Fig. 5.1
Embryologic development of the lip (from Moore KL, Persaud TVN. The Developing Human: Clinically Oriented Embryology, 5th ed. Philadelphia: W.B. Saunders; 1993. Copyright Elsevier 1993)
Fig. 5.2
Embryologic development of the palate (from Moore KL, Persaud TVN. The Developing Human: Clinically Oriented Embryology, 5th ed. Philadelphia: W.B. Saunders; 1993. Copyright Elsevier 1993)
Definition
Due to their differing embryologic development, cleft lip with or without cleft palate (CL/P) is an entity distinct from isolated cleft palate (CP). Clefting of the lip and primary palate results from incomplete fusion of the maxillary and medial nasal processes, whereas clefting of the secondary palate results from failure of fusion of the palatal shelves. Cleft lip/palate may be defined by the laterality of clefting (left, right, or bilateral) or by whether the cleft is incomplete or complete. In a complete cleft lip, no tissue connects the medial and lateral lip segments (Fig. 5.3). In an incomplete cleft of the lip, a band of tissue of variable width (Simonart’s band) connects the medial and lateral lip segments in the superior portion of the lip (Fig. 5.4). Clefting of the secondary palate occurs from the incisive foramen posteriorly and may involve the soft palate alone or both the soft and hard palate (Fig. 5.5). A submucous cleft palate is identified as a bifid uvula, notching of the posterior hard palate, and a zona pellucidum within the soft palate [5] (Fig. 5.6). In a submucous cleft palate, the mucosa of the soft palate is intact but the muscular levator sling is disrupted, with the levator veli palatini aberrantly inserting onto the posterior edge of the hard palate.


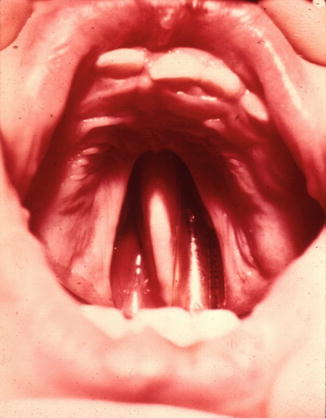

Fig. 5.3
Complete unilateral cleft lip and palate
Fig. 5.4
Incomplete unilateral cleft lip and palate
Fig. 5.5
Cleft of the secondary palate
Fig. 5.6
Submucous cleft palate
Incidence
Cleft lip/palate has variable incidence depending upon race and gender of the patient. The relative occurrence of CL/P is a 6:3:1 ratio of left: right: bilateral. Cleft lip/palate is more common in males compared to females. Race plays a role in the incidence of CL/P as well, with Native Americans and Asians having the highest incidence (3.6 and 2.1 per 1,000 live births, respectively). The incidence of CL/P in Caucasians is 1.0 per 1,000 live births, and that in African Americans is 0.5 per 1,000 live births [6]. Unlike CL/P, isolated cleft palate has a uniform incidence across all races (0.5 per 1,000 live births). CP occurs more frequently in females than in males.
History
The first cleft lip repair to appear in the world’s literature was that performed by a Chinese surgeon on a poor farm boy in the fourth century AD. The patient, Wei Yang-Chi, would later become the Governor General of six Chinese provinces, an extraordinary historical testament to the social impact of cleft surgery. For more than a millennium thereafter, cleft lip surgery did not advance much beyond simple cauterization or paring of the cleft edges with simple approximation of the lip segments. Attempts to restore adequate lip length began with the use of curved incisions, as first described by von Graefe and later by Rose and Thompson, and later progressed to the use of rectangular (LeMesurier) and later triangular (Tennison and Randall) flaps from the lateral lip. The rotation-advancement technique, introduced by Millard in 1955, was based on the understanding that the entire Cupid’s bow is invariably present on the medial lip segment and is rotated superiorly. Downward rotation of the entire philtral complex, noted Millard, levels the Cupid’s bow and opens a gap in the superior lip into which a flap derived from the lateral lip element may be advanced. The rotation-advancement technique has been modified by many cleft surgeons since its introduction and remains widely used throughout the world.
The first anecdotal report of cleft palate repair in 1766 is attributed to LeMonnier, a French dentist. He simply placed several sutures across the cleft, cauterized the mucosa along the cleft margin, and then tied the sutures. In 1819, Dr. Philibert Roux reported repair of the cleft soft palate of a Canadian medical student named John Stephenson. Bernard von Langenbeck is credited with first describing closure of hard palatal clefts by elevating full-thickness mucoperiosteal flaps in 1861. His technique of raising the mucoperiosteum from the posterior edge of the cleft hard palate to the posterior aspect of the alveolus is still commonly used today in the procedure that bears his name (Fig. 5.7a–c). In the early twentieth century, cleft palate surgeons began to focus their attention on means by which to improve speech outcomes by lengthening the palate at the time of repair. The most popular of these techniques, the V–Y pushback technique described by Wardill, and Kilner, remains in widespread use today. In 1978, Leonard Furlow of the University of Florida first described a novel technique of velar repair utilizing opposing mirror-image Z-plasties of the oral and nasal mucosa. The technique offered several advantages over straight-line techniques. Use of Z-plasty closure provided for palatal lengthening without the need for pushback procedures, and transposition of the posteriorly based myomucosal flaps reoriented the levator muscle bundles into anatomical position, reconstructing the levator sling [7] (Fig. 5.8a, b).
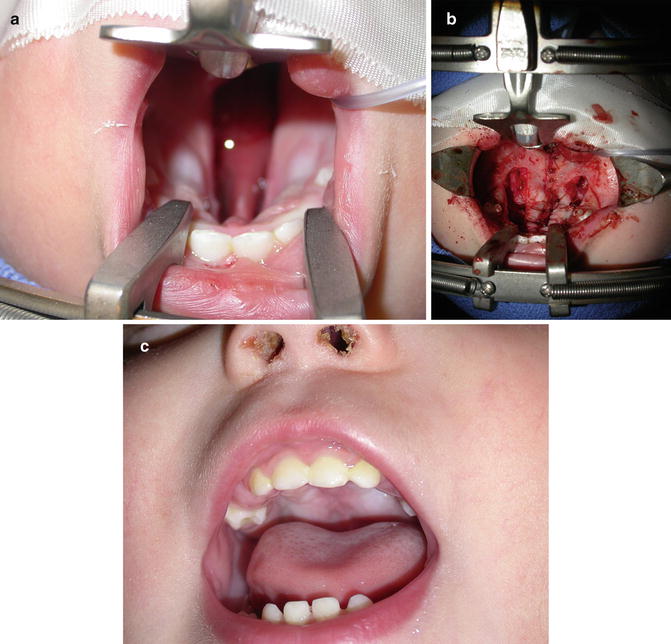
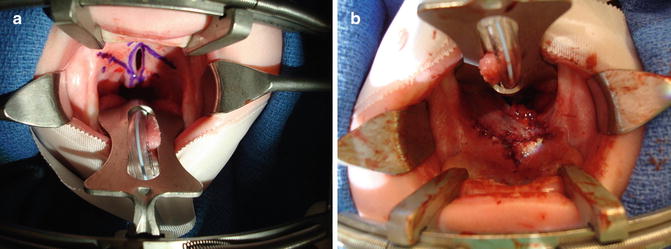
Fig. 5.7
(a–c) Von Langenbeck cleft palate repair (a and b demonstrates the surgeon’s view from the top of the stretcher with the patient lying supine.)
Fig. 5.8
(a and b) Furlow cleft palate repair (surgeon’s view from the top of the stretcher)
Heredity
Genetic analyses have shown that nonsyndromic cleft lip with or without cleft palate has complex inheritance patterns, and there is substantial data to support an etiologic role for genetic factors. Although segregation analysis has provided significant insights, the mode of inheritance for nonsyndromic orofacial clefts remains uncertain. It is widely believed that cleft lip with or without cleft palate is a heterogeneous disorder and that 3–20 genes may interact with one another and/or with environmental factors to produce orofacial clefting [8, 9]. Certainly, a family history is one of the strongest risk factors for cleft lip/palate and cleft palate alone. The risk of cleft lip/palate in first-degree relatives is approximately 4 %, increasing to 10 % when two first-degree relatives are affected. For cleft palate alone, the overall risk in first-degree relatives is approximately 2 %, increasing to 8 % when two first-degree relatives are affected [10].
Etiology
As noted above, there is clear evidence for a genetic etiology of nonsyndromic orofacial clefting. In addition, several environmental factors have been implicated, including pharmacologic agents (retinoids, anti-convulsants, folate antagonists, benzodiazepines, and corticosteroids), maternal diseases (diabetes mellitus), and maternal smoking.
Associated Conditions
Understanding the conditions associated with syndromic orofacial clefts are essential to proper clinical management. Over 400 distinct syndromes associated with orofacial clefts, some quite rare, have been described. Associated abnormalities are seen in 25–35 % of clefts of the lip with or without cleft palate in the fetal and newborn period, and yet only 10–15 % of older children with cleft lip with or without cleft palate have associated defects, indicating that many infants with associated severe malformations do not survive infancy [11, 12]. The most common syndrome associated with cleft lip with or without cleft palate is van der Woude syndrome, an autosomal dominant condition most often caused mutations in interferon inhibiting factor 6 (IRF6) [13]. In addition to orofacial clefts, the syndrome often presents with hypodontia and lower lip pits (Fig. 5.9). CHARGE Association (coloboma, heart defect, atresia choanae, retarded growth and development, genital anomalies and hypogonadism, and ear anomalies and deafness), an autosomal dominant condition most often associated with mutations in CHD7, is the second most common syndrome associated with cleft lip with or without cleft palate [14].




