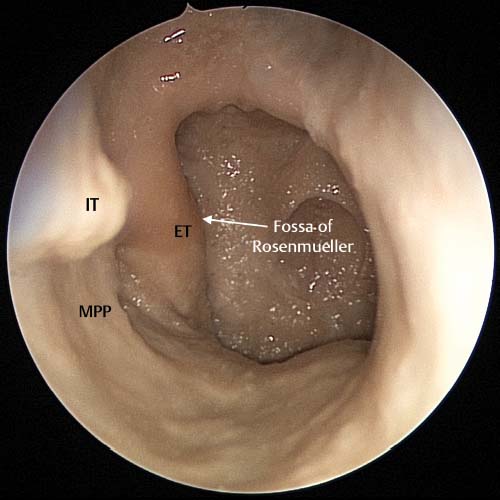
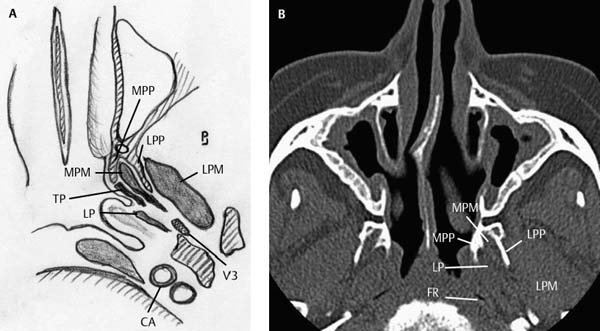
17 The most common tumor of the postnasal space is nasopharyngeal carcinoma. Fortunately, these tumors are radiosensitive and there is seldom a need for surgical excision. In rare cases nasopharyngeal carcinoma that has recurred despite repeated radiotherapy may need surgical excision. In these cases recurrent tumor is best managed by external procedures such as the maxillary swing technique, transmaxillary approach, facial translocation, transcervical-mandibulo-palatal, infratemporal fossa, and lateral infratemporal middle fossa.1–7 These recurrent carcinomas are usually only suitable for endoscopic excision if the tumor has not extensively infiltrated the surrounding structures.8,9 When a patient has previously undergone radiotherapy there is usually significant fibrosis which will often obliterate surgical planes making surgical dissection very difficult. If the tumor significantly infiltrates the surrounding tissue, they are removed by traditional techniques with appropriate vascular control. However, there are a small number of rare benign and malignant tumors that occur in the postnasal space and Eustachian tube (ET) that are nonresponsive to radiotherapy and are best treated by primary surgical excision. Examples of these are the minor salivary gland tumors (benign and malignant), malignant melanomas, and juvenile angiofibromas. These tumors usually have an identifiable plane and a pushing front which will allow identification of the surgical plane and can be excised endoscopically even if there is limited extension into the parapharyngeal space. Endoscopic resection is appealing as it allows a complete resection of the tumor with minimal morbidity in contrast to the external approaches that have significant associated morbidity. To perform endoscopic resections in this region, a detailed knowledge of the anatomy is necessary. The key anatomical landmark is the medial pterygoid plate. The relationship of the medial pterygoid plate, medial pterygoid muscle, tensor palatini, levator palatini, and ET needs to be understood. If the postnasal space is viewed endoscopically the medial pterygoid plate, ET, and fossa of Rosenmüller can be clearly seen (Fig. 17.1). To access the ET, the medial pterygoid plate needs to be removed and the underlying medial pterygoid muscle exposed (Figs. 17.2 and 17.3). Note how the tensor palatine muscle forms a natural surgical plane as it attaches to the anterior aspect of the ET (Fig. 17.4). Inferiorly, the ET lies on the levator palatini muscle as it moves laterally to its attachment to the skull base (Fig. 17.4). The lateral pterygoid muscle attaches to the lateral aspect of the lateral pterygoid plate and is usually not seen in the dissection unless there is significant infratemporal fossa extension of the tumor. Just anterior to where the ET attaches to the skull base, the mandibular branch (V3) of the trigeminal nerve is seen (Fig. 17.5). Directly posterior to V3, in the apex of the fossa of Rosenmüller, the internal carotid artery can be seen (Figs. 17.2 and 17.5). The nose is prepared in the standard fashion. A pterygopalatine fossa block is placed through the mouth and greater palatine canal into the pterygopalatine fossa. The first step for this surgery is to remove the posterior half of the inferior turbinate. A large middle meatal antrostomy is done with exposure of the posterior wall of the maxillary sinus (Fig. 17.6). The middle meatal antrostomy is taken down to the floor of the nose and the mucosa over the medial pterygoid plate is elevated (Fig. 17.7). To access this region a two-surgeon approach is advocated. The use of both nostrils allows greater angulation and, if significant bleeding occurs, clearance of blood, so that surgery can continue. The first step is to raise a Hadad pedicled septal flap on the contralateral side (see Chapter 20) to the tumor. The posterior aspect of the tumor side of the septum is mobilized by making superior and inferior horizontal incisions then by joining them with a posterior vertical incision creating an anterior pedicled flap. This flap is now rotated anteriorly and fixed with a 30 Vicryl plication suture (Ethicon, Somerville, NJ). Additionally, to help the passage of instruments in and out of the nose during the two-surgeon approach, a 5–6 × 1.5 cm piece of thin silastic can be placed across the columella and the limbs pushed down each nostril and sutured with silk plication suture placed in the same manner as the septal suture. This results in the removal of the posterior half of the septum and gives great access to both sides of the postnasal space for the two-surgeon approach. This access allows the ET and tumor to be placed on traction when dissection is being performed in the lateral regions of the postnasal space which increases the safety by pulling the ET and tumor medially lessening the risk to the carotid artery (Fig. 17.8). Fig. 17.1 Cadaveric image taken of the right postnasal space showing the posterior attachment of the inferior turbinate (IT) to the vertical portion of the palatine bone. The right medial pterygoid plate (MPP) can be seen as a mucosal prominence directly anterior to the eustachian tube (ET). The fossa of Rosenmüller can be seen behind the ET. The next step is to remove the bone of the medial pterygoid plate using a Stylus skull base curved diamond burr (Medtronic ENT, Jacksonville, FL; Fig. 17.3). As the bone is removed the descending palatine artery is exposed. This needs to be cauterized using the suction bipolar then divided. This gives the surgeon access to the medial pterygoid muscle and the lateral pterygoid plate. The medial pterygoid muscle is surrounded by a dense venous plexus and sharp dissection of this muscle can result in significant venous bleeding. We prefer to use the coblation wand to remove this muscle as this can be done without significant bleeding. There is a natural surgical plane anterior to the ET. This is formed by the cartilaginous anterior aspect of the ET and the attached fibrous aponeurosis of the tensor palatini. If the aponeurosis is followed inferiorly the tensor palatini muscle fibers can be seen (Fig. 17.9). The surgical removal of the medial pterygoid plate and partial removal of the medial pterygoid muscle with establishment of the anterior surgical plane can also be appreciated (Fig. 17.10). The next step is to release the ET inferiorly and posteriorly (Fig. 17.11). These horizontal and posterior incisions are made with the coblation wand to minimize bleeding. The horizontal incision cuts through the tensor and levator palatini muscles and further dissection enters the parapharyngeal space. The dissection is continued laterally directly under the ET thereby mobilizing the ET from the parapharyngeal space. If the fossa of Rosenmüller is to be included in the resection the posterior incision is made onto the longus capitis muscle. The surgical plane is anterior to the fascia of this muscle. If the plane is deep to these muscles the carotid artery and jugular vein are at increased risk in the most lateral extent of the fossa (Fig. 17.5). Fig. 17.2 In diagram (A) and axial CT scan (B), the medial pterygoid plate (MPP) and lateral pterygoid plate (LPP) are identified. The medial pterygoid muscle (MPM) is seen between these two plates. The lateral pterygoid muscle (LPM) is seen lateral to the LPP. The levator palatini (LP) attaches to the medial aspect of the Eustachian tube (ET) while the tensor palatini (TP) lies below the ET. The fossa of Rosenmüller (FR) forms most of the posterior boundary of the ET. Note the relationship of the mandibular nerve (V3) and the carotid artery (CA) to the apex of the fossa of Rosenmüller and V3.
Endoscopic Resection of the
Eustachian Tube and Postnasal Space
 Anatomy
Anatomy
 Surgical Approach (Video 50)
Surgical Approach (Video 50)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


