PHYSICAL EXAMINATION
Careful evaluation of visual function, including both acuity and visual field examination, should be performed to detect any loss of visual acuity or reduction of visual fields. This is usually verified with a formal ophthalmologic evaluation. Extraocular movements should be evaluated to rule out any dysfunction of the third (oculomotor), fourth (trochlear), and sixth (abducens) nerves. Olfaction should always be tested to rule out the possibility of an anterior skull base lesion, such as a meningioma of the cribriform plate or planum sphenoidale, extending posteriorly.
INDICATIONS
Tumors such as pituitary tumors, craniopharyngiomas, midline meningiomas, or a Rathke cleft cyst causing symptoms from mass effect (vision loss, pituitary or hypothalamic dysfunction) all require surgical decompression and/or resection. Even vascular lesions such as aneurysms can cause compression of the optic apparatus or other associated structures. In addition, certain suprasellar lesions involving the infundibulum or hypothalamus may require biopsy. All of these can be accomplished through a frontotemporal or subfrontal craniotomy, with wide exposure and access.
CONTRAINDICATIONS
There are few, if any, absolute contraindications to craniotomy for suprasellar tumors, assuming the patient is medically sound for surgery. Significant tumor burden in the sella may be challenging to remove completely through a craniotomy, but suprasellar tumors can always be accessed albeit with varying degrees of difficulty depending upon the relationship to the optic nerves and chiasm.
PREOPERATIVE PLANNING
Any surgical procedure should be well planned, particularly the anticipated trajectory to remove the lesion. It is important to obtain as much information as possible regarding endocrine status, visual status, and preoperative imaging prior to planning a surgical procedure in this region, which is replete with cranial nerves, proximal major arteries with perforating vessels, and the hypothalamic–pituitary axis. In addition, a rare compressive mass lesion such as a giant aneurysm must be ruled out because the surgical planning would demand preparation for management of this lesion. If a large aneurysm is anticipated, preoperative angiographic studies such as a digital subtraction or computed tomography (CT) angiogram should be performed. The surgical procedure may require more proximal control of the artery in the neck.
Magnetic resonance imaging is the best study to define the nature of the suprasellar mass; a fine-cut T1-weighted study should be obtained with and without contrast enhancement. Careful attention should be paid to involvement of the sella in addition to the suprasellar area, which may indicate a primary pituitary lesion, such as a pituitary adenoma or a cyst. Similarly, the relationship of the lesion to the third ventricle should be carefully examined. Coronal imaging allows evaluation of the optic nerves extending posteriorly from the posterior orbit through the optic canal and the suprasellar cistern and of the relationship of the lesion to the optic chiasm and tracts. Extraaxial lesions causing compression of the optic nerves should be visible in relationship to the nerves; an intrinsic lesion of the chiasm or hypothalamus may envelop and involve the optic nerves. Any involvement and encasement of major vessels (i.e., the internal carotid arteries, the proximal middle cerebral arteries, and the anterior cerebral arteries) should be delineated. The location and displacement of the pituitary stalk should be noted.
Occasionally, a CT scan may add complimentary information, especially to identify acute hemorrhage (such as pituitary apoplexy) or calcium within the tumor. This latter finding may be extremely helpful in identifying a craniopharyngioma, especially in patients in the pediatric age group.
There are several options for approaching lesions in the suprasellar region. The majority of the tumors in my practice are removed using a frontotemporal or subfrontal craniotomy (Fig. 9.1). The subfrontal approach may be unilateral or bilateral. The location of the tumor, its area of attachment, direction of displacement of the pituitary stalk, and its relationship to the optic nerves and canals are noted and included in the decision-making process.
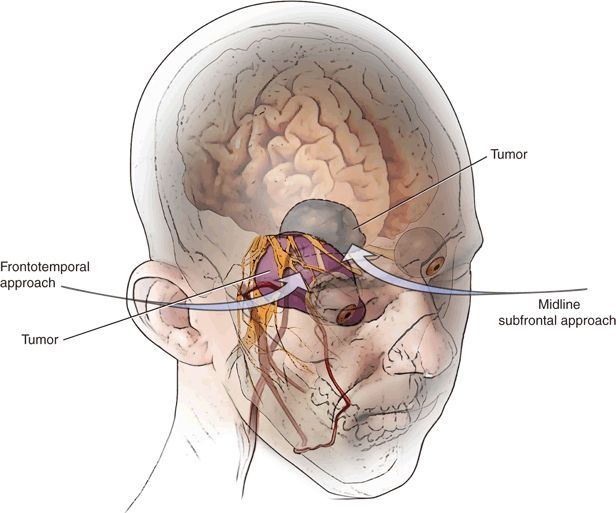
FIGURE 9.1 Illustration of three-quarter view demonstrating the frontotemporal or midline subfrontal approaches to the suprasellar cistern. The particular approach is chosen depending on the pathology and location of attachment.
Frontotemporal Approach
The frontotemporal approach offers a more anterolateral trajectory to the suprasellar cistern, with early detection of the carotid artery and pituitary stalk behind or lateral to the tumor (Fig. 9.2). It also offers the shortest distance to the region of the suprasellar cistern along the axis of the sphenoid ridge. For various tumors, a narrow or wide corridor can be chosen depending on the size of the craniotomy. Smaller lesions or those with limited attachment may allow a much smaller approach for access. For tumors with more superior extent, a frontotemporal orbitozygomatic modification may be chosen to allow the surgeon an inferior-to-superior trajectory to view and remove the most superior aspect of the tumor. This is especially helpful in tumors such as meningiomas and craniopharyngiomas, which may have significant suprasellar extension.
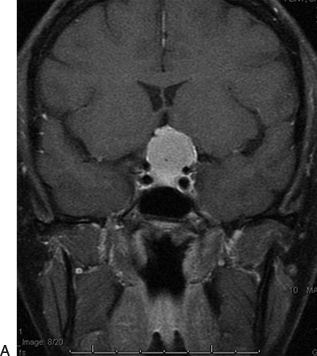
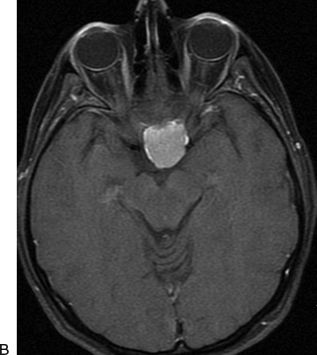
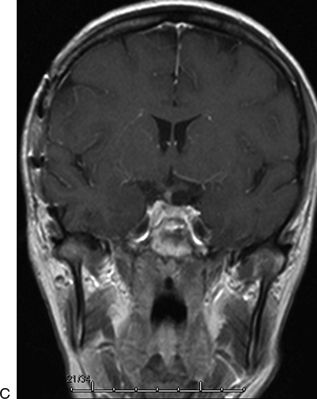
FIGURE 9.2 A 40-year-old woman presented with bilateral visual loss. This midline tumor has significant suprasellar extension. The tumor could be approached from either a frontotemporal or a subfrontal corridor. The frontotemporal approach was chosen here to enable early detection of the pituitary stalk and to provide the shortest distance to the suprasellar cistern. The frontotemporal approach also avoids any manipulation of the olfactory tracts, which could result in loss of the sense of smell. Preoperative T1 weighted post-contrast (A) coronal and (B) axial MR images demonstrate a meningioma with compromise of the optic chiasm. C. Postoperative image demonstrates complete removal.
Frontal Approach
The frontal approach to the suprasellar cistern may be unilateral or bilateral. It is chosen when the tumor is in the midline and the surgeon believes that a lateral approach is not necessary for identification of the carotid artery and pituitary stalk.
SURGICAL TECHNIQUE
Frontotemporal Approach
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


