Chapter 19 Complications of Surgery for Chronic Otitis Media
 Videos corresponding to this chapter are available online at www.expertconsult.com.
Videos corresponding to this chapter are available online at www.expertconsult.com.
PREOPERATIVE COUNSELING
Each patient should be informed of the indications, alternatives, and potential complications of surgery. We describe the diagnosis and procedure in layman’s terms. We explain the probability of success in simple ratios, such as “8 or 9 times out of 10 we close the perforation with a gain in hearing.” We then explain the potential risk of partial or total sensorineural hearing loss, dizziness, facial weakness, and other complications of mastoid surgery. Our group uses a handout that follows the example outlined by Sheehy1 to facilitate the discussion. With practice, this can be done in a way that does not sound negative. To do so, the patient must understand the goals of the surgery and how they are to be accomplished. The principal goal of chronic otitis media surgery is to eradicate infection. Correction of hearing loss is secondary and often is delayed until a second procedure.
LABYRINTHINE FISTULA SECONDARY TO CHRONIC OTITIS MEDIA
Labyrinthine fistulas are well-known complications of chronic otitis media. They are an unusual entity—but by no means rare—and are a serious operative hazard. An inexperienced surgeon may not foresee this and spoil an otherwise good result. The incidence of labyrinthine fistulas secondary to chronic otitis media in the modern literature ranges from 3.6%, reported by Palva and colleagues,2 to 12.9%, reported by Sanna and coworkers.3 Although the incidence of infectious complications of chronic otitis media, such as meningitis, sigmoid sinus thrombosis, and intracranial abscess, has declined, labyrinthine fistulas have had a remarkably stable prevalence of about 10%.4
The most common location of a labyrinthine fistula is the lateral semicircular canal in all published series. Most authors have reported isolated lateral semicircular canal fistulas in about 80% of cases, but this figure ranges from 57%5 to 90%.6 This preponderance shows that the lateral semicircular canal is more exposed to cholesteatoma than the rest of the labyrinth. The remainder of fistulas in most series involved the lateral canal plus one or more other sites.
There is a difference between a fistula and a bone erosion, although both appear as a blue-gray line under the microscope. A fistula is an abnormal communication between a hollow organ and the outside. With erosion, the bone is thin, but the layer next to the endosteum is still intact. Consequently, the labyrinth behaves differently than with a fistula.5 With a fistula, only the endosteal membrane separates the cholesteatoma matrix from the perilymphatic space. Pressure changes are transmitted directly to the membranous labyrinth causing the findings described in most reports (Table 19-1).
TABLE 19-1 Site of Labyrinthine Fistula and Associated Eye Movements
| Site of Fistula | Eye Movements |
|---|---|
| Lateral canal, postampulla | Horizontal, toward normal ear |
| Lateral canal, preampulla | Horizontal, toward diseased ear |
| Vestibule | Rotary, horizontal, toward diseased ear |
| Superior canal, ductal side | Rotary, toward normal ear |
| Posterior canal | Vertical, with an arc |
Adapted from McCabe BF: Labyrinthine fistula in chronic mastoiditis. Ann Otol Rhinol Laryngol 93(Suppl 112):138-141, 1983.
Many authors describe fistulas as small or large without quantifying these terms. Sanna and coworkers3 have classified fistulas as small (0.5 to 1 mm), medium (1 to 2 mm), and large (>2 mm). They found that most fistulas were large (74%), followed by medium (18.4%) and small (7.6%). Gacek5 also classified fistulas as either small or large with a cutoff of 2 mm in the greatest dimension. Although Gacek said that 2 mm was an arbitrary dividing point, he thought that the bony margin of the opening could support the cholesteatoma matrix in fistulas smaller than 2 mm. This forms a subtle separation from the endosteal membrane and allows relatively safe removal.
Although the surgeon should be prepared to deal with a fistula in any case of chronic otitis media, the length of symptoms may heighten suspicion. Sheehy and Brackmann,7 reporting on 97 cases of labyrinthine fistulas, noted that greater than 50% had a history of chronic otitis media for 20 years or longer. Ritter8 also noted that many of his patients had lifelong otorrhea, often dating back to childhood.
Vestibular symptoms increase the probability of a labyrinthine fistula. Sheehy and Brackmann7 noted that almost two thirds of patients were dizzy, and dizziness was constant in 12%. Ritter8 said that 76% of his patients complained of vertigo, which was usually brief, lasting seconds to minutes. Ostri and Bak-Pedersen,9 with 20 cases, and Gormley,10 with 35 cases, noted frank vertigo in 65% of patients. McCabe4 reported the highest prevalence of vestibular symptoms of any larger series: 90% of 79 cases. In addition, there was a high prevalence of positive fistula tests (72%). McCabe gave an outstanding description of the test along with the anticipated eye movements for different fistula locations (see Table 19-1). Dizziness is much less common in cases of chronic otitis media without fistulas. One review found the prevalence to be 15% in such cases, and more related to age than to duration of disease.11
With a positive fistula test of a postampullary lateral canal fistula, air compression into the ear causes conjugate deviation (not nystagmus) of the eyes to the opposite ear; this displaces the endolymph and cupula toward the vestibule. There is nystagmus toward the tested ear with sustained pressure. If the pressure is pulsed, there is still deviation to the opposite ear, but the eyes drift back to the midline with pressure release. If the fistula is located at the junction of the lateral canal ampulla and vestibule (preampullary region), positive pressure displaces the cupula away from the vestibule with deviation of the eyes toward the diseased ear. Positive pressure on a fistula of the vestibule moves the horizontal and superior canal ampullae, causing rotary-horizontal eye movements toward the diseased ear.4
Pressure changes are not the only way for a fistula to cause vestibular symptoms. Extension of infection into the perilymph is rare, but causes purulent labyrinthitis with complete loss of vestibular function. Serous labyrinthitis is more common and occurs when only inflammation and bacterial toxins enter the labyrinth.8
Sensorineural hearing loss is another clue that there might be a fistula. Sheehy and Brackmann7,11 found an impairment in more than half of their fistula cases compared with only 20% of nonfistula cases. Sensorineural levels were more often diminished in patients with extensive fistulas at sites other than the lateral canal. Preoperative anacusis existed in 12%.7 Ritter8 also found decreased sensorineural levels in his series—70% had decreased bone conduction, which averaged 26 dB. Speech discrimination was less than 80% in 20% of patients, and 30% were deaf. Farrior12 reported nonserviceable hearing in 13% of 31 cases, whereas Ostri and Bak-Pedersen9 noted anacusis in 15%.
Preoperative facial weakness, although rare, is more common with fistulas than without fistulas: 4% versus 1%.7 All series report a high incidence of facial nerve dehiscence, including Gormley (27%),10 Ritter (36%),8 Sheehy and Brackmann (50%),7 and Ostri and Bak-Pedersen (55%).9 There is a greater potential for intraoperative nerve injury with fistulas.
INTRAOPERATIVE MANAGEMENT OF LABYRINTHINE FISTULAS
The suitability of leaving cholesteatoma matrix over a fistula versus removing it remains a passionate controversy. Walsh13 and Baron14 drew attention to this in 1953 during a symposium on the management of cholesteatomas. Walsh13 thought the cholesteatoma had a chemical osteolytic effect and advocated removal in all cases. Baron14 believed that bone erosion from cholesteatoma was mainly from pressure, so exteriorization of the sac was sufficient. Various techniques have been promoted since then.
All authors support three concepts with labyrinthine fistula treatment, as follows:
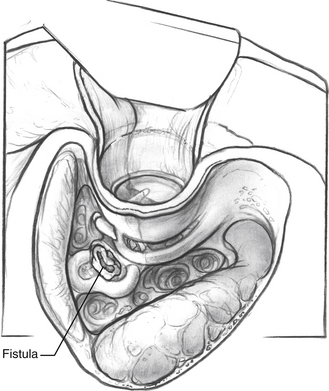
FIGURE 19-1 Fistula of the lateral semicircular canal secondary to cholesteatoma. The facial recess is opened.
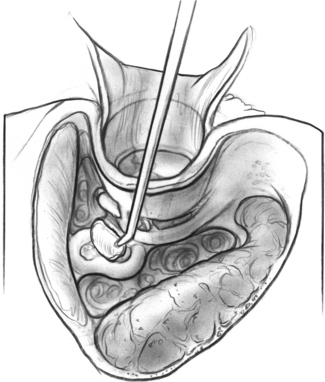
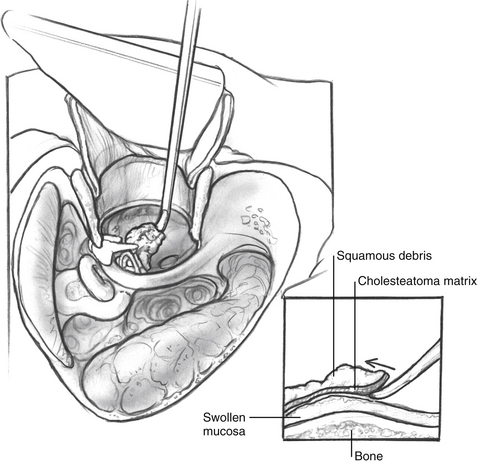
FIGURE 19-2 Fascia placed over lateral semicircular canal fistula after removal of cholesteatoma matrix.
A promontory cochlear fistula is one of the few absolute indications for radical mastoidectomy because postoperative sensorineural hearing loss is likely. Sheehy and Brackmann7 had a 56% incidence of severe or total sensorineural hearing loss when they attempted matrix removal from extensive fistulas. Gacek5 reported a partial to profound hearing loss in three cases in which he removed matrix from cochlear fistulas. Gacek believed that the membranous semicircular canals and their ampullae have thicker, more rigid walls than Reissner’s membrane or the basilar membrane, and are less likely to rupture with manipulation. In addition, the cochlear duct is in the outermost portion of the bony cochlea, so it is more closely in contact with the overlying matrix than the membranous labyrinth is elsewhere.
With regard to the isolated lateral canal fistula, some authors always leave the matrix alone because of the risk to the inner ear.8,16,17 Ritter8 recommended a canal wall down mastoidectomy and leaving the matrix over the fistula. He reported hearing loss in 47% of cases when he removed the matrix compared with 22% when it was undisturbed. He left 80% of fistulas uncovered after matrix removal; this increases the possibility of an inner ear injury. Nevertheless, the senior author (R.J.W.) agrees with this philosophy—especially when the fistula looks larger than 2 mm on computed tomography (CT) scan.
Other surgeons perform a canal wall down tympanomastoidectomy and matrix removal in cases of isolated lateral canal fistulas. Farrior12 prefers a single-stage operation, but cautions against matrix removal from an acutely inflamed or better hearing ear. Palva and associates2 also use this technique. Their preference is due to cases of periodic otorrhea or persistent vertigo when the matrix was left in place. All cases in which the matrix was removed and the fistula was covered healed without further otorrhea or vestibular symptoms.
According to Gacek,5 the decision to remove matrix is based on the following factors:
Sheehy and Brackmann7 have an eclectic approach to lateral canal fistulas. They consider all of the factors mentioned by Gacek5 except for the final one about mechanisms of bone erosion. They prefer the intact canal wall tympanomastoidectomy with removal of the matrix over the fistula in a second operation 4 to 6 months later, after the ear is healed, and any infection is gone. They remove the matrix at the first stage in selected cases. It must be a small lateral canal fistula in a noninfected ear with normal bone conduction; however, they do not define “small.” When there is a fistula in a much better hearing ear, Sheehy and Brackmann,7 similar to Farrior,12 do a canal wall down procedure to avoid hearing loss or a second operation. They leave the matrix over the fistula when doing this.
Sanna and associates3 and Gormley,10 reporting on Smyth’s series of labyrinthine fistulas, have nearly the same approach as Sheehy and Brackmann.7 They prefer a staged intact canal wall tympanomastoidectomy with matrix removal from the fistula during the second surgery. Sanna and associates3 do a canal wall down mastoidectomy without matrix removal in patients with an only hearing ear, in patients with a large external auditory canal defect, in patients with multiple fistulas, or in elderly patients. In contrast, Ostri and Bak-Pedersen9 encourage matrix removal, even with large fistulas, using a one-stage intact canal wall tympanomastoidectomy. Ostri and Bak-Pedersen report that they have hearing improvement in most of their cases, and that anacusis is uncommon.
There are a variety of surgical procedures for labyrinthine fistulas. These procedures range from always exteriorizing the disease and leaving matrix over the fistula to removing the matrix over large fistulas during one closed mastoid operation.8,9 Other authors have an approach between these extremes.3,5,7,10,12,21
Several technical points warrant mention. As stated, matrix removal should be at the end of the surgery. One should see if the matrix is attached to the underlying membranous labyrinth, and if so, stop dissecting.5 Conversely, Bellucci22 does not think it can get attached, and that it always can be elevated under high magnification. Bellucci believes that damage to the labyrinth results directly from instruments such as the suction. Farrior12 agrees and believes that no instrument should touch the fistula. Instead, he recommends using a strip of cellulose sponge for this part of the dissection. It is soft, but also slightly abrasive, which helps with removal from the bone. Irrigation should be gentle, but it is still important to prevent contamination by infected debris.
Hearing preservation is an important goal of labyrinthine fistula treatment. Postoperative hearing results vary among authors, and direct comparisons are impossible because of differences in surgical approaches and disease extent. Gormley10 reported a 3.3% incidence of anacusis in ears that were functioning before surgery. Ostri and Bak-Pedersen9 had a 5% incidence, whereas Sanna and associates3 separated their results between open (9.5%) and closed (2.6%) mastoidectomy groups. Gacek5 had a 14% incidence of anacusis, all in ears in which he attempted matrix removal from a cochlear fistula. Sheehy and Brackmann7 noted severe or total loss of hearing in 8% of lateral canal fistulas, and in 56% of fistulas involving other sites—predominantly cochlear fistulas. Law and colleagues21 reported postoperative anacusis in 22% of their cases.
Decreased postoperative sensorineural levels or discrimination scores without total hearing loss are reported as follows: Sanna and associates (4% with closed mastoidectomy, 6.4% with open mastoidectomy),3 Gacek (7%),5 Ostri and Bak-Pedersen (17%),9 and Ritter (37%).8 Sensorineural hearing loss from surgery is common, and this must be explained beforehand to any patient who may have a fistula.
Finally, extensive labyrinthine destruction does not invariably cause hearing loss. Phelps23 described a patient with an extensive cholesteatoma involving the vestibule along with the basal and middle turns of the cochlea who still had hearing, but it was lost during surgery. We saw something similar in four patients with slow-growing cholesteatomas. Bumstead and coworkers24 reported four cases of extensive labyrinthine destruction in which vestibular function was gone, but the hearing remained, even after surgery. They suggested that the inflammatory response sealed the cochlea and protected it. There is at least one report of a labyrinthine fistula with preoperative anacusis and a large hearing gain after surgery.25 The hearing loss was thought to be from serous labyrinthitis that later resolved.
IATROGENIC LABYRINTHINE FISTULA
Although iatrogenic labyrinthine injury and hearing loss is always possible, it is infrequent. The three sites at the most risk during chronic otitis media surgery are the lateral semicircular canal, promontory, and oval window.26 Similar to a cholesteatoma fistula, an iatrogenic breach of the membranous labyrinth is treacherous, but the hearing is not always lost. Multiple case reports from the fenestration era show this to be the case.27–30 That said, the surgeon must recognize and repair the injury.
Palva and associates31 reported iatrogenic injury to the lateral canal in the absence of a cholesteatoma fistula in 0.1% of chronic otitis media cases (2 of 2192). One case had stable hearing, whereas the other had an approximately 20 dB bone conduction loss in the speech frequencies. Jahrsdoerfer and colleagues32 described two episodes of drilling into the lateral canal without hearing loss. A more recent review by Canalis and coworkers33 reported a 0.08% incidence of this mishap, similar to Palva and associates.31 They had several observations about this injury.33 There was an acute, moderately severe sensorineural loss in cases that ultimately had a favorable outcome—hearing returned close to preoperative levels after 3 to 6 weeks. A permanent mild high-frequency loss was common, but speech discrimination scores returned to normal. Tinnitus was rare. Vertigo and nystagmus occur as anticipated, but commonly last beyond the usual period of central compensation. Patients sometimes have unsteadiness, positional vertigo, and spontaneous nystagmus 1 to 2 years after surgery. This is consistent with a partial labyrinthine injury along with continued neurosensory activity.
How is hearing preservation possible with labyrinthine injuries? There are theories, but no conclusions. Canalis and coworkers33 believe that there is a better outcome when the lateral canal is opened on its posterior limb where symptoms may be from hemorrhage and serous labyrinthitis. Injuries near the vestibule would be more likely to cause contamination of the perilymph by endolymph, which causes permanent damage. They suspect that their cases of cochlear preservation were due to local changes at the fistula. The walls of the membranous labyrinth might collapse from a loss of fibrovascular support within the perilymphatic space. This, along with a sudden loss of endolymph, collapses the membranous labyrinth and seals it. Jahrsdoerfer and colleagues32 have a different theory. They think there is a closure of the pars superior from the pars inferior near the utriculoendolymphatic valve. An acute loss of endolymph from the vestibule causes the utricular wall to collapse, closing the valve area and protecting the cochlea from decompression. They recommend sealing iatrogenic fistulas with a fascia plug. Bone wax34 and muscle plugs33 are also used.
Accidental opening of the inner ear is more common at the oval window than at the lateral semicircular canal. Palva and associates2 had a 1.4% incidence of this iatrogenic fistula, and of their 12 cases, 11 occurred at the oval window.2 Two had complete avulsion of the footplate, three had dislocation, and the rest were fractures without dislocation. There were no drastic hearing losses, despite preoperative infections, but three cases did have depressed bone conduction thresholds several months later. In a 5-year follow-up report, Palva and associates31 opened the oval window once in an additional 1362 cases, for an overall incidence of 0.5%. This is still higher than the rates of lateral semicircular canal injury mentioned earlier.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


