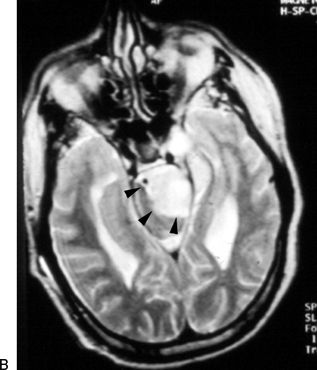
FIGURE 38.1 A. Axial MRI T1 with gadolinium showing the well-defined tumor left of the midline with extension into the left Meckel’s cave (arrowheads). B. Axial T2 shows tumor and brainstem border (arrowheads). There is no edema within the brainstem. The ventricles are enlarged in this case.
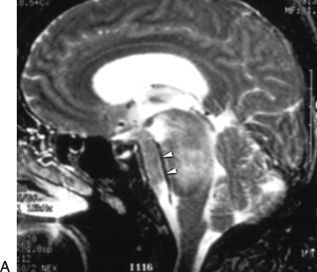

FIGURE 38.2 A. Sagittal T2 MRI shows encasement of the basilar artery within the tumor (arrowheads). B. There is extensive high signal within the brainstem indicating invasion of the pia by the tumor producing edema (asterisk); arrowheads indicate the tumor–brainstem interface; T, tumor.
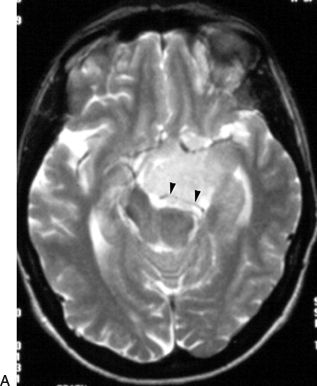
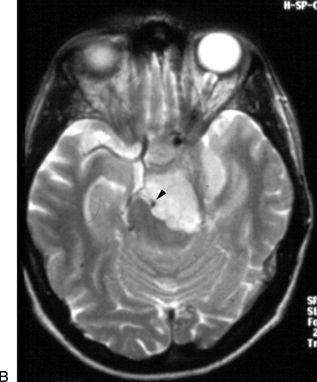
FIGURE 38.3 Axial T2 MRI showing that the tumor surrounds the posterior cerebral artery (arrowheads) (A) and the basilar artery (arrowhead) (B).
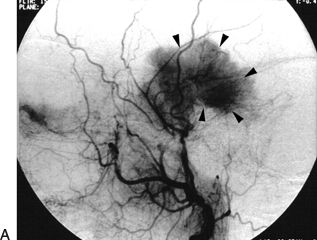

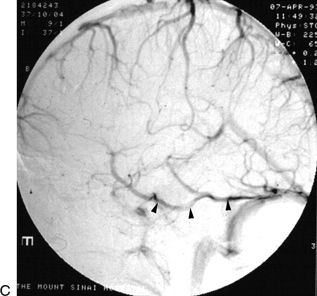
FIGURE 38.4 A. Cerebral arteriogram, external carotid injection showing the blood supply to the tumor from the middle meningeal artery (arrowheads). B. The basilar artery and its branches are displaced by the tumor (arrowheads).Figure 38.4(Continued) C. The venous phase shows a large temporal draining vein (arrowheads) coursing along the inferior surface of the temporal lobe to drain into the tentorium and then into the sigmoid–transverse junction. This venous channel must be preserved while the tentorium is being incised.
SURGICAL TECHNIQUE
Anesthesia, Intraoperative Neurophysiologic Monitoring, and Positioning
General intravenous anesthesia is used during the tumor phase of the operation because of the need for intraoperative neurophysiologic monitoring. Intra-arterial and venous lines are place. Continuous neurophysiologic monitoring of cranial nerves VII and VIII, somatosensory and motor evoked potentials, and transcranial facial nerve evoked potentials are very helpful during these operations. Lumbar spinal drains and external ventricular drains are usually not necessary. Broad-spectrum antibiotics and anticonvulsant prophylaxis are administered at the beginning of the operation.
The patient is positioned supine with a soft roll under the ipsilateral shoulder, and the head is turned to the contralateral direction about 60 degrees and stabilized in a three-point headrest (Fig. 38.5). The extent of the head rotation is for the surgeon to be able to visualize and access both the base of the tumor along the petrous ridge and the surface of the tumor pressing into the brainstem. The head is kept elevated relative to the chest and body to facilitate venous drainage.
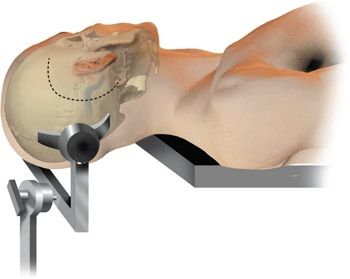
Figure 38.5 The patient is positioned with the head turned away from the side of the tumor about 60 degrees. The surgeon sits behind the patient. The incision is “C” shaped such that the posterior limb is about 1 inch posterior to the tip of the mastoid.
Scalp Incision and Soft Tissue Flaps
A large “C”-shaped flap is used located above, behind, and below the ear and centered at the ear (Fig. 38.5). The posterior limit of the incision should extend about an inch posterior to the mastoid tip. The scalp flap is elevated up to the external ear canal, which has to be carefully identified and separated from the bony ear canal. The muscle flaps are elevated superiorly and inferiorly, by making an incision horizontally separating the temporalis muscle from the nuchal muscles. The posterior temporal line, which is the posterior extension of the zygomatic arch, is identified, which separates the floor of the middle cranial fossa from the mastoid.
Craniotomy and Bone Work
The opening of the bone can be done in two ways: One way is to perform a craniotomy first and then a retrolabyrinthine mastoidectomy, and the other way is to perform the mastoidectomy first and then use that as the starting point for the craniotomy. In order to perform the craniotomy first, one burr hole is made above the sigmoid–transverse junction (Fig. 38.6A), at the junction of the squamosal suture with the posterior temporal line. The second burr hole is made below the sigmoid–transverse junction at the asterion (Fig. 38.6A and B). Since there is a deep groove housing it, the sinus can be readily injured here. Therefore, a bony trench is drilled joining the two burr holes. Once the dura has been separated from the bone, a combined temporal and posterior fossa craniotomy is made with the high-speed craniotome following the dotted line in Figure 38.6A. Traversing the posterior part of the transverse sinus with the saw is safe because there is no bony groove. The retrolabyrinthine mastoidectomy is now carried out unroofing the sigmoid sinus down to the jugular bulb and the superior petrosal sinus.
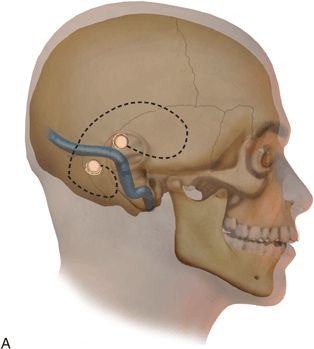
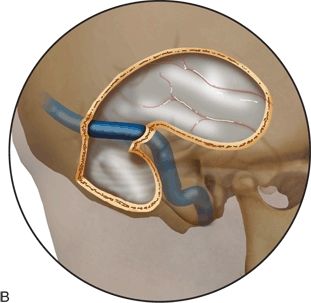
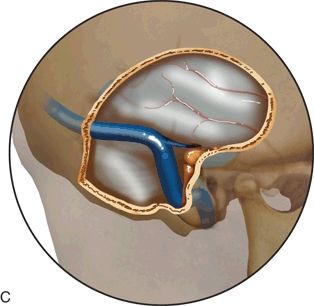
FIGURE 38.6 A–C. Sequence of the bony opening starting with the craniotomy. The burr holes A and B are made above and below the transverse/sigmoid junction as described in the text. In this sequence, the mastoidectomy is performed later in the bone removal.
In the other option, the mastoidectomy is performed first, skeletonizing the labyrinth and exposing the sigmoid sinus entirely from the sigmoid–transverse junction down to the jugular bulb. The subtemporal and presigmoid dura are exposed so that the superior petrosal sinus and the endolymphatic sac are fully unroofed. It is very important that the unroofing of the sigmoid sinus be carried out all the way down to the jugular bulb and the thin ridge of bone between the two structures be drilled down carefully. This reduces the venous bleeding from the area of the jugular bulb that can occur when the sigmoid sinus is retracted posteriorly during the tumor resection phase. The labyrinth must be fully skeletonized so that the maximal exposure of the dura between the sigmoid sinus and the posterior semicircular canal can be achieved. The petrous bone can be drilled down further anteriorly by performing a partial or complete labyrinthectomy and even by drilling down the cochlea to provide a larger exposure while minimizing brain retraction. A combined temporal and posterior fossa craniotomy is started at the mastoidectomy defect. The anterior extent of the temporal craniotomy should extend to above the external ear canal. The inferior extent of the posterior fossa craniotomy should be almost down to the foramen magnum. It must provide enough temporal exposure to allow for placement of a temporal lobe retractor without limiting the retractor by the bone edge of the craniotomy. Posteriorly, the craniotomy must extend far enough behind the sigmoid sinus to allow the sinus to be retracted posteriorly and also to allow the surgeon to perform a retrosigmoid exposure should it be needed in addition to the presigmoid exposure (Fig. 38.7).
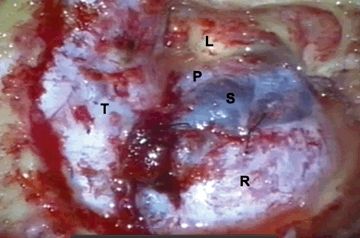
Figure 38.7 Intraoperative view of a right-sided exposure. The vertex is to the left, and the ear is superior. Dural exposure after completion of the bone work. (T, temporal lobe dura; R, retrosigmoid dura; S, sigmoid sinus; P, presigmoid dura; L, labyrinth.)
Dural Exposure and Opening
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


