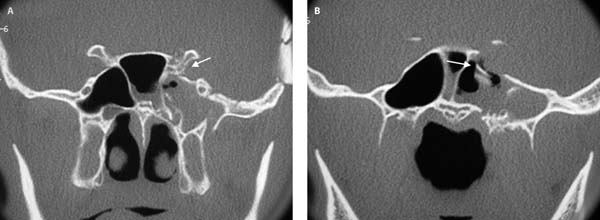
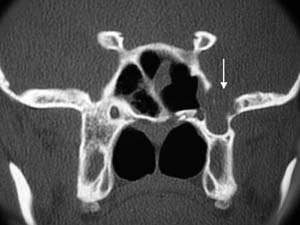
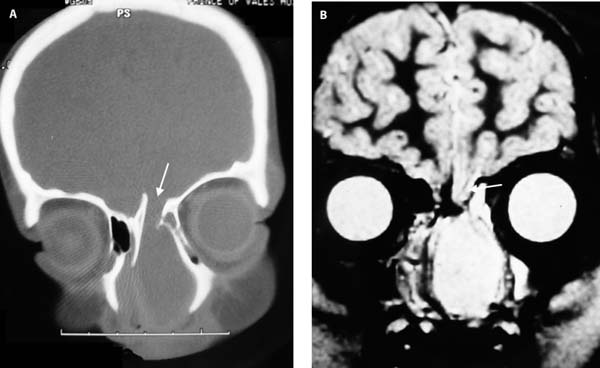
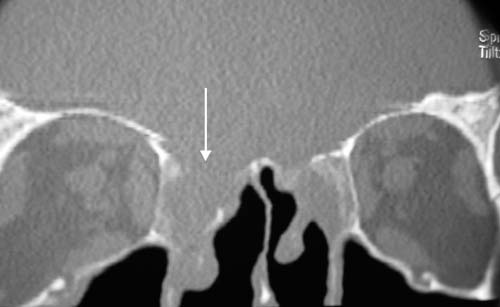
12 The traditional management of anterior skull base cerebrospinal fluid (CSF) leaks was via an anterior craniotomy and intracranial repair of the leak. This was usually done by elevating the frontal lobes in the region of the suspected site of the leak and laying a sheet of fascia lata over this area. The success rate of this technique was around 70% but usually left the patient with some loss of smell. In addition, frontal lobe retraction is associated with the risk of postoperative epilepsy. In the late 1980s and early 1990s endoscopic closure of CSF leaks was first reported. Since then many published series have reported success rates of above 90%.1–3 This high success rate and the very low associated morbidity are the major advantages of the endoscopic technique.1 A variety of materials have been used to close these leaks.3,4 Free mucosal grafts, pedicled mucosal grafts, fat, fascia, muscle, and synthetic materials such as hydroxyapatite have all been described with similar success rates.3,4 In a recent review Hegazy et al.3 felt that the type of material did not appear to make a significant difference to the success rate of the closure. Although this may indeed be the case in small CSF leaks, the purely onlay technique may not be as suitable for larger leaks.3,4 The techniques proposed in this chapter (the bath-plug closure and fascia lata repair) have been used in a large series of patients and have been found to be reliable for both large and small leaks.5,6 In our experience if the onlay technique alone is used for medium or large defects with a free flow of CSF, the graft tends to be pushed away from the skull base and hence from the dural defect and the flow of CSF resumes. Although the leak may be sealed at the end of the operation, coughing or straining in the postoperative period may raise the CSF pressure sufficiently to cause the leak to start again. An analogy of patching these high flow CSF leaks with onlay technique alone is trying to patch a plastic bag of water by applying a patch to the outside of the bag.5,6 The bath-plug technique allows the plug to be placed on the inside of the bag and uses the pressure from the water to increase the seal on the plug. The other techniques presented (underlay alone or underlay and onlay fascia grafting) and the indications for these techniques also overcome this problem of the CSF pressure pushing the graft away from the skull base because the fascia is placed intracranially and the CSF pressure again helps create the seal. This chapter does not attempt to describe all the alternative techniques but will concentrate on the bath-plug and underlay fascia techniques as we have considerable experience in a wide variety of situations with these techniques and have found them to be both versatile and reliable.5,6 Anterior skull base CSF leaks can be divided into four broad categories according to their etiology. In a recent large series from our department, there was a fairly even spread between leak types: skull base trauma, spontaneous, meningoencephaloceles, and iatrogenic leaks. Traumatic CSF leaks usually follow an anterior skull base fracture. The initial management is conservative as most of these leaks will cease within 10 days of the injury. However, leaks that persist longer than 10 days should be closed. One of the major causes of continued CSF leakage is rotation of a bony spicule which continues to hold the edges of the torn dura apart as demonstrated in this traumatic CSF leak of the sphenoid in Fig. 12.1. If the bone fragment is freely mobile, then this should be removed at the time of closure of the leak. More common than traumatic CSF leaks of the sphenoid are those seen in the fovea ethmoidalis or at the fovea ethmoidalis-olfactory fossa junction (Fig. 12.2). Less frequent are fractures in the posterior table of the frontal sinus. Fortunately these leaks from the base of skull fractures rarely need closure but if they persist, access is usually only possible with an endoscopic modified Lothrop procedure or an osteoplastic flap. The endoscopic modified Lothrop procedure allows most of the posterior table of the frontal sinus to be accessed and the CSF leak can be closed under direct visualization (Fig. 12.3). The reason that skull base fractures tend to heal spontaneously as opposed to injuries created during endoscopic sinus surgery (ESS) is that, although the dura is torn, there is usually no bony displacement so there is no prolapse of the torn dura preventing sealing. Where there is bony fragment displacement, surgical closure of the CSF leak should be done expeditiously and not watched expectantly. CSF leaks during ESS almost always have associated bony loss and dural prolapse so all are closed expeditiously without any conservative management prior to surgery. Fig. 12.1 (A,B) CT scans of patient with a fracture through the clinoid (A, white arrow) with a displaced bony fragment (B, white arrow) and a CSF leak. Note the fluid level in the sphenoid. Spontaneous CSF leaks are usually seen either in the cribriform plate or lateral wall of the sphenoid sinus. Cribriform fossa leaks often result from a dilation of the dural sheath around the olfactory fibers. A small prolapse of dura may result which may leak CSF (Fig. 12.4). Spontaneous CSF leaks in the sphenoid sinus are usually seen in well-pneumatized sphenoid sinuses where the sinus pneumatizes into the sphenoid wing under the maxillary nerve. This brings this region of the sphenoid sinus in contact with the temporal lobe region of the middle cranial fossa with only thin bone separating the two. One theory as to why the skull base becomes eroded in this region is that arachnoid granulations in the floor of the middle cranial fossa often do not have a venous connection. When these arachnoid sacks fill with CSF and pulsate they may gradually erode the bone eventually leading to a prolapse of dura and arachnoid into the sphenoid with an associated leak.7–10 In addition it is thought that several of these patients may have undiagnosed benign raised intracranial pressure as part of the etiology. In Fig. 12.5 a defect is seen in this lateral aspect of this well-pneumatized sphenoid with associated opacity (prolapsing meninges and CSF). Fig. 12.2 CT scan of patient following head trauma with a fracture through the fovea ethmoidalis (white arrow) and with an associated CSF leak. Note the fluid level in the adjacent ethmoid sinus. Fig. 12.3 CT scan of a patient with a fracture through the posterior table (white arrow) of the frontal sinus with an associated CSF leak. Fig. 12.4 A coronal CT illustrating a triangular dilation of the cribriform plate around an olfactory neuron (confirmed at surgery). Fig. 12.5 Defect in left lateral wing of sphenoid with prolapse of dura through the defect. Meningoencephaloceles may either be spontaneous (congenital or acquired) or associated with a previous traumatic event. Congenital meningoencephaloceles usually present within the first few years of life. The meningoencephalocele consists of meninges and dura containing CSF with a variable amount of brain tissue prolapsing through the skull base defect into the nasal cavity or sinuses. The brain tissue within the encephalocele is usually nonfunctional and is usually resected as the first step of the procedure. Posttraumatic meningoencephaloceles often have a funnel-shaped defect in the skull base and this needs to be recognized during the repair process as this affects the ability of the surgeon to properly visualize the edges of the bony skull base defect as well as the intracranial cavity. The funnel-shaped bony defect is caused by the intracranial contents protruding through the defect and pushing the edges of the bony defect downward into the nasal cavity/sinuses (Fig. 12.6). Iatrogenic leaks will frequently be seen on the lateral wall of the olfactory fossa and fovea ethmoidalis. The lateral wall of the olfactory fossa forms the medial limit of the dissection of the frontal recess. It can be very thin varying from 0.1 to 1 mm in thickness and is perforated by the anterior ethmoidal artery. Damage to this lateral wall of the olfactory fossa may occur if the dissecting instruments are turned medially during surgery in this region. Laceration of the anterior ethmoidal artery with bleeding may prompt the use of diathermy in an attempt to obtain hemostasis. Unipolar diathermy, if used to cauterize a bleeding vessel, may burn through the bone and dura causing a CSF leak. The remaining skull base (fovea ethmoidalis) may be damaged if the surgeon loses orientation and fails to recognize that the dissection has reached the skull base. If cells are assumed to be present on the skull base, an attempt to remove these “cells” may damage the skull base with an associated CSF leak (Fig. 12.7). Generally these leaks are readily apparent at the time of surgery and can be fixed with the bath-plug technique described. Fig. 12.6 (A) CT shows the bevelling of the edges of the meningoencephalocele (white arrow). (B) Three-dimensional reconstruction also illustrates the funnel shape of the skull base defect through which the meningoencephalocele protrudes (black arrow). Fig. 12.7 Intraoperative iatrogenic injury to the anterior fovea ethmoi dalis (white arrow) on the right side. This is performed if the patient presents with a suspected CSF leak. Intraoperative CSF leaks should be dealt with at the time of the surgery. The most reliable method of confirming a CSF leak is to test the clear watery secretions from the nose for β2 transferrin (β2 transferrin is only present in CSF).4,5,7,11 Once the CSF leak has been confirmed, the site of the leak is sought by performing a high resolution fine cut computed tomography (CT) scan of the sinuses.5,11 On this scan dehiscences of the anterior skull base are sought. Depending on the suspected cause, different areas in the anterior skull base are thoroughly scrutinized for bony defects. An additional clue may be the presence of fluid in the sinuses indicating that the leak is in the region of the opacified sinuses. Patients with spontaneous CSF leaks without evidence of any bony dehiscences on CT scan and without any opacification of any sinuses should have the cribriform plate region carefully examined intraoperatively for the CSF leak as it has been our experience that this is the most likely source of the leak (Fig. 12.4). If the site of the leak is not apparent on the CT scan a high resolution T2-weighted magnetic resonance imaging (MRI) scan may allow visualization of fluid within the sinuses and, if the patient is leaking at the time of the MRI, it may allow identification of the site of the leak.5,11 All patients with suspected meningoceles or meningoencephaloceles should have a preoperative MRI. This allows brain tissue within the meningoencephalocele to be identified and the opinion of the neurosurgeon should be sought whether the resection of this tissue transnasally is considered reasonable and safe (Fig. 12.8). Although in the past there have been other investigations used to identify CSF leaks, the discussed investigations are the only ones recommended. Intrathecal contrast does not improve the sensitivity of the detection of the site of a CSF leak. Intrathecal radioisotope may confirm the presence of CSF in the nasal cavity, but does not add additional information to that obtained by a positive β2 transferrin test.3 If the site of the leak is not able to be determined with the previously listed investigations, the patient is taken to theater and intrathecal fluorescein is injected into the CSF space and the site of the leak sought while the patient in under general anesthetic.5,11,12 Fig. 12.8 (A) A CT scan showing the skull base defect of a congenital meningoencephalocele (white arrow) whereas (B) is a T2-weighted MRI showing a large CSF filled sac filling the nasal cavity with an associated stalk of brain tissue prolapsing through the skull base defect (white arrow). This meningoencephalocele was managed endoscopically.
Cerebrospinal Fluid Leak Closure
 Etiology of Cerebrospinal Fluid Leaks
Etiology of Cerebrospinal Fluid Leaks
Traumatic Cerebrospinal Fluid Leaks
Spontaneous Cerebrospinal Fluid Leaks


Meningoencephaloceles with Associated Cerebrospinal Fluid Leaks
Iatrogenic Cerebrospinal Fluid Leaks

 Preoperative Assessment
Preoperative Assessment

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


