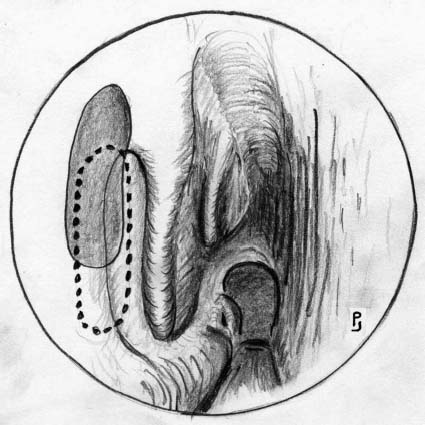
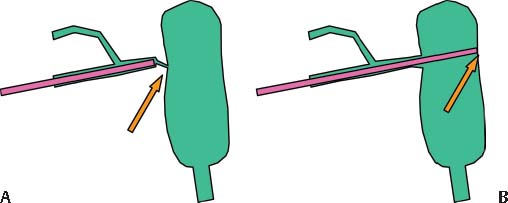
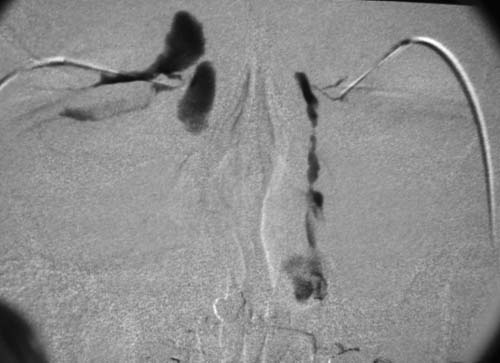
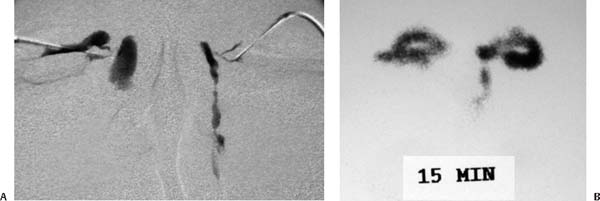
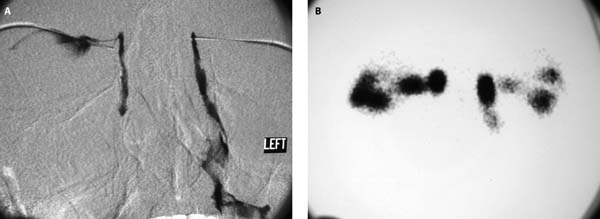
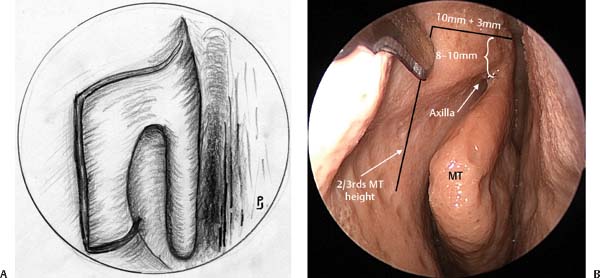
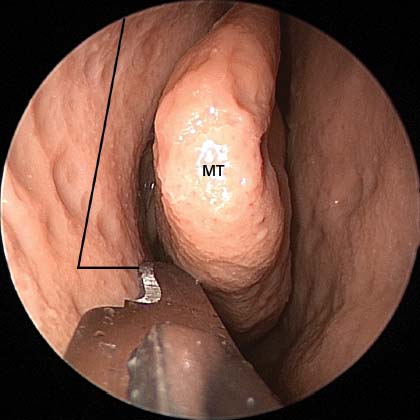
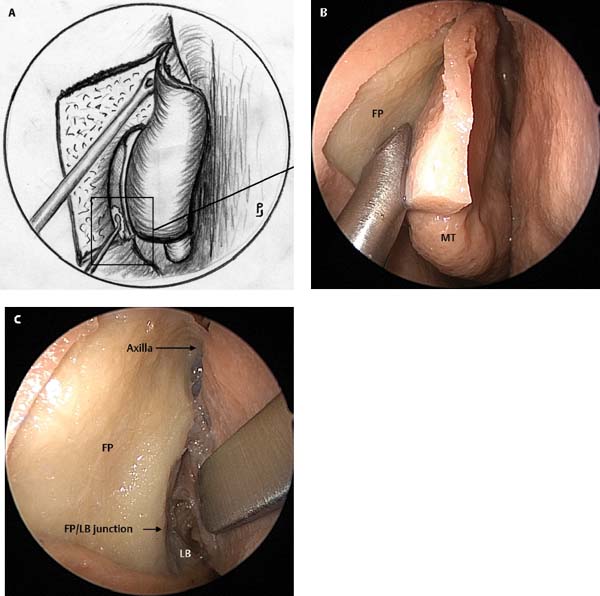
11 Endoscopic dacryocystorhinostomy (DCR) was initially described by Caldwell in the 19th century.1 However, it fell into disrepute as surgeons experienced problems with visualization of the surgical site. In the early 20th century, Toti described the external DCR procedure and, with a few modifications, this procedure remains largely unchanged from those early descriptions.2 As the technique has developed, so the success rate for the external procedure has improved until today, in the hands of properly trained oculoplastic surgeons, success rates of between 90 and 95% can be expected.3 As endoscopic sinus surgery (ESS) became popular in the late 1980s, there was renewed interest in endoscopic DCR with the initial descriptions having appeared in the late 1980s and early 1990s.4–6 As could be expected of a new and developing technique, the initial success rates were lower than that of external DCR and varied between 65 and 90%.4–6 Laser endoscopic DCR was promoted in the mid 1990s but success rates were disappointing and tended to be at the lower end of the spectrum (around 75%).7–9 This was probably due to the technique creating only a small opening into the posterior inferior lacrimal sac through the thin lacrimal bone. It is well recognized within the literature on external DCR that a small ostium does not achieve the same success rates as a large opening of the lacrimal sac.10 The original endoscopic DCR technique was described as follows: a mucosal flap anterior to the middle turbinate was raised and the junction between the lacrimal bone and frontal process of maxilla established. A Hajek Koffler punch was used to remove what bone one could over the lacrimal sac.4 In the early 1990s, I reviewed my own results with this technique and found a disappointing long-term patency rate of only 83%.11 On review of the literature on external DCR, the critical factor necessary for achieving the 90 to 95% success rate was a wide bone removal so that the entire lacrimal sac was exposed.10,12–14 Following this the mucosa of the lacrimal sac and nasal mucosa were anastomosed with sutures allowing primary intention healing without significant granulation. This raised the question—could the external DCR technique be duplicated by a similar intranasal technique? If this were to be done the first step was to define the intranasal anatomy of the lacrimal sac.13 The early descriptions of the intranasal anatomy of the sac placed the sac anterior to the middle turbinate with minimal extension of the sac above the insertion of the middle turbinate on the lateral nasal wall (the so-called axilla of the middle turbinate as it resembles an armpit).13,15,16 To investigate the precise location of the sac, a series of computed tomography (CT) dacryocystograms (DCGs) in patients undergoing DCR were performed and the relationship of the lacrimal sac and the axilla of the middle turbinate evaluated.13 This study showed that the anatomy of the sac on the lateral nasal wall was significantly different to what had been previously described in the literature (Fig. 11.1). The sac was not only anterior to the middle turbinate but a significant proportion was located above the axilla of the middle turbinate. On average the sac extended 8 mm above the axilla of the middle turbinate.13 Therefore, if the external DCR principles were to be applied to endoscopic DCR, a different technique was required. This led to the design of a new technique (powered endoscopic DCR) which is presented in the following text.14,17,18 Fig. 11.1 The broken line indicates the location of the sac prior to our studies on the intranasal anatomy of the lacrimal sac. The shaded area is the actual intranasal position of the lacrimal sac on the lateral nasal wall. Note it extends between 8 and 10 mm above the axilla of the middle turbinate. In epiphora caused by nasolacrimal duct obstruction (NLDO), tears will frequently run down the cheek. This is more noticeable in conditions that stimulate tear formation such as walking in a cold wind. During examination, the position and size of the puncta should be assessed. The lid laxity and positioning of the puncta in the tear lake should be determined. To assess the patency of the inferior, superior, and common canaliculi, the upper lacrimal system should be probed (Fig. 11.2). The punctum is dilated with a punctum dilator. A Bowman’s lacrimal probe is then used to probe the inferior canaliculus and common canaliculus. Fig. 11.2 (A) A soft stop is felt as the probe rests against a common canaliculus stricture or obstruction whereas in (B) a hard stop is felt as the probe comes to rest against the bone encasing the lacrimal sac. Differentiating between a soft and a hard stop on probing helps assess the patency of the canalicular system. If a common canaliculus stricture is present, it should be diagnosed preoperatively so appropriate steps can be taken to correct it during surgery. Additionally, the patient can be informed that the likelihood of a successful procedure is significantly less than is the case with a DCR performed for nasolacrimal duct obstruction. Syringing of the lacrimal system will also help assess the patency of the nasolacrimal system. In NLDO there will be significant reflux through the upper punctum with no saline penetration into the nose. In partial NLDO there will be reflux through the upper punctum with saline penetration into the nose but only with increased syringing pressure. Penetration into the nasal cavity without reflux through the upper punctum indicates a patent (but not necessarily functional) lacrimal system. It is sometimes confusing to determine exactly where the saline is refluxing as some may reflux from the punctum that has been injected, or from the other punctum or a combination. Rigid nasal endoscopy is performed on all patients presenting with epiphora. A significant proportion (15%) of patients require surgery for nasal pathology at the same time as the DCR. Mostly this is for associated chronic sinusitis. All patients need to be questioned regarding nasal symptoms and endoscopy performed to assess the nasal cavity. If there is evidence of nasal and sinus disease, appropriate investigations are performed and treatment instituted. If medical therapy fails to resolve the problem, surgery is performed at the same time as the DCR. We routinely perform a DCG to assess the patency of the canalicular system and penetration of dye into the nasolacrimal sac.17 If the patient has a hard stop on probing with a blocked system on syringing, this investigation can be omitted. Filling of the sac but failure of the dye to penetrate the nasal cavity confirms the diagnosis of NLDO (Fig. 11.3). Fig. 11.3 Right nasolacrimal duct (NLD) obstruction with reflux through the superior punctum into the conjunctiva with patent left NLD system. Fig. 11.4 Obstruction of the left common canaliculus–sac junction with reflux of dye into the conjunctival region. Patency of the NLD system without reflux through the canalicular system normally indicates an anatomically patent system (left side, Fig. 11.3). Failure of the dye to penetrate the lacrimal sac may indicate a common canalicular obstruction (Fig. 11.4). To assess the function of the NLD system, lacrimal scintillography is performed. DCG assesses anatomy but not function. A radioisotope is placed in the conjunctival fornix and regular scanning performed for 30 minutes. If the isotope penetrates the lacrimal sac and not the nasal cavity, NLDO exists (Fig. 11.5). In some patients the DCG may show no filling of the lacrimal sac, whereas scintillography shows filling of the sac (Fig. 11.6). This may occur when the sac is full of mucus and the distended sac kinks the common canaliculus just before it enters the sac. Scintillography also helps identify a functional obstruction when the DCG is normal (patent) in a symptomatic patient. If the scintillography confirms lack of nasal cavity penetration of the isotope, then a functional NLDO exists (Fig. 11.7). These patients can be managed by performing an endoscopic DCR but the outcome is not as successful as with anatomical obstruction of the NLD system (see results of functional NLDO). After nasal decongestion with neuropatties and infiltration with lidocaine and adrenaline, a no. 15 scalpel blade is used to make the initial mucosal incisions. It is important that these incisions are correctly placed as they form the borders for the subsequent bone removal and lacrimal sac exposure. The first incision is made horizontally 8 to 10 mm above the axilla of the middle turbinate, starting ~3 mm posterior to the axilla and coming forward ~10 mm onto the frontal process of the maxilla (bony prominence in the lateral nasal wall just anterior to the middle turbinate). The blade is then turned vertically and a vertical incision made to about two-thirds of the vertical height of the middle turbinate, stopping just above the insertion of the inferior turbinate into the lateral nasal wall (Fig. 11.8). The blade is turned horizontally and the inferior incision is started at the insertion of the uncinate process and brought forward to meet the vertical incision (Fig. 11.9). Fig. 11.5 DCG shows nasolacrimal duct obstruction (NLDO) on the right side. The scintillography shows penetration of the radioisotope on the left into the nasal cavity but shows holdup on the right with no nasal cavity penetration. This confirms the diagnosis of NLDO. Fig. 11.6 Obstruction of left common canaliculus on DCG with radioisotope penetrating the lacrimal sac on scintillography indicating likely distention of sac kinking common canaliculus–sac junction. Fig. 11.7 If the left side is examined on the DCG the system appears normal. However, on the scintillography although the sac fills nicely with radioisotope, no penetration of the nasal cavity occurs. Later time points need to be checked to ensure that this continues to be the case. This is an anatomical obstruction of the nasolacrimal system on the right side and a functional obstruction on the left side. Fig. 11.8 (A) Mucosal incisions 8 to 10 mm above and anterior to the axilla of the middle turbinate. (B) Cadaveric dissection demonstrating the horizontal and vertical incisions. The horizontal superior incision is made 8 to 10 mm above the axilla of the middle turbinate (MT), and started 3 mm behind the axilla of the MT, and continued 10 mm in front. The vertical incision is continued for two-thirds of the MT height. (A adapted with permission from Wormald PJ. Powered endoscopic DCR. Otolaryngol Clin North Am 2006;39:539–549.) Using a 30-degree endoscope a suction Freer elevator is used to elevate the mucosal flap while ensuring that the tip of the instrument always maintains contact with the bone (Fig. 11.10). Be particularly careful to keep the tip of the suction Freer on bone as it rides over the prominence of the frontal process of the maxilla as the bone contour can fall away abruptly and contact with the bone and surgical plane can be lost. At this point the bone should be palpated so that the junction of the soft lacrimal bone and hard bone of the frontal process can be identified (Fig. 11.10C). This is a key landmark and must be sought in all primary surgeries. Note that the lacrimal bone is sought at the bottom of the region from which the mucosal flap has been raised, just above the insertion of the inferior turbinate. The thin lacrimal bone is 2 to 5 mm wide before the insertion of the uncinate process is reached (Fig. 11.11). Dissection stops at the uncinate and the uncinate insertion should not be disturbed. A round knife (from the standard ear tray of instruments) is used to flake the soft lacrimal bone away from the posteroinferior region of the sac. If this is difficult, the frontal process can be removed first before the lacrimal bone is flaked away. Fig. 11.9 Cadaveric image of left nasal cavity demonstrating the inferior horizontal incision. This incision begins from the insertion of the uncinate process (UP) forward to meet the vertical incision. Fig. 11.10 (A) Illustrates elevation of the flap with a suction Freer elevator. Note the round knife removing the thin lacrimal bone in the inferior region of the dissection. The cadaveric photo (B) shows the suction Freer hard against the frontal process (FP), elevating the mucoperiosteal flap. (C) At the junction where the hard frontal process can fall away to become the soft lacrimal bone (LB), care must be taken when elevating in this region. MT, middle turbinate. (A adapted with permission from Wormald PJ. Powered endoscopic DCR. Otolaryngol Clin North Am 2006;39: 539–549.)
Powered Endoscopic
Dacryocystorhinostomy
 Preoperative Assessment of the Patient Presenting with Epiphora
Preoperative Assessment of the Patient Presenting with Epiphora
Examine the Eye and Look for Other Causes of Watery Eye
Excess Tear Production
 Conjunctival disease. Patients with conjunctivitis present with sticky secretions or pus in the eye that is often worse when they awake in the morning. Antibiotic eye drops are used to treat bacterial infections and prevent colonization in patients with viral conjunctivitis.
Conjunctival disease. Patients with conjunctivitis present with sticky secretions or pus in the eye that is often worse when they awake in the morning. Antibiotic eye drops are used to treat bacterial infections and prevent colonization in patients with viral conjunctivitis.
 Lid malposition. Ectropion or entropion cause the puncta to not be properly positioned in the tear lake. A floppy lower eyelid (increased lid laxity) may also place the puncta in a position where tear collection is impaired. Surgical repositioning or tightening of the lid is required.
Lid malposition. Ectropion or entropion cause the puncta to not be properly positioned in the tear lake. A floppy lower eyelid (increased lid laxity) may also place the puncta in a position where tear collection is impaired. Surgical repositioning or tightening of the lid is required.
 Blepharitis. Blepharitis causes a mucoid discharge from the eye. In this condition there is an alteration in the bacteriology of the mucous glands in the hair follicles of the eyelashes that results in a mucoid discharge from the eye. The vision will be blurred and the eye often burns. Treatment is to rub the eyelid margin with gauze soaked in warm soapy water twice a day. This will need to be done for ~3 months before the condition resolves.
Blepharitis. Blepharitis causes a mucoid discharge from the eye. In this condition there is an alteration in the bacteriology of the mucous glands in the hair follicles of the eyelashes that results in a mucoid discharge from the eye. The vision will be blurred and the eye often burns. Treatment is to rub the eyelid margin with gauze soaked in warm soapy water twice a day. This will need to be done for ~3 months before the condition resolves.
Epiphora
 Punctal stenosis. Obliteration or narrowing of the superior or inferior punctum.
Punctal stenosis. Obliteration or narrowing of the superior or inferior punctum.
 Canalicular stenosis or obstruction. Superior or inferior canalicular stenosis or obstruction may follow trauma or viral infection.
Canalicular stenosis or obstruction. Superior or inferior canalicular stenosis or obstruction may follow trauma or viral infection.
 Nasolacrimal duct blockage. Usually from unknown cause.
Nasolacrimal duct blockage. Usually from unknown cause.
Nasolacrimal Duct Obstruction
Examine the Nasal Cavity
Dacryocystogram and Lacrimal Scintillography

 Surgical Technique14,17–19 (Videos 33 and 34)
Surgical Technique14,17–19 (Videos 33 and 34)
 Dry eye. Patients may have significant dryness that will irritate the eye and produce tearing. Application of artificial tears is usually all that is necessary.
Dry eye. Patients may have significant dryness that will irritate the eye and produce tearing. Application of artificial tears is usually all that is necessary.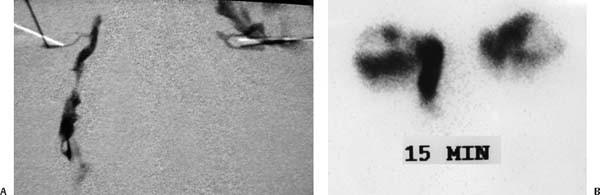
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


