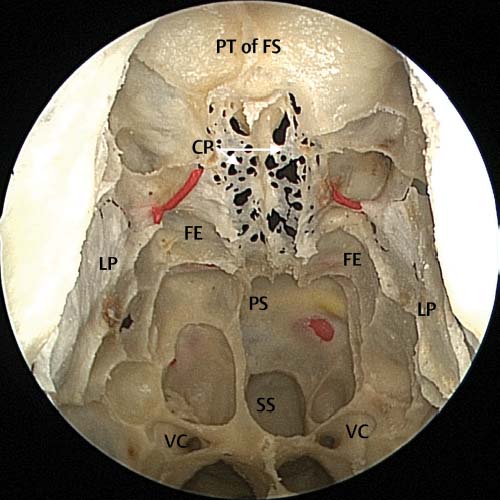
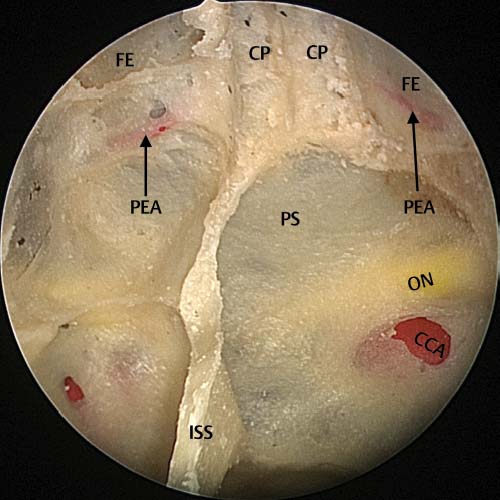
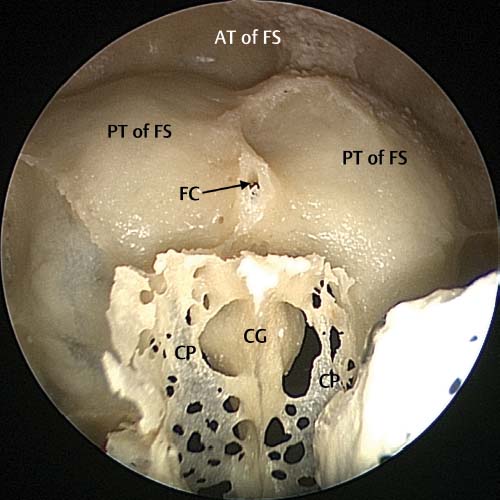
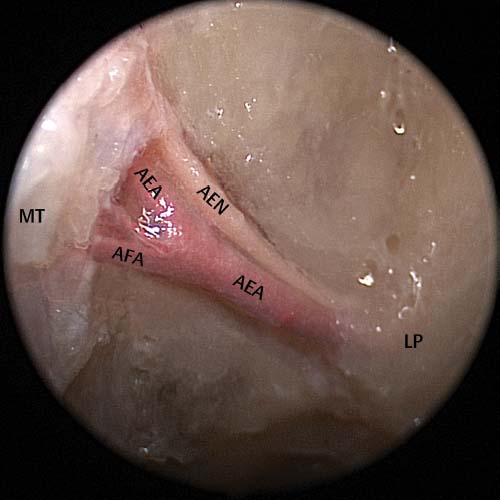
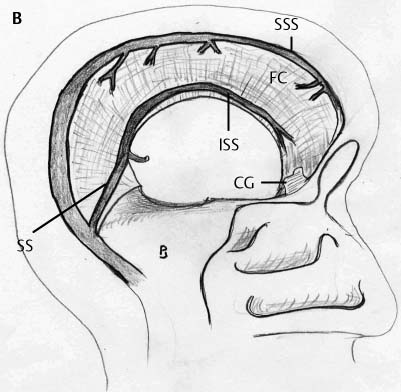
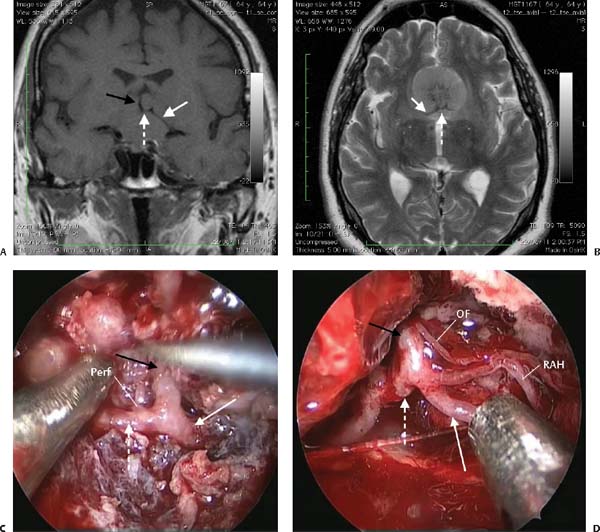
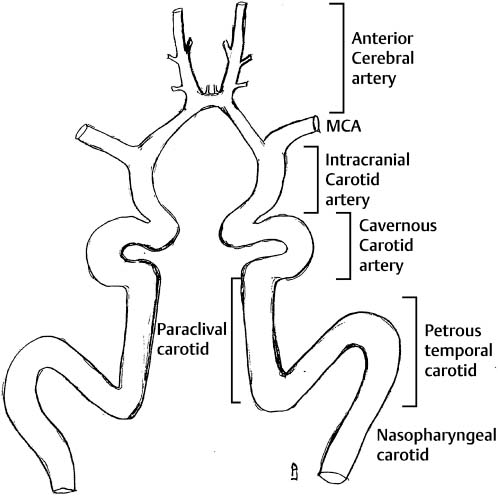
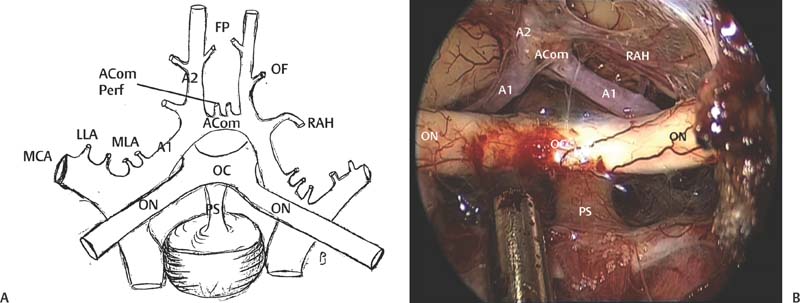
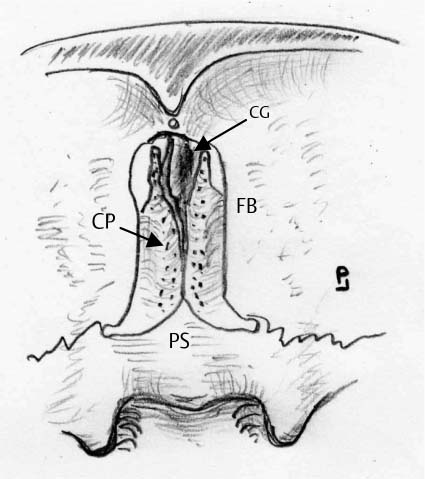
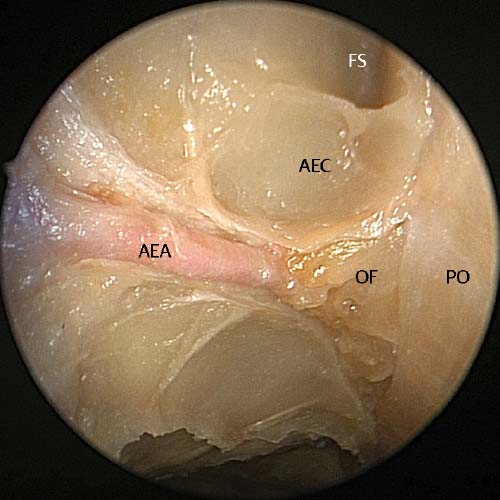
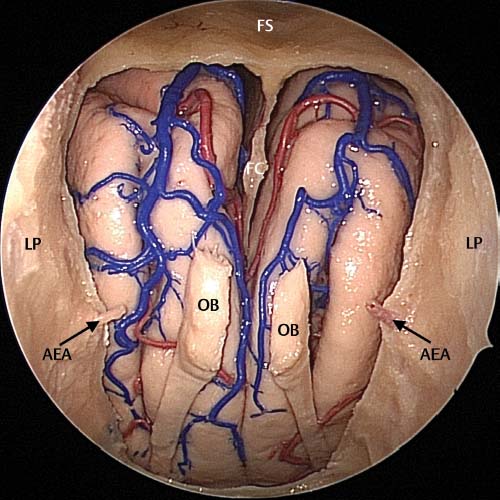
20 Endoscopic techniques for transnasal resection of anterior cranial fossa tumors were developed for tumors involving the nasal cavity, sinuses, and the anterior cranial fossa. However, experience with these tumors has led to the refinement of these techniques to address tumors of the anterior cranial fossa that do not have a nasal or sinus component. Although most of this experience has been with meningiomas, these techniques can also be used to address malignant nasal tumors that are primary intracranial or that extend intracranially. The first step toward a wholly endoscopic resection of malignant sinonasal tumors was the experience gained with endoscopic management of the sinonasal component of the tumor during a standard craniofacial resection. We found that the endoscopic resection of the sinonasal component could be as effectively dealt with endoscopically as it can with external traditional approaches. In the case of large tumors involving both nasal cavities, the endoscopic approach was more effective as it dealt with both sides as opposed to most of the external approaches which limited access to one side of the nose. A significant number of these malignant tumors attach to the skull base and associated orbit. During craniofacial resection the skull base involved with tumor is completely excised.1–3 The associated orbital involvement would, in most circumstances, be removed as a separate excision. We found that endoscopically resecting the sinonasal component afforded better visualization of the tumor allowing the nonattached tumor to be extensively debulked and the regions of tumor attachment to be accurately identified. This in turn allowed a complete resection of the sinonasal and, if present, the orbital component. As the experience with anterior skull base tumor resections developed, these techniques could in turn be applied to the resection of malignant tumors involving the skull base and intracranial cavity. Tumors thought to be suitable were tumors with a localized intracranial extension. Because of the infiltrative nature of squamous cell carcinomas these were thought not to be as suitable as adenocarcinoma and esthesioneuroblastoma, which in general have a pushing rather than infiltrative front and are thus more easily addressed endoscopically. Although the gold standard for resection of these malignancies was a craniofacial resection,1 there is increasing evidence that for selected patients the wholly endoscopic resection yields comparable results.2–6 Recently published series have reported similar morbidity and mortality rates and very similar local recurrence rates.2,3,5,6 In addition, there are significant benefits for the patients undergoing wholly endoscopic resection because uninvolved structures are not removed and this approach avoids skin incisions with improved cosmetic results.2–6 In addition, those patients who are medically or otherwise unsuitable for a standard craniofacial resection, or who choose not to undergo this procedure, can be offered the endoscopic approach as an alternative. Endoscopic resection of the anterior skull base requires a detailed knowledge of the anatomy of this region. The anterior skull base consists of the orbital plates of the frontal bone with the cribriform plates (part of the ethmoid bone) separating them. These plates attach to the planum sphenoidale (lesser wing of the sphenoid bone) posteriorly (Fig. 20.1). The cribriform plate gives rise to the crista galli onto which the falx cerebri attaches anteriorly. If the anterior skull base is approached endoscopically from front to back the frontal bone (posterior wall of the frontal sinus), foveae ethmoidalis, and intervening cribriform plates can be seen (Figs. 20.2 and 20.3). Posteriorly the foveae ethmoidalis and cribriform plates attach to the planum sphenoidale (Fig. 20.4). The important vascular structures within the anterior skull base are the anterior and posterior ethmoid arteries. Note how there is a space or cell between the frontal sinus ostium and the anterior ethmoidal artery (Fig. 20.5). This is always the case as the artery usually runs in the base of the second lamella which is the upward continuation of the anterior face of the bulla ethmoidalis. Fig. 20.1 This diagram illustrates the view of the anterior skull base from above (intracranial side). The crista galli (CG), cribriform plate (CP), orbital plate of the frontal bone (FB), and planum sphenoidale (PS) of the lesser wing of the sphenoid bone are visible. Fig. 20.2 Cadaveric dissection illustrating the anatomy of the anterior skull base following partial resection of both middle turbinates (MT) and nasal septum. The communal frontal sinus (FS) ostium can be seen anteriorly with both fovea ethmoidalis (FE) exposed. The lateral margins are the lamina papyracea (LP) and posteriorly the planum sphenoidale (PS) can be seen. OF, olfactory fossa; AEA, anterior ethmoidal artery; PEA, posterior ethmoidal artery; AEN, anterior ethmoidal nerve; PEN, posterior ethmoidal nerve. Fig. 20.3 Dry bone specimen following a Draf 3 shows the delicate cribriform plate (CP) and fovea ethmoidalis (FE). The nasal septum and middle turbinates have been completely resected. The sphenoid sinus (SS) can be seen posteriorly with the roof forming the planum sphenoidale (PS). The lamina papyracea (LP) is still intact. VC, vidian canal; PT of FS, posterior table of frontal sinus. Fig. 20.4 Dry bone dissection image taken with a 30-degree endoscope demonstrating the fovea ethmoidalis (FE) and cribriform plate (CP) junction with the planum sphenoidale (PS). This is marked approximately by the posterior ethmoidale artery (PEA). ISS, intersinus septum of sphenoid sinus; ON, optic nerve; CCA, anterior genu of the intracavernous carotid artery. Fig. 20.5 Cadaveric dissection image of the left ethmoid cavity revealing the anterior ethmoidal artery (AEA) located one anterior ethmoidal cell (AEC) posterior to the frontal sinus (FS). OF, orbital fat; PO, periorbita. Fig. 20.6 Dry bone specimen following a frontal drillout procedure. This specimen clearly shows the close relationship between the frontal sinuses and the cribriform plate, and hence the advantage of the drillout procedure for anteriorly based lesions. AT of FS, anterior table of frontal sinus; PT of FS, posterior table of frontal sinus; FC, foramen cecum; CP, cribriform plate; CG, crista galli. One of the first decisions that need to be made is whether the entire skull base needs to be resected. To determine this, the important landmark is the anterior ethmoidal artery (AEa). If the tumor approaches but does not come further forward than the anterior ethmoidal artery then the posterior skull base can be resected without the need to perform a modified Lothrop or frontal drillout procedure. Once the tumor encroaches past the AEa, a frontal drillout is necessary to be able to achieve the correct angle onto the tumor and be able to delineate the anterior arachnoid/tumor interface. This is necessary so that, once the inside of the tumor has been debulked, the tumor arachnoid plane can be identified and the tumor wall collapsed into the tumor cavity allowing progressive resection of the tumor. Resection of the skull base is only possible once the entire skull base has been exposed. This requires, as a first step, bilateral sphenoethmoidectomy with exposure of the skull base within the sphenoids, anterior and posterior ethmoids, and visualization of the frontal ostia. If the entire anterior skull base is to be resected the frontal sinuses need to be drilled out with an endoscopic modified Lothrop procedure. The relationship between the cribriform plate and the frontal sinuses is clearly illustrated in this osteology model and illustrates the importance of performing a frontal drillout procedure for more anteriorly based tumors (Fig. 20.6). The other important structures that need to be identified are the anterior ethmoidal artery and the posterior ethmoidal artery. Note how the anterior ethmoidal artery has the anterior ethmoidal nerve running adjacent to it and how the lamina papyracea tents into the skull base as the anterior ethmoidal canal is formed (Figs. 20.5 and 20.7). This tenting of the lamina papyracea is important to understand when exposing and cauterizing the AEa. Our preferred technique is to expose the artery with a diamond burr then to use the suction bipolar to cauterize the artery. However, if the burr is too big or if the exposure is done over the lateral area on the triangular fat invagination, division of the artery with the burr may result in retraction of the artery into the orbit and orbital hematoma formation. This has happened in one case in which an anterior skull base tumor was being removed and required an immediate orbital decompression to relieve the pressure in the eye. The tumor resection continued uneventfully once this had been done. The posterior ethmoidal artery should be addressed in the same manner with exposure with a diamond burr and bipolar cautery. Once this has been done any residual septum is detached from the anterior skull base. Fig. 20.7 Cadaveric dissection image demonstrating the left anterior ethmoidal artery (AEA) and nerve (AEN) running across the skull base toward the middle turbinate (MT) attachment. Here it can be seen dividing into several branches including the anterior falcine artery (AFA) to supply the falx cerebri. LP, lamina papyracea. Fig. 20.8 Cadaveric dissection image: the skull base has been removed affording a view of the inferior aspect of both anterior cerebral lobes. The olfactory bulbs (OB), branches of the anterior cerebral artery (ACa), and cut inferior aspect of the falx cerebri (FC) can be seen. FS, frontal sinus; AEA, anterior ethmoidal artery; LP, lamina papyracea. Fig. 20.9 The anterior attachment of the falx cerebri (FC) to crista galli (CG) is seen. Note the superior sagittal sinus (SSS) running in the superior aspect of the falx cerebri within the inferior sagittal sinus (ISS) in the lower margin of the falx cerebri. The inferior sagittal sinus becomes the straight sinus (SS) after it joins with the great cerebral vein. Once the skull base has been dropped down and removed, the anterior cranial fossa can be viewed (Fig. 20.8). The two olfactory bulbs and olfactory tracts are seen on the under-surface of the anterior cerebral hemispheres. The major vascular structures are the anterior cerebral arteries and branches from these arteries. The venous drainage of the anterior cranial fossa is via the superior and inferior sagittal sinuses. The superior sagittal sinus runs in the upper border of the falx cerebri whereas the inferior sagittal sinus runs in the lower border of the falx cerebri (Fig. 20.9). Large anterior skull base tumors may have large veins draining into the inferior sagittal sinus which if disrupted can bleed significantly. Tumors that arise in the tuberculum sella region, planum sphenoidale, or posterior olfactory fossa can involve the anterior part of the circle of Willis and anterior cranial fossa vessels as they push posteriorly and superiorly (Fig. 20.10). Figure 20.11 gives an overview of the how the carotids enter the skull base and then form the anterior portion of the circle of Willis and go on to supply the anterior cranial fossa. The most common tumor in this region is the tuberculum sella meningioma but others include craniopharyngiomas and anterior/superior extension of pituitary tumors. When the tumor fills the subchiasmatic cistern, the superior hypophyseal vessels are also at risk and damage to these vessels can lead to ischemic damage of the optic nerves and chiasm with blindness. When the A1–AComm-A2 complex is surrounded by tumor understanding the anatomy of this complex is vital for safe surgery to be performed in this region (Fig. 20.10). A detailed description of the anterior cerebral arteries is given in Fig. 20.12. A1 (first part of the anterior cerebral artery) is formed when the internal carotid divides into the middle and anterior cerebral arteries. It enters the lamina terminalis cistern and at this point is banded to the lateral aspect of the optic nerves by thick arachnoid bands.7 The medial lenticulostriate arteries arise from the posterior and superior surface of the first half of A1 and supply the medial septum pellucidum, medial part of the anterior commissure and pallidum, pillars of the fornix, paraolfactory area, anterior limb of the internal capsule, anteroinferior part of the striatum, and anterior hypothalamus. Vessels arising from the second half of A1 are smaller and join the arterial plexus of the optic nerve, chiasm, and optic tract.7 Once identified the A1 vessel wall can be followed to the anterior communicating artery (AComm) and the recurrent artery of Heubner8 (Figs. 20.10 and 20.12). The recurrent artery of Heubner (RAH) is present bilaterally in 85% of patients, unilaterally in 11%, and absent in 4%. It immediately courses posteriorly toward the trunk of A1 before entering the subarachnoid space and penetrating the brain at the junction of the medial and lateral olfactory stria. It is an important vessel to preserve because it supplies the head of the caudate and the anteroinferior internal capsule, anterior hypothalamus, and olfactory region. The other vitally important vessels in this region are the posterior perforating vessels from the AComm. These branches can number from one to six and arise from the superior and posterior surface of AComm and course posteriorly to supply the infundibulum of the pituitary, optic nerve and chiasm, lamina terminalis, anterior perforating substance, corpus callosum, anterior commissure, limbic system, and associated regions of cortex. Deficits associated with injury to these arteries include serious and incapacitating memory deficits, personality changes, and electrolyte imbalances. Occlusion of A1 region can result in paraplegia of the lower extremities with sparing of the upper limbs, incontinence, abulic or motor aphasia, and frontal lobe symptoms. Fig. 20.10 (A,B) MRI scans show the A1 (solid white arrow) leaving the middle cerebral artery juncture toward the AComm (dashed white arrow) with the A2s (black arrow) progressing superiorly. These vessels are all within the substance of the tumor. The clinical dissection of this tumor is seen in (C) and (D) with tumor encompassing the perforators (Perf) coming off the AComm. Once all tumor had been removed the vascular complex with A1-AComm,-A2 and the important branch of A1, the recurrent artery of Heubner (RAH), and the A2 branch, orbitofrontal (OF) artery, are clearly visible. The A2 (anterior vertebral artery after AComm) has three main branches (Figs. 20.10 and 20.12). The RAH originates from the AComm-A2 junction or from the first few millimeters of A2 in 90% of patients (in the other 10% from the upper A1).7 The other two branches are the orbitofrontal and frontopolar branches. The orbitofrontal usually originates from the first 5 mm of A2 at the junction of the lamina terminalis and callosal cisterns and has a downward and forward course crossing the olfactory tract to the gyrus rectus. The frontopolar branch originates after the orbitofrontal branch and travels anteriorly more medially across the subfrontal sulcus. Fig. 20.11 The carotid bends laterally in the nasopharynx before entering the petrous temporal bone. It then swings anteriorly before becoming the paraclival carotid in the floor of the sphenoid and progresses vertically into the cavernous sinus and then enters the anterior cranial fossa giving off the middle cerebral artery (MCA) to become the anterior cerebral artery. The surgical removal of anterior skull base tumors requires a team consisting of an endoscopic sinus surgeon and a neurosurgeon. It is vitally important that both members of this skull base team have endoscopic skills. These are best learnt doing pituitary tumor resections as a team. Here the neurosurgeon learns how to manage the endoscope and how to work from the video monitor in two dimensions rather than with the microscope in three dimensions. The sinus surgeon learns how to manipulate intracranial tumors and surrounding neural and vascular structures. These hours spent on pituitary tumor resection build confidence within the skull base team enabling benign or malignant nasal tumors with intracranial extension to be tackled. The first steps for access are complete sphenoethmoidectomy with exposure of the entire skull base. If the tumor is relatively posteriorly sited with a relatively small intracranial extension, skull base resection can be performed without a modified Lothrop procedure. In such cases the intracranial extension of tumor must be small and the resection of this extension should be possible without it being necessary to resect across the midline. Surgically, the skull base defect should be clearly delineated and then enlarged to expose uninvolved dura on all sides of the defect. The dura is then excised with a combination of endoscopic skull base scissors* (Medtronic ENT, Jacksonville, FL) or scalpel with a normal margin of dura and the tumor extension and dura delivered into the nose. However, if a complete resection of the anterior skull base is required then the next step is to perform an endoscopic modified Lothrop procedure allowing the anterior aspect of the skull base to be delineated (Fig. 20.13). The nasal septum is separated from the skull base allowing visualization of the entire skull base from the frontal sinuses anteriorly to the anterior face of the pituitary fossa (Fig. 20.2). Both laminae papyracea should be on view forming the lateral limits of the resection. Before the skull base can be resected the anterior and posterior ethmoidal arteries need to be identified and ligated or cauterized and divided. The technique of removing lamina papyracea to find the anterior artery as it enters the canal is not preferred as it risks rupture of the artery and with fat prolapse makes identification of the artery very difficult. An easier and safer technique is to run the diamond burr over the region of the anterior ethmoidal artery removing the bone until the artery is exposed in its canal. The bone is removed and the artery identified and exposed. It is then cauterized, and divided. This is done bilaterally before the posterior ethmoidal arteries are also identified using the diamond drill on the skull base. The arteries usually enter the skull base at the junction of the posterior ethmoids and sphenoid and the drill is run over this region of the skull base until the artery is clearly identified, cauterized, and cut on both sides (Fig. 20.4). Fig. 20.12 (A) The middle cerebral artery (MCA) gives rise to the lateral lenticulostriate arteries (LLA) at the bifurcation complex. The medial lenticulostriate arteries (MLA) arise from the proximal section of A1. At the juncture of A1-AComm-A2 the recurrent artery of Heubner (RAH) is given off. AComm completes the anterior portion of the circle of Willis and has several perforating vessels (AComm Perf) that head posteriorly. In the first 5 mm of A2 the orbitofrontal (OF) artery is given off with the frontopolar (FP) artery staying more medial. (B) A clinical picture after removal of a tuberculum sella meningioma with a well-defined display of the anterior cerebral arteries.
Endoscopic Resection of Anterior
Cranial Fossa Tumors
 Anatomy of the Anterior Skull Base
Anatomy of the Anterior Skull Base

Vascular Anatomy of the Anterior Cranial Fossa (Video 56)
 Surgical Technique (Videos 54 to 56)
Surgical Technique (Videos 54 to 56)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


