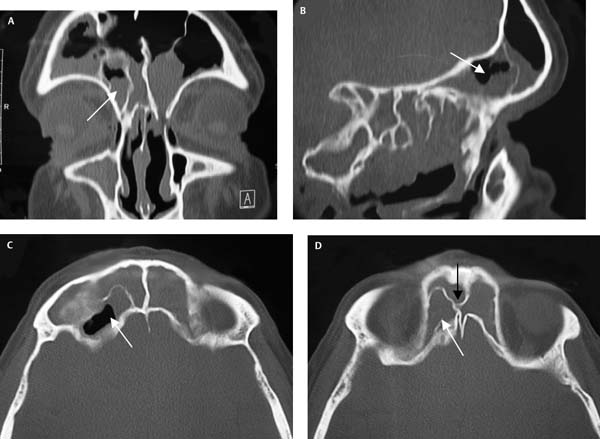
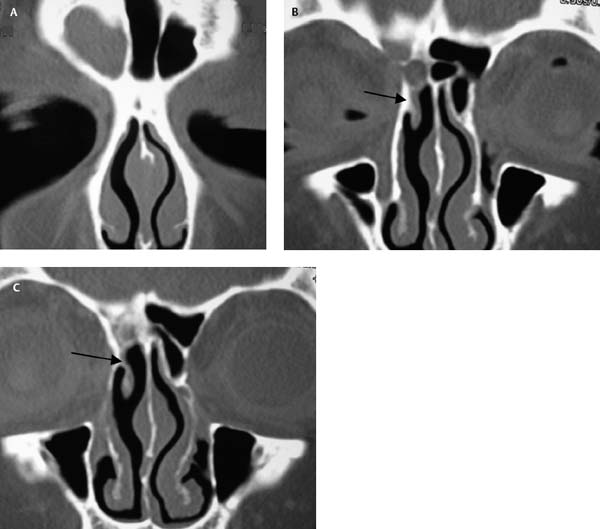
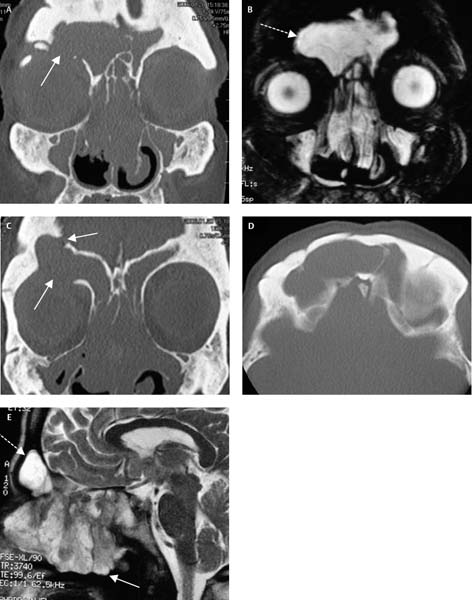
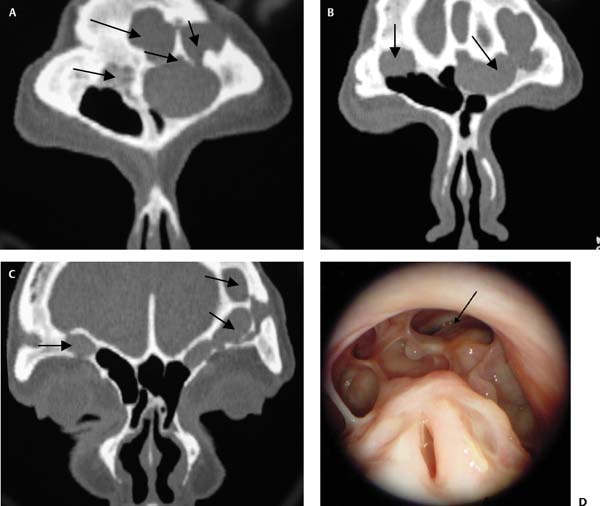
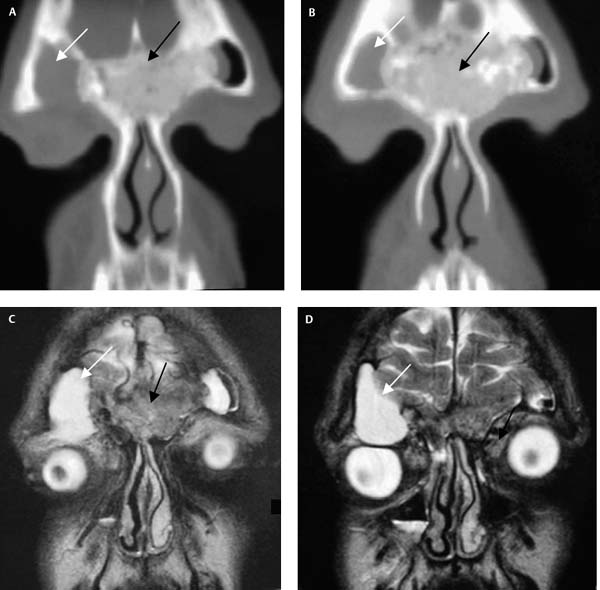
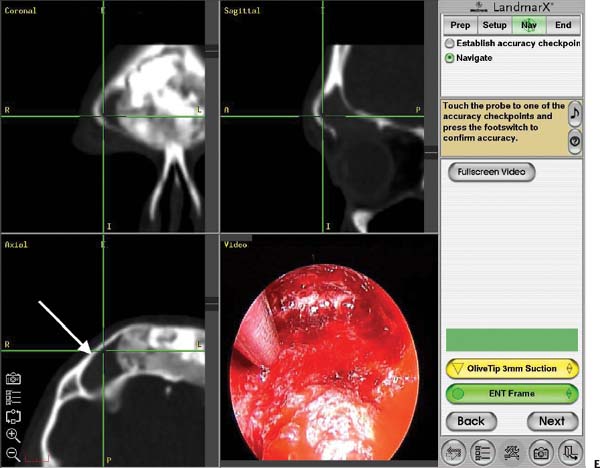
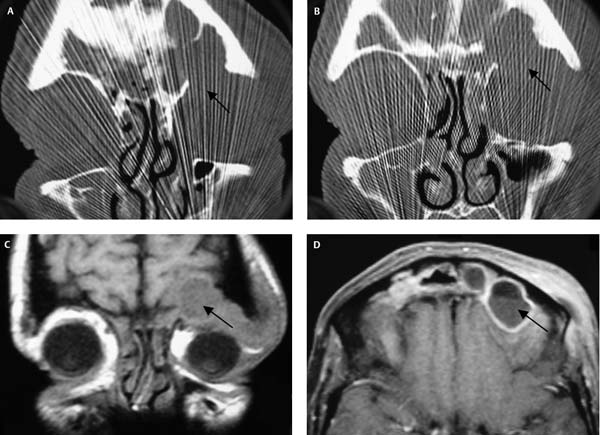
9 Chronic frontal sinusitis has challenged surgeons for many years. In the past, frontal sinus obliteration through an osteoplastic flap (OPF) approach has been the gold standard for the management of recalcitrant frontal sinusitis.1–3 Other external procedures such as frontoethmoidectomy have fallen into disfavor due to a failure rate of around 30%.3,4 OPF and obliteration has a reported failure rate of around 10% but has a significant complication rate of around 65%.3,5,6 The complications include cerebrospinal fluid (CSF) leak, frontal bossing, supraorbital neuralgia, chronic sepsis, mucocele formation, and chronic frontal bone osteitis with loss of the frontal sinus bone flap.1–3,6 In recent years the modified endoscopic Lothrop (MEL) procedure—otherwise known as the Draf 3 or frontal drillout—has been proposed as an alternative to the OPF with obliteration.7–20 The MEL procedure is based on the technique originally described by Lothrop in 1914.21 This technique involves removal of the upper portion of the septum, the floor of the frontal sinus, and the intersinus septum. Removal of the floor is accomplished with the aid of a small external incision (similar to a Lynch incision) which creates a window through which the drill can be observed. Although this procedure was successful in 29 out of 30 patients, the technique was considered too technically difficult for most surgeons to master and it was not until Draf in 19917 and Gross in 19958,9 published series of patients using a modified version of the technique that interest was renewed. The major modification to the Lothrop technique is the absence of an external incision with the entire procedure performed endoscopically. The MEL can be used as an alternative to OPF with obliteration with recent publications12 showing excellent short-term success rates with minimal complications. The indications for the MEL procedure should be the same as the indications for an OPF with obliteration and these are detailed in the following text.12 The MEL procedure is indicated in patients who have failed standard endoscopic sinus surgery (ESS) techniques.12 These include clearance of the frontal recess and removal of cells obstructing the frontal ostium.20 In those very rare cases where patients have a very large cell obstructing the frontal ostium (i.e., a type 4 cell that extends into the frontal sinus by more than 50% of the vertical height of the frontal sinus), management may include a primary MEL procedure if the surgeon is certain that the cell is causing significant obstruction and that it is not possible to remove the cell with standard ESS techniques discussed later.20 All patients should have had a standard ESS approach with an attempt to remove obstructing cells from the frontal ostium and improve the drainage of the frontal sinus. It is only if such techniques fail that the MEL procedure should be considered for removal of a type 4 cell.20 In Fig. 9.1 the patient had undergone five previous standard ESS procedures and was still left with significant frontal sinus symptoms and a large type 4 cell obstructing the frontal sinus ostium. This patient underwent a successful MEL procedure. Significant new bone formation in the regions of the frontal recess after ESS indicates probable osteitis. This can be difficult to manage with standard ESS techniques. The neo- osteogenesis results in a narrowed frontal sinus openings and increases vascularity in the region. Surgery to widen such narrowed ostia will often result in significant bleeding and loss of mucosa. The healing process may produce significant restenosis as ongoing low-grade osteitis and sinusitis continue to stimulate new bone formation and fibrosis. The MEL procedure overcomes this problem by drilling away a significant amount of the osteitic bone and creates the largest possible opening in the frontal sinuses. Even if some degree of restenosis occurs in the MEL procedure, this should not affect the function of the frontal sinuses.22 Recent work done on the MEL procedure in our animal laboratory on the presence of neo-osteogenesis in a newly created frontal ostium suggests that most frontal ostia will restenose by an average of a third.23,24 This figure was not affected by the presence of neoosteogenesis which was found in 56% of animals. In addition, this restenosis did not affect the mucociliary drainage of the frontal sinuses as measured by the clearance of radioisotope from the frontal sinuses.22 Figure 9.2 shows a patient with significant neo-osteogenesis in the left frontal ostium. This patient had undergone six previous standard ESS procedures in an attempt to maintain a patent left frontal ostium. In all cases the restenosis was rapid and associated with a return of frontal sinus symptoms. Fig. 9.1 (A–D) CT scans of a patient with a type 4 cell (white arrow) who had undergone multiple previous ESS procedures. (D) Note on the axial scan the significantly narrowed frontal sinus drainage pathway (black arrow) caused by the type 4 cell (white arrow). In patients who have previously undergone multiple ESS procedures one will often find that the middle turbinates have been resected subtotally.12 In this scenario the middle turbinate remnant may lateralize and become adhesive to the lateral nasal wall in the frontal recess. This results in significant narrowing of the frontal drainage pathway and, in some instances, complete obstruction of the frontal ostium (Fig. 9.3). Standard ESS techniques will usually fail to recreate a mucosalized opening of sufficient diameter into the frontal sinuses and a MEL procedure or OPF with obliteration should be considered. If the disease process results in bony erosion of either the posterior wall or floor of the frontal sinus, the mucosa of the sinus becomes adherent onto the dura or orbital periosteum.18 OPF with obliteration becomes extremely difficult in these patients as the mucosa cannot be safely or completely removed from the dura or orbital periosteum and a recurrence of a mucocele is likely if the sinus is obliterated. These patients often have long-term severe chronic sinusitis and may have disease with a high incidence of recurrence such as fungal sinus disease. It is important to keep the frontal ostia open as obstruction of the frontal ostium may lead to either orbital or intracranial complications (Fig. 9.4).18 Fig. 9.2 (A,B) Coronal CT scans of a patient with multiple previous ESS procedures with neo-osteogenesis in the left frontal recess (black arrow) with associated chronic frontal sinusitis. Fig. 9.3 (A–C) This patient has undergone previous middle turbinate resection and the stump (black arrow) has lateralized blocking the frontal ostium. (C) In addition, new bone formation can be seen above the middle turbinate. Fig. 9.4 (A–D) This patient with chronic frontal sinusitis with loss of the roof of the orbit and loss of the posterior table of the frontal sinus developed an abscess (black arrow) with associated cellulitis around the orbit and depression of the left globe. (C,D) In addition, this abscess had eroded the posterior table of the frontal sinus and compressed the anterior cerebral hemisphere. This was managed by a MEL procedure with the creation of a large communal frontal ostium. Frontal sinus obliteration has been the gold standard for the management of recalcitrant frontal sinusitis for many years. However, severe mucosal disease such as that seen in patients with Samter’s triad (aspirin sensitivity, asthma, and nasal polyposis), allergic fungal sinusitis, and aggressive recurrent nasal polyposis is best managed endoscopically rather than with an OPF and obliteration.14–18 There is now widespread agreement in the literature that the MEL procedure should be the operation of first choice in this difficult group of patients.14–18 One of the major problems with OPF and obliteration is the tendency for the adipose tissue placed in the frontal sinuses to resorb. Weber et al.,14 in a large study of 82 patients who underwent OPF and obliteration, showed that the majority of patients had less than 20% of the sinus obliterated after a median of 15.4 months.14 In this patient group who aggressively form polyps, such space can be rapidly filled by even the smallest amount of residual mucosa inadvertently left in the frontal sinuses. In the postoperative period this group tends to develop thick inspissated mucus among the regrowing polyps. Without a wide opening or marsupialization of the affected sinus, this mucus cannot be removed in the office. The inability to pass a large suction through the sinus ostium into the sinus cavity prevents this very tenacious mucus from being removed. A course of systemic prednisolone may loosen the mucus and lessen its tenacity facilitating its removal. Clearance of this toxic material allows shrinkage of the polyps and reestablishment of the nasal airway with control of polyp growth. In most patients it is a relatively simple procedure to create a wide maxillary antrostomy, completely remove all ethmoid cells, and open widely the anterior face of the sphenoid sinus. However, the frontal sinuses are extremely difficult to access without the wide opening that the MEL procedure creates. Naturally sized frontal ostia tend to be quickly obstructed by thickened mucosa and this results in a buildup of thick mucus in the frontal sinuses which may be resistant to aggressive prednisolone therapy and attempted suction clearance. One of the difficulties with OPF and obliteration in this group of patients is when there is loss of bone over the orbit or dura. Due to the aggressive nature of the polyposis and in some cases aggravated by repeated surgeries, there may be loss of the anterior or posterior bony frontal sinus wall. This brings the mucocele lining in direct contact with the orbital periosteum and/or dura and makes it impossible to remove all the mucosa from these structures without resection.15 Even microscopic mucosal remnants left on the periosteum or dura will lead to the development of a mucocele in the obliterated cavity (Fig. 9.5). Fig. 9.5 (A) CT scan shows frontal sinus opacification with an orbital roof dehiscence (white arrow). (B) T2-weighted MRI shows a frontal sinus mucocele (broken white arrow). (C) CT scan shows both orbital and posterior table dehiscences where the mucocele is in contact with the orbital periosteum and the dura. (D) Axial CT scan shows previous osteotomies in the anterior table of the frontal sinus and MRI scan (E) shows the frontal sinus mucocele (broken white arrow) and the extensive nasal polyp formation in the nasal cavity (solid white arrow). Another contraindication to OPF and obliteration is when the patient has very large pneumatized frontal sinuses.15,18 In these patients it is extremely difficult to eradicate all the mucosa from the lateral and posterior recesses of the frontal sinus and this residual mucosa will form mucoceles which, if left untreated, will erode the bony walls of the sinus and may well give rise to either intracranial or orbital complications (Fig. 9.6). Mucoceles that form in a previously obliterated frontal sinus can be treated by an MEL procedure.13,14,18 The mucocele should be sufficiently large that it can be accessed through the frontal recess and marsupialized into the frontal recess (Fig. 9.6).13,18 Mucoceles confined to the far lateral aspect of previously well-pneumatized sinuses may be difficult to reach and, if the intervening space is filled with scar tissue, may be difficult to keep open postoperatively. Patients who have previously undergone an OPF with obliteration often present with frontal pain and it can be quite difficult to ascertain whether their pain is from a frontal sinus mucocele or from other causes. All these patients undergo magnetic resonance imaging (MRI) to ensure that there is indeed a mucocele present. If there is no mucocele present surgery is usually not offered and the patient is given treatment for neuralgic pain or myofascial pain syndrome. To assess if the pain is neuralgic or myofascial in origin, a trial of low dose amitriptyline (10 mg per night) is prescribed for 6 weeks. If neuralgia or myofascial pain syndrome is contributing to the patient’s pain, there should be an improvement in symptoms on this treatment.19 Most patients will also undergo radioisotope screening to exclude osteomyelitis of the previous bone flap. If the radioisotope scan is positive, consideration may have to be given to removal of this bone flap. The MEL procedure is useful for the removal of benign tumors from the frontal sinuses. These tumors include osteomas and inverting papillomas. Fairly large osteomas can be removed through the MEL opening.12,15,18 Figure 9.7 illustrates a patient with a large frontal osteoma which has blocked the pathway of the right frontal sinus and resulted in the formation of a large lateral mucocele. This mucocele had eroded the bone over the roof of the orbit with the lining of the mucocele in contact with a large proportion of the orbital periosteum (Fig. 9.7). Fig. 9.6 This patient has extensive pneumatization of the frontal sinuses. (A–C) OPF with obliteration failed with resultant superior and lateral mucocele formation (black arrows). This was addressed with a MEL. (D) The postoperative picture at 3 years is presented, with black arrow indicating one of the opened mucocoeles. The patient underwent a MEL procedure with removal of 90% of the osteoma and drainage of the mucocele. A free mucosal graft was placed on the circumferential raw area created after removal of the osteoma. The patient is now 3 years postsurgery and has a nicely healed and patent right frontal sinus with free drainage of the lateral mucocele into the nose (Fig. 9.8). The MEL procedure is also suitable for removing inverting papilloma from the frontal sinus.12,15,20 Figure 9.9 shows a recurrent inverting papilloma entering the frontal sinus on the left. This had previously been removed via a lateral rhinotomy procedure. The tumor is seen in the left frontal recess and sinus. The entire tumor was removed after a MEL procedure until direct visualization. As a large area of frontal sinus mucosa was removed in association with the tumor, a free mucosal graft was placed. Figure 9.10 shows the patient 1 year after the procedure. There still remains a little edema of the frontal ostium. Biopsies were negative for recurrence. Excellent visualization of the site of the tumor is provided by the large frontal ostium and recurrences can be detected early (Fig. 9.10). Fig. 9.7 (A,B) CT scans and (C,D) MRI scans (T2-weighted) showing the osteoma (marked with a black arrow) and the right-sided lateral mucocele (marked with white arrow) with associated proptosis and inferolateral displacement of the eye. (B) Intraoperative images seen on the image-guidance system of the large frontal osteoma (white arrow) occupying the vast majority of the frontal sinuses. The laterally based mucocele is under the crosshairs which are formed from the tip of the suction.
Extended Approaches to the
Frontal Sinus: The Modified Endoscopic
Lothrop Procedure
 Indications for Modified Endoscopic Lothrop Procedure
Indications for Modified Endoscopic Lothrop Procedure
Failed Endoscopic Sinus Surgery
Neo-Osteogenesis in the Frontal Recess and Frontal Ostium
Frontal Recess Adhesions
Disease Processes with Resultant Loss of the Posterior Wall or Floor of the Frontal Sinus18

Failed Previous OPF with Obliteration with Mucocele Formation13
Tumor Removal from the Frontal Sinus (Video 43)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


