Fig. 719 The classification of mastoidectomies and reconstructive methods proposed by Müsebeck. a Antrostomy with opening of the antrum, leaving most of the ear canal intact. b Mastoidectomy with a preserved ear canal wall and ventilated cavity. c Meatoplasty. The ear canal is partly or totally removed, but reconstructed. The cavity is ventilated (arrow). d Mastoid obliteration after removal of the bony ear canal wall. e Radical operation with an open cavity
Another classification, including mastoidectomy types as well as their reconstruction, and dividing the procedures into atticotomy, atticoantrotomy, cortical mastoidectomy, tympanomastoidectomy, Bondy’s operation, the conservative radical operation, and the classical radical operation, is also used. These procedures are defined and illustrated in Chapter 1 above, but this classification neither includes nor sufficiently describes the methods of reconstruction.
Some general terms have become widely used in connection with reconstruction, such as open, as opposed to closed techniques, indicating the outcome of the reconstruction. Another generally accepted classification is related to the region to be reconstructed.
Closed and Open Techniques
Recognizing that reconstruction of the middle ear cleft often cannot be performed as planned or desired, but is a compromise between various principles and methods; and recognizing that the outcome of a reconstruction technique does not always correspond to its intention, the author proposes a new flexible classification of open and closed techniques, allowing transition from the closed to the open technique. This classification also includes the situation in the attic.
The closed technique includes and describes all procedures required to avoid a cavity. However, there is a gradual transition to open techniques.
In canal wall–up mastoidectomy situations, the closed technique includes ventilation (repneumatization) of the cavity behind the preserved ear canal wall (Fig. 720a), or total obliteration (Fig. 720b), or partial obliteration of the cavity behind the preserved ear canal wall, with ventilation of the attic (Fig. 720c).
In canal wall–down mastoidectomy situations, the closed techniques include the reconstruction of the ear canal wall with ventilation (Fig. 721a) with total or partial obliteration of the cavity (Figs. 721b,c). The outcome of the reconstruction of the ear canal wall with hard materials, such as bone or hydroxyapatite, closely resembles closed techniques after a canal wall–up mastoidectomy. The outcome of reconstructions of the ear canal wall with soft tissues, such as fascia, muscle or cartilage, or obliteration of the cavity with soft tissues without ear canal wall reconstruction, often includes a meatoplasty, resulting in some widening of the ear canal. Despite the meatoplasty and a widened ear canal, the obliterations are closed cavity techniques, mainly because a cavity is avoided.
The cavity including the attic can be totally obliterated (Fig. 722a), and the attic can be ventilated (Fig. 722b) or can remain as an open cavity (Fig. 722c). This latter technique is still a closed technique, because a cavity is avoided, even though it includes some elements of the open technique, e. g., the meatoplasty with widened ear canal and the open attic.
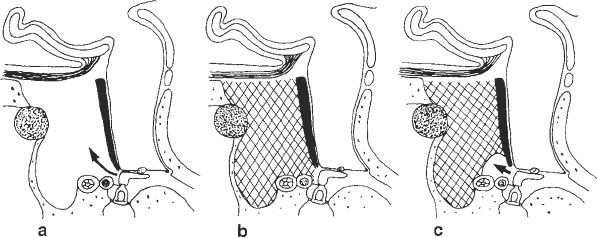
Fig. 720 The classification of closed techniques after canal wall–up mastoidectomy. a The ear canal wall is preserved and the cavity is ventilated (arrow). b The ear canal wall is preserved and the cavity is obliterated, including the attic. c The ear canal wall is preserved, the cavity is partly obliterated, and the attic is ventilated (arrow)
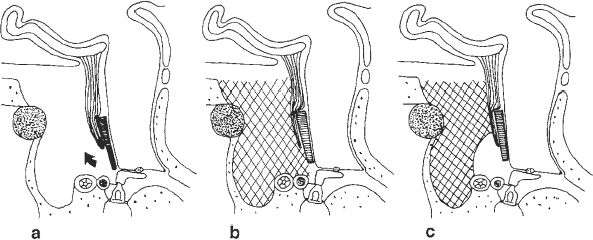
Fig. 721 The classification of closed technique after a canal wall–down mastoidectomy with reconstruction of the ear canal wall. a The ear canal is reconstructed, supported with a Palva flap, and the cavity is ventilated (arrow). b The ear canal wall is reconstructed and the cavity is completely obliterated. c The ear canal wall is reconstructed. The cavity is partly obliterated and the attic is ventilated
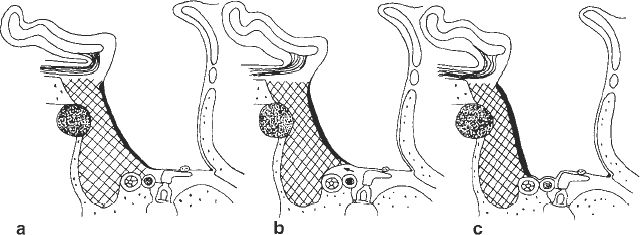
Fig. 722 The classification of closed techniques after a canal wall–down mastoidectomy with obliteration and reconstruction of the ear canal with soft tissues, or with obliteration alone. a The ear canal is widened and the cavity and the attic are obliterated. b The cavity is obliterated and the attic is ventilated (arrow). c The cavity is obliterated and the attic is open
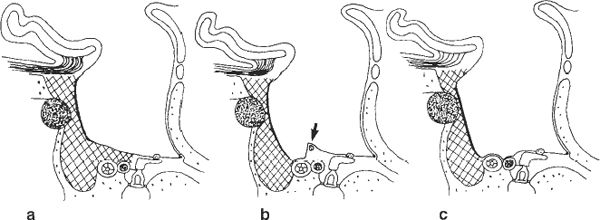
Fig. 723 The classification of closed techniques after canal wall–down mastoidectomy with obliteration of the cavity with soft tissue and some meatoplasty. The ear canal is considerably widened. a The cavity and the attic are obliterated. b The cavity is obliterated, and the attic is ventilated behind a preserved bridge (arrow). c The cavity is obliterated and the attic is open. A gradual transition to the open technique is evident
If the ear canal is further widened, then despite an obliteration the result increasingly resembles an open technique (Fig. 723). The same is the case if less extensive obliteration is performed. Large obliterated “cavities” often occur some years after obliteration. The cavities gradually become larger due to atrophy of the obliterating material, particularly muscle, or fibroplasia in the cartilage used for obliteration, or both.
The open technique is defined as resulting in a cavity, often combined with a meatoplasty, either with no attempt to obliterate the cavity (Fig. 724a), or with partial cavity obliteration alone (Fig. 724b) e. g., of the perilabyrinthine space or the mastoid tip. The attic is usually part of the open cavity, but it can be ventilated (Fig. 724c) or obliterated (Fig. 724d). The latter situation is also defined as an open cavity technique because the cavity is still not avoided.
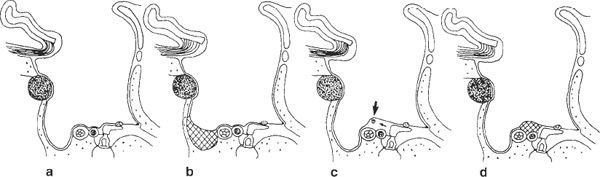
Fig. 724 The classification of open techniques after canal wall–down mastoidectomy. a The entire cavity, including the attic, is covered with skin. b The perilabyrinthine part of the cavity is partially obliterated. c The attic is ventilated behind a preserved bridge (arrow), and the remaining cavity is open. d The attic is obliterated, and the remaining cavity is open
This classification into closed and open techniques according to the outcome of the reconstruction takes the degree of obliteration into consideration for several reasons:
1. In canal wall–down mastoidectomy, the primary obliteration of the cavity is seldom complete, even if such an obliteration is desired and performed. A small cavity is often the immediate postoperative result (Tos 1969, 1977, 1978b). Widening of the ear canal in the form of a small meatoplasty is therefore, in the author’s opinion, an important and necessary improvement of an obliteration technique.
2. The size of the primarily obliterated cavity when soft tissue is used increases with time, making the degree of obliteration less and less complete. Meatoplasty with widening of the ear canal is increasingly necessary, and the closed technique becomes an open technique during the increase in the cavity size.
3. In most previous open radical cavities reconstructed into a closed cavity using obliteration techniques, a meatoplasty was originally performed. All these closed techniques thus already have a widened ear canal and resemble the situation illustrated in Figures 722 and 723.
The four groups of closed cavity techniques can be summarized as follows:
1. Closed technique in canal wall–up mastoidectomy with ventilation or obliteration of the cavity (Fig. 720).
2. Closed technique in canal wall–down mastoidectomy with reconstruction of the ear canal wall and ventilation or obliteration of the cavity (Fig. 721).
3. Closed technique in canal wall–down mastoidectomy with cavity obliteration (Fig. 722) and ear canal reconstruction using soft tissues, subdivided into an obliterated, ventilated, or an open attic.
4. Closed technique in canal wall–down mastoidectomy with cavity obliteration, subdivided into an open, ventilated, or obliterated attic (Fig. 723).
After reconstruction of the ear canal wall with solid material and obliteration with soft tissues, atrophy of the obliteration material leads to the formation of a retraction pocket (Fig. 725), similar to the retraction pockets seen in canal wall–up mastoidectomies (Chapter 6). This is also the result if ventilation of the cavity behind the reconstructed ear canal is disturbed (Fig. 720a). After ear canal wall reconstruction and obliteration with soft tissues, the atrophy of the obliteration material leads to diffuse retraction of the entire soft ear canal wall and results in a small cavity with a widened ear canal (Fig. 726).
This classification does not describe how the cavity has been obliterated and the ear canal wall reconstructed, but indicates whether the ear canal has been reconstructed with solid tissue or not. The various surgical methods used to achieve the closed or open techniques are described separately.
As long as the classification into closed and open techniques is related to the situation pertaining to cavity or noncavity conditions, the classification is simple. However, if the various conditions in the attic are included, then the classification becomes complicated, with many variations. The various methods of reconstructing the attic used, and their relation to reconstructions of the tympanic cavity, therefore have to be subclassified separately in order to understand the techniques being used.
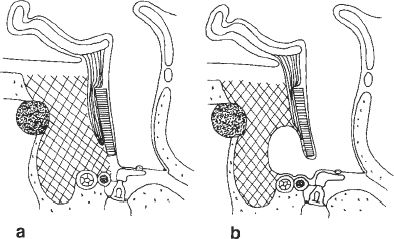
Fig. 725 Reconstruction of the ear canal with hard tissue and obliteration of the cavity with soft tissue. a Early postoperative condition. b Late after the operation, there is a retraction pocket behind the new ear canal when atrophy or fibroplasia of the obliterating material occurs
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


