Chapter 151 Choroidal Metastases
Introduction
Choroidal metastases are the most common of adult intraocular tumors.1,2 Autopsy studies suggest that approximately 10% of cancer patients have ocular metastases, most frequently to the choroid.1,3 Pathologies such as breast cancer are associated with higher rates approaching 40% late in the course of the disease.4 Of the cases, 20–40% are bilateral, and multifocal involvement of one eye occurs in approximately 20% of affected cases.5 Frequency of metastases does not differ for the right or the left eye.5
Symptoms and clinical findings
Intraocular metastases may be asymptomatic. When symptomatic, choroidal metastases cause painless visual loss by involvement of the macular area or peripapillary retina or because of an associated, generally exudative, retinal detachment.6,7 Retinal detachment may cause visual deficits, floaters and flashes. Larger retinal detachments may be associated with peripheral field deficits. Tumors located anteriorly may tilt the lens, thereby causing visual loss. Rarely, these patients may have painful visual loss as a result of neovascular glaucoma or metastatic iritis.
In a review of 70 patients with choroidal metastases, symptoms at presentation included: blurred vision in 80%; pain in 14%; photopsias in 13%; red eye and floaters in 7%; field defects in 3%, and photophobia in 1%. A total of 6% of patients were asymptomatic.8
The most common location for choroidal metastases is the posterior pole of the globe. Up to 40% of lesions have been reported to be in the macular region.9 The reason for this may be due to differential blood flow to that area, although macular metastases are also more likely to be symptomatic, therefore increasing the likelihood of diagnosis.
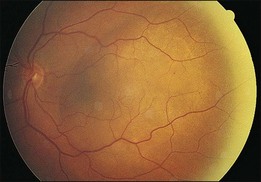
In contrast to choroidal melanomas which are generally darkly pigmented, choroidal metastases more commonly present as yellow or white lesions (Fig. 151.1). For lesions of a comparable basal size, choroidal metastases are often flatter than choroidal melanomas. Serous retinal detachment is commonly associated and frequently not in proportion with the tumor size.8,10
Frequency of primary cancer site
The relative frequency of primary cancer site for patients with choroidal metastases varies by gender. A series of more than 500 patients from the Wills Eye Hospital11 revealed primary sites for women as follows: breast, 68%; lung, 12%; unknown, 12%; gastrointestinal, 2%; skin, 1%; renal, <1%; and other, 4%. For men, primary sites were: lung, 40%; unknown, 29%; gastrointestinal, 9%; prostate, 6%; renal, 6%; skin, 4%; breast, 1%; and other, 4%.
Diagnostic evaluation
Differential diagnosis
Metastatic tumors usually have a creamy yellow appearance; purely amelanotic lesions are more likely to represent amelanotic choroidal melanomas. Metastatic lesions are usually flatter and rarely show the mushroom-shaped configuration that is often seen with melanomas. Choroidal metastases are also generally located in the posterior pole. Metastatic lesions anterior to the equator and metastases that involve the ciliary body are uncommon, and therefore amelanotic choroidal melanoma is more likely to be diagnosed in those locations. Bilateral or multifocal lesions are more likely to be metastatic, infectious, or uveitic. Combined A- and B-scan ultrasonography is of value in differentiating metastases from primary choroidal melanomas. Choroidal melanomas usually have low to moderate internal reflectivity, whereas metastatic lesions usually have higher internal reflectivity.12,13 More recently, optical coherence tomography has become useful to assist with the differential diagnosis of choroidal tumors.14
Choroidal osteomas may be bilateral and may have a color similar to that of metastatic tumors. Osteomas are rarely significantly elevated, and associated choroidal neovascularization is more common in patients with choroidal osteomas than in those with metastases. Ultrasound examinations15 and computed tomography (CT) scans are extremely valuable diagnostic tools in these patients because the bony change in the choroid shows very high reflectivity on ultrasound examination, and bone density can be confirmed with the CT scan.16 Optical coherence tomography may show overlying photoreceptor changes.17
Circumscribed choroidal hemangiomas are almost always unilateral and unifocal. Their characteristic reddish orange coloration is an important diagnostic clue. Fluorescein angiography shows more prominent early choroidal filling than is usually seen with metastatic lesions.16 Optical coherence tomography features of hemangioma have also been reported.18
Although some inflammation may be associated with a choroidal metastasis, inflammation is generally not prominent, but it can be seen, sometimes associated with choroidal detachment.19 A number of inflammatory conditions should be distinguishable, including Harada disease, the uveal effusion syndrome, posterior scleritis, and similar entities.16 In these patients, associated vitreous inflammation is often seen, and diffuse thickening of the choroid usually can be demonstrated on ultrasound examination.
Rarely do patients with large disciform scars or subretinal hemorrhages present a confusing picture. There is usually a history of previous visual loss related to choroidal neovascularization, and a history of systemic cancer is much less common. Drusen are usually apparent in the fellow eye. The echograms may be difficult to interpret, and the eyes are occasionally enucleated owing to a mistaken diagnosis of choroidal melanoma.20 The whitish yellow color of choroidal metastases is usually quite different from the darker appearance of these lesions, in which admixed blood is a prominent feature.
Ophthalmic evaluation and ancillary tests
Anticipating that radiation therapy may be recommended and may be cataractogenic, the status of the lens should be carefully evaluated.21 If the patient is diabetic or has retinal microangiopathy, this should be noted because radiation therapy exacerbates pre-existing retinal vascular disease (see Chapter 58, Radiation retinopathy). Documentary fundus photographs should be obtained to compare with later examinations to assess growth or treatment response.
Fluorescein angiography
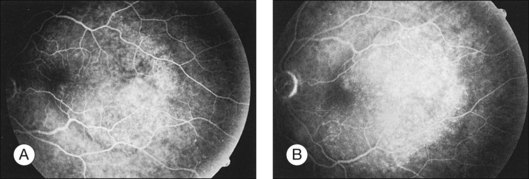
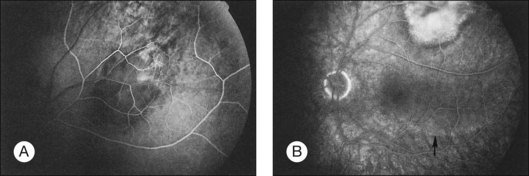
Metastatic choroidal tumors are usually hypofluorescent in the early phases of the study and become progressively hyperfluorescent in late phases (Figs 151.2, 151.3). The so-called double circulation pattern, thought to be characteristic of choroidal melanomas that have broken through Bruch’s membrane, is a rare finding in metastatic tumors.22 Prominent early choroidal filling is a feature more typical of circumscribed choroidal hemangiomas.16
A- and B-scan ultrasonography
B-scan ultrasonography is of value in evaluating patients with media opacities or bullous retinal detachments when a choroidal lesion is suspected but cannot be clearly seen. The B-scan ultrasonogram shows an echogenic subretinal mass with diffuse, ill-defined borders. Overlying retinal detachment is common, and sound attenuation in the lesion is usually moderate.13 In unusual cases, choroidal detachment may be seen.19
The A-scan ultrasonogram usually demonstrates moderate to high internal reflectivity. Vascularity is not prominent, and the consistency is solid.12,13 It is useful to determine the height of the metastatic tumor by ultrasonography, so that shrinkage of the lesion can be documented after treatment. A more complete discussion of the ultrasonographic features of choroidal metastases is provided in Chapter 9 (Diagnostic ophthalmic ultrasound), as well as in standard texts.15 Magnetic resonance imaging and spectroscopy may also prove to be valuable differential diagnostic aids.23,24
Optical coherence tomography
Optical coherence tomography (OCT) imaging, particularly with enhanced depth imaging (EDI) of the choroid as popularized by Spaide and others may help with the differential diagnosis. Torres and colleagues have recently summarized the EDI features of various choroidal tumors.25
Fine-needle aspiration biopsy
Diagnostic fine-needle aspiration biopsy (FNAB) of intraocular tumors should be considered only under special circumstances.26 The technique may be appropriate in a patient who has what appears to be a characteristic metastatic tumor but in whom a primary lesion cannot be found despite an extensive systemic evaluation. Augsburger and Shields26 include, as an additional indication, the use of the technique in some patients who refuse treatment without histopathologic verification of the lesion (rare) or in patients who have lesions that present major diagnostic uncertainty.
In general, oncologists require a histologic diagnosis before initiation of treatment of nonocular sites. Because of the potential threat to vision, it is not a routine procedure to biopsy intraocular lesions before treatment. Useful reports provide updates on FNAB and choroidal tumors.27–29
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


