shown in Figure 59-2C. For the dorsolateral approach, a lazy S incision is used, 1 to 2 cm posterior to the mastoid bone, and extending inferiorly along the hairline. For the anterolateral ELITE procedure, a retroauricular curvilinear C-shaped, or question mark–shaped, skin incision is begun approximately 2 to 3 cm posterior to the upper border of the ear. Inferiorly, this incision is carried down into the neck, traversing the border of the sternocleidomastoid muscle (SCM) and running parallel to the body of the mandible, approximately two fingerbreadths below. The skin flaps are raised. For the dorsolateral approach, the SCM is retracted anteriorly; for the anterolateral approach, the SCM is retracted posteriorly. The inferior edge is raised in the subplatysmal plane. Superiorly, the temporoparietal fascia is elevated as a separate flap under the skin flap, after it is dissected off the bone with the periosteum.
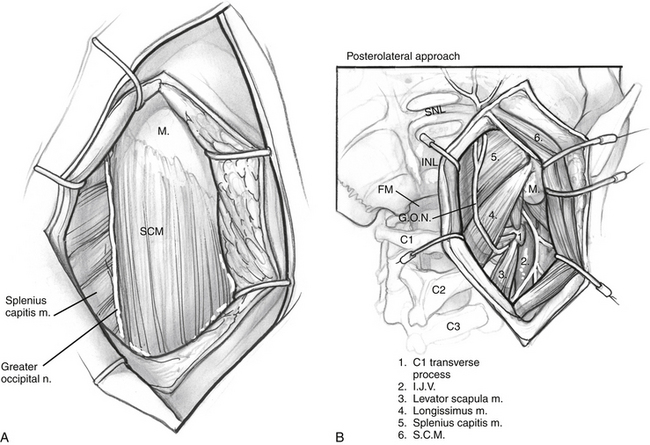
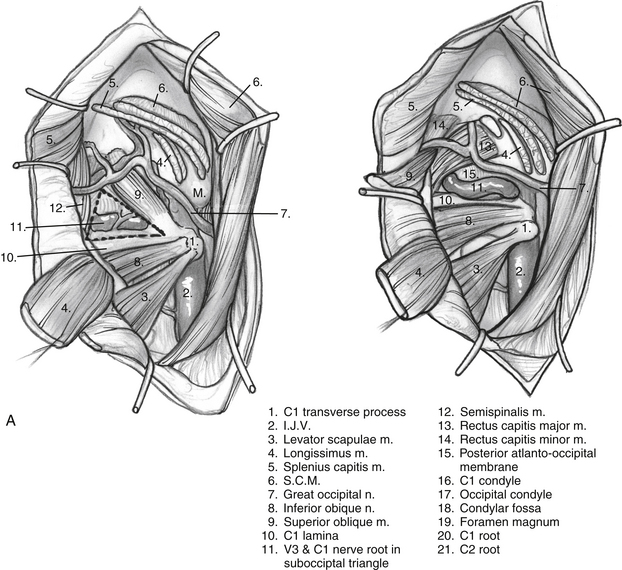
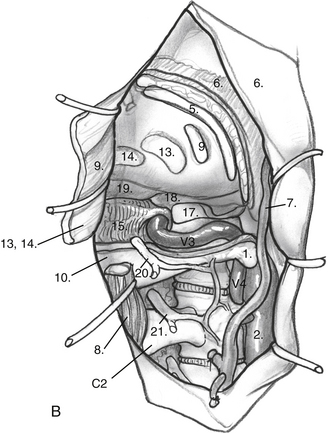
The anterior flap is now reflected, and the posterior auricular muscle should be visible behind the external auditory canal. Inferiorly, the greater auricular nerve should be seen crossing the SCM approximately 3 cm below the mastoid tip. This nerve can be preserved for use as an interposition graft, if needed. The posterior flap is displaced, and the posterolateral neck muscles are reflected to expose the mastoid more fully. This group of muscles is composed of three layers (Fig. 59-3). The superficial layer is composed of the SCM and splenius capitis muscles. The middle layer consists of the longissimus capitis and semispinalis capitis. These muscles are reflected to expose the deep layer, which consists of the rectus capitis posterior major, the obliquus capitis superior, and the obliquus capitis inferior muscles. These muscles form the suboccipital triangle (Fig. 59-4A). The styloid diaphragm also is identified in this region. Beneath that diaphragm runs the occipital artery as it courses beneath the posterior belly of the digastric muscle (Fig. 59-4B).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


