 he term anterior blepharitis refers to inflammation of the eyelashes and follicles. Posterior blepharitis refers to meibomian gland dysfunction. Blepharitis often is associated with systemic diseases such as rosacea, as well as ocular diseases such as the dry eye syndrome, conjunctivitis, and keratitis. Many patients have a history of a drug reaction or fever associated with their blepharitis.
he term anterior blepharitis refers to inflammation of the eyelashes and follicles. Posterior blepharitis refers to meibomian gland dysfunction. Blepharitis often is associated with systemic diseases such as rosacea, as well as ocular diseases such as the dry eye syndrome, conjunctivitis, and keratitis. Many patients have a history of a drug reaction or fever associated with their blepharitis.
Patients with posterior blepharitis have ocular symptoms of burning, watering, foreign-body sensation, photophobia, and decreased vision.
On examination, you may find crusting of the lashes and meibomian orifices and plugging and “pouting” of the meibomian orifices. Corneal findings can include punctuate epithelial erosions and corneal ulcers or pannus.
Posterior blepharitis is related to dysfunction of the meibomian glands; the meibomian secretions become waxlike and block the gland orifices. Visual inspection reveals the typical plugging and “pouting” of the meibomian orifices, leading to diagnosis. Test for tear insufficiency aids in diagnosis, leading to improved dry eye treatment.
Early in these conditions, we recommend the following treatment:
- Hot packs to the lids. The goal is to get the secretions in the meibomian glands to melt, liquefy, and drain out to the lid margin.
- A balanced diet rich in fruits and vitamins.
- A teaspoonful of flaxseed oil every day. We have found that flaxseed oil ameliorates many symptoms. A drop in the eye also helps.
If the condition is advanced and medical treatment is not working, surgery is recommended. Surgery in these cases consists of opening each individual meibomian duct. This procedure can be accomplished with the Fugo blade, which opens the ducts without charring or burning tissue. Before the advent of the Fugo blade, there was no device that could perform this function.
Both lids of one eye are treated at the first sitting, so that the patient can compare the relief obtained from the operation with the condition of the untreated eye. The worst eye is treated first.
TECHNIQUE
Anesthesia
Use topical anesthetic and lidocaine along the lid margin.
Surgical Technique
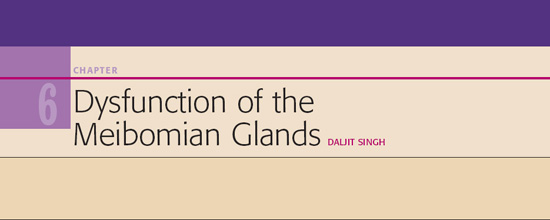
- Use either the standard capsulotomy Fugo plasma blade tip or a special sharp pointed long tip (300 µm) (Fig. 6.1). The idea is to clear the meibomian ducts and not damage the glands. Apply the lowest energy settings for ablation.
- Control the position of the lid margin with the thumb, such that the openings of the meibomian ducts are available for vertical penetration.
- Align the tip vertically, activate it, and insert it into the meibomian duct. When a duct is treated, a fatty substance flows out. When the tip is withdrawn a small gaping hole is left where earlier the fatty plug was (Figs. 6.2 and 6.3). We often see secretions coming out of the adjoining meibomian openings, which may indicate the presence of communicating channels between adjacent glands.
- Treat each meibomian gland in 1 to 2 seconds, so that all the glands are treated within a short time.
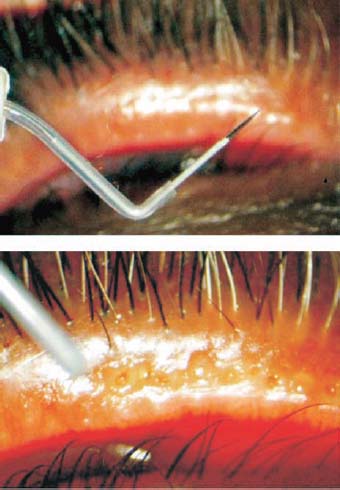
Figure 6.1. A long, sharp, pointed Fugo blade tip outside and inside the meibomian gland.
Postoperative Management
Advise patients that during the postoperative period they should continue with hot packs at least twice a day, maintain a nourishing diet, and take a spoonful of flaxseed oil daily.
Prescribe artificial tears as needed for burning or tearing and oil-based lubricant/antibiotics once or twice a day.
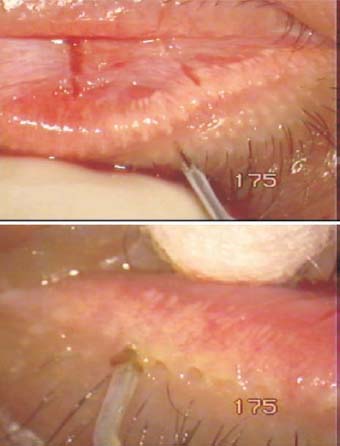
Figure 6.2. Heavily plugged meibomian gland openings before and during treatment.

Figure 6.3. Secretion-plugged meibomian glands before and 4 hours after Fugo blade treatment.

Figure 6.4. Finely plugged meibomian gland openings before and after treatment with the Fugo blade. Note the absence of burning or charring.
Patients commonly feel relief within 3 to 4 hours of meibomian gland treatment. No burning or charring of tissue occurs (Fig. 6.4). In most patients, the need for local artificial tears is greatly reduced and or even eliminated. Our patients are advised toreturn every 2 months, as some of them require retreatment.
Summary
During the past 5 years we have treated more than 20 patients with this method. Every patient benefitted to some extent from the treatment. The operation reduced their dependence on artificial tears. We advise patients to avoid being in the sun, especially in the summer, and to reduce evaporation of tears by closing their eyes for a few minutes every now and then.
If the meibomian glands are atrophied, this treatment does not help to improve secretion of the glands. However, the irritation and gritty feeling from the plugs at the lid margins is eliminated.
Patients with Stevens–Johnson syndrome may exhibit symptoms of meibomian gland dysfunction, not only plugged meibomian glands but also metaplasia, so that cilia grow from the meibomian ducts. These conditions can be treated with the Fugo blade.
Many people live with the terrible reality of dry eyes and are totally dependent on the frequent use of artificial tears. Some of these patients’ conditions are suitable for treatment of meibomian glands using the Fugo blade. For these patients, it is wise to proceed cautiously by treating only a few glands at a time and observing the response.
Suggested Reading
Cohen EJ. Cornea and external disease in the new millennium. Arch Ophthalmol. 2000;118:979–981.
Lowery RS. Adult blepharitis. Accessed January 3, 2010, at www.emedicine.com/oph/topic81.htm.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


