CHAPTER 45 Epistaxis
Epistaxis is the commonest otolaryngologic emergency, affecting up to 60% of the population in their lifetimes, with 6% of cases requiring medical attention.1 It has been estimated that nosebleeds affect 108 per 100,000 population per year.2 In England and Wales an average of 10.2 per 100,000 patients with nosebleed are admitted, for an average stay of 2.9 days, in a 3-month period3; and in the United States 17 per 100,000 or 6% of patients with nosebleed are admitted.4 There are peaks in incidence for patients both younger than 10 years old and older than 40 years.4–6 The etiology of epistaxis in the majority of patients is idiopathic,7 followed in frequency by primary neoplasms and traumatic or iatrogenic causes.
Decisions about the optimum therapeutic intervention and timing are often made on an ad hoc basis, and most units do not have a protocol (systematic algorithm) for the management of epistaxis,8 despite a 2005 published protocol aimed at junior doctors.9 However, this protocol does not contain the timing of surgical intervention. The management of a patient with epistaxis ranges from resuscitation, through direct visualization and cautery, nasal packing, and surgery (both endoscopic and external) to embolization.
Vascular Anatomy
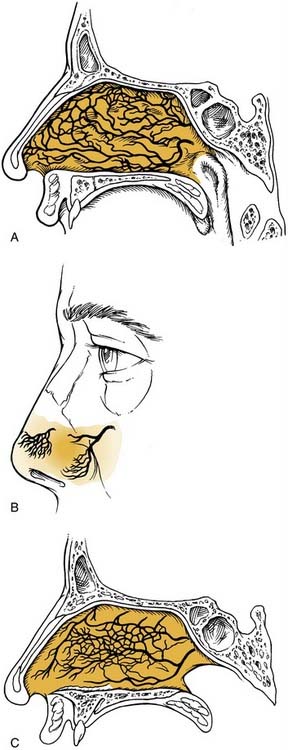
The nasal cavity is extremely vascular. Terminal branches of the external and internal carotid arteries supply the mucosa of the nasal cavity with frequent anastomoses between these systems (Fig. 45-1). The anterior nasal septum is the site of a plexus of vessels called Little’s or Kiesselbach’s area, which is supplied by both systems.

The terminal branches of the external carotid artery that supply the nasal cavity are the facial artery and the internal maxillary artery. The facial artery supplies the superior labial artery, which enters the nose and supplies the anterior nasal septum. The internal maxillary artery courses within the pterygopalatine fossa and terminates in the sphenopalatine, descending palatine, pharyngeal, infraorbital, and posterior superior alveolar arteries. The branching of the sphenopalatine artery when it enters the nasal cavity is a key point in the understanding of the management of posterior nosebleeds. The sphenopalatine artery enters the nasal cavity through the sphenopalatine foramen and then divides into conchal (posterior-lateral) and septal (posterior-medial) branches.10,11 The descending palatine artery courses through the greater palatine canal and becomes the greater palatine artery, entering the nose through the incisive foramen, where it supplies the anterior inferior septum and anastomoses with medial branches of the sphenopalatine artery. Importantly, the vidian artery has a significant anastomosis between the internal carotid artery and a branch of the sphenopalatine artery and therefore with the external carotid system (Fig. 45-2).

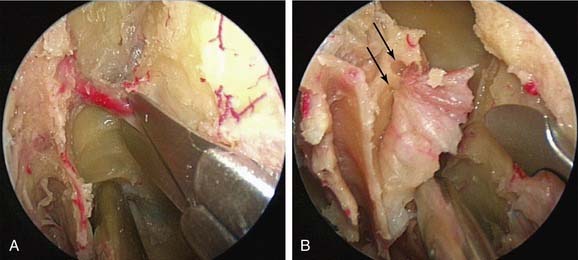
The internal carotid artery supplies the nasal mucosa via the ethmoidal branches of the ophthalmic artery. The ophthalmic artery is the first branch of the internal carotid artery. The posterior ethmoidal artery passes through the posterior ethmoidal canal into the anterior cranial fossa and divides into lateral and medial branches, supplying the superior part of the posterior septum and lateral nasal wall. The anterior ethmoidal artery enters the nasal cavity through the anterior ethmoidal canal and passes anteromedially to the area of the anterior skull base (Fig. 45-3). Where it crosses the anterior ethmoid roof to reach the fovea ethmoidalis and cribriform plate, a nasal branch supplies the anterior superior part of the septum (Fig. 45-4) and its other branch—the anterior meningeal artery—enters intracranially.
A fundamental aspect of the understanding of the vascular anatomy and its importance to epistaxis is the fact that various anastomoses on the ipsilateral side between the internal and external carotid systems exist as well as crossover to the contralateral side. The rich anastomoses underlie the importance of a strategy to address the most distal site of any bleeding (Figure 45-5).
Management
Initial Assessment
Obtaining intravenous access, checking for and correcting any clotting abnormalities, and taking blood for “group and save” and/or crossmatching may be required. In our unit patients admitted via the emergency department can be “fast-tracked” to the otorhinolaryngologic emergency unit if stable (Box 45-1). This practice helps avoid unnecessary and counterproductive nasal packing in the emergency department as well as transfer of patients before they are fit enough to travel.
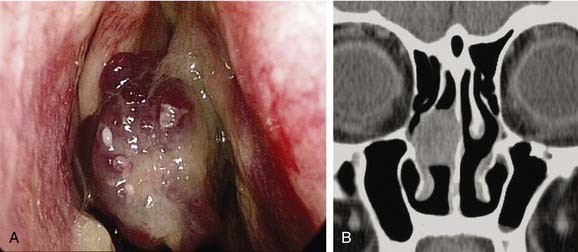
It is important to establish both the site and the cause (Box 45-2; Figs. 45-6 to 45-12) of bleeding. The philosophy of this approach can be summarized as follows:
Box 45-2 Etiology—Selected Causes of Epistaxis


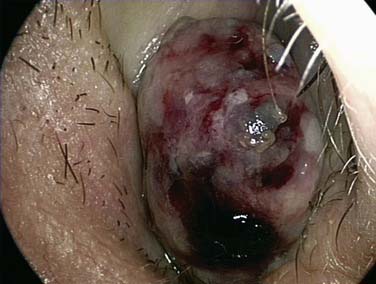




Figure 45-12. Total septal perforation causing epistaxis and crusting in a patient with cocaine abuse.
The clinician must remember that epistaxis is frequently idiopathic but can be a manifestation of a possible underlying pathology (see Fig. 45-12). Your patient should undergo further investigation according to the history.
Epistaxis in Children
Young children usually bleed from a vessel just inside the nose at the mucocutaneous junction on the septum, and the bleeding invariably stops spontaneously. In children with epistaxis in whom no prominent vessel can be seen, the regular local application of a cream can help,12 but petroleum jelly (Vaseline) alone does not.13 A Cochrane Collaboration systematic analysis of the efficacy of topical treatments for idiopathic epistaxis in children concluded that the best treatment still must be defined.14 As many as 5% to 10% of children with recurrent nosebleeds may have undiagnosed von Willebrand’s disease.15,16 Children who have leukemia or are undergoing chemotherapy often have epistaxis associated with thrombocytopenia. Older children, adolescents, and adults often bleed from Little’s area or a maxillary spur.
Epistaxis in Adults
The caudal end of the septum, where several branches of the external and internal carotid anastomose in Little’s area or Kiesselbach’s plexus, is the most common site of bleeding in adults.17 Less commonly bleeding, comes from further back on the septum, and a septal deviation may make it difficult to visualize (Fig. 45-13). Some patients with seasonal allergic rhinitis complain of more nosebleeds in the hay fever season, and topical nasal steroids aggravate the bleeding in approximately 4% of users. Many people believe that a nosebleed signifies a release of pressure and may herald a stroke, and it is important for the clinician to address these anxieties for the patient. Although many patients are found to be hypertensive during nosebleeds, few remain so on follow-up. The association between hypertension and epistaxis is disputed.18 Many clinicians report that hypertension is not related to nosebleed.19–21 However, nosebleeds in patients with hypertension are more likely to lead to admission and to be associated with comorbidity.22

Bleeding disorders can manifest de novo as nosebleeds, although this situation is rare. A range of drugs has been linked with epistaxis, warfarin being one of the most common.3,23 Nearly a third of patients admitted with epistaxis who were taking warfarin had an international normalized ratio (INR) value above the upper limit of the therapeutic range.24 The need to reverse anticoagulation is uncertain as long as the INR value is within the therapeutic range.25 In over-anticoagulated patients, fresh frozen plasma, clotting factor extracts, and vitamin K help. Vitamin K takes more than 6 hours to work, however, and it can delay anticoagulation for 7 days after warfarin is started. If the INR value is greater than 4, the warfarin should be stopped, and fresh frozen plasma given.23 Clotting factor extracts should be given with extreme caution because of the risk of thromboembolic complications. Tranexamic acid, an antifibrinolytic agent, has not been shown to help.26 Other drugs associated with bleeding are aspirin, which interferes with platelet function for up to 7 days, clopidogrel, and nonsteroidal anti-inflammatory drugs.27,28 In patients who do not have a history of a bleeding disorder or undergoing anticoagulant therapy, routine clotting studies do not add to the management.22,24 There is a higher incidence of epistaxis in patients with a high alcohol intake, even when there is no laboratory evidence of a coagulation abnormality.29,30
Topical Treatment
A randomized controlled trial of silver nitrate cautery with topical antiseptic nasal carrier cream versus topical alone showed both to be effective.31 A study of patients applying weekly triamcinolone 0.025% and daily petroleum jelly reported that 89% of patients had no further bleeding.32 Various hemostatic compounds have been used but without consistent evidence of their efficacy. Collagen-derived particles with bovine-derived thrombin have been found to be better than nasal packs.33
Cautery
Most anterior epistaxis can be controlled with identification of the bleeding point and cautery using a headlamp. The vast majority of posterior bleeding sites can be identified by endoscopy without the use of general anesthesia.34 The majority of posterior idiopathic bleeds are from the septum, usually from the septal branch of the sphenopalatine artery as it runs submucosally (Fig. 45-14
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


