Fig. 971 Primary total obliteration of the cavity after classic intact canal wall mastoidectomy using autogenous cartilage and a Palva flap. After a canal wall–up mastoidectomy with a completely intact ear canal wall, plates of tragal cartilage are placed on the medial attic wall behind the intact ear canal wall to form a close and tight connection with the tympanic cavity. Behind these plates, other pieces of available cartilage tightly obliterate the attic, antrum, and the medial part of the cavity. The lateral part of the cavity will be filled with a muscle flap
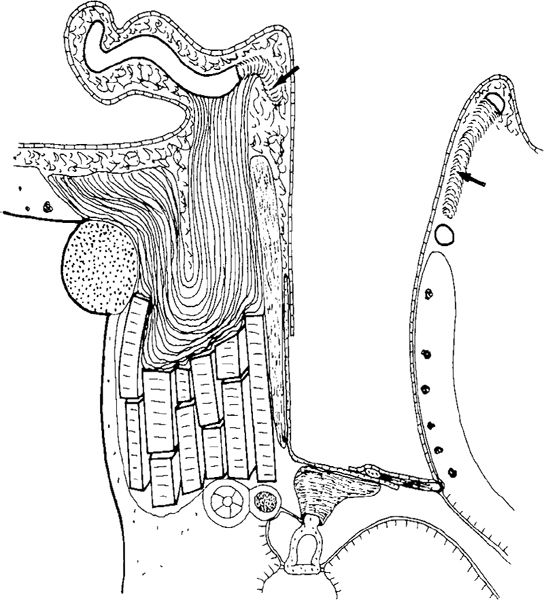
Fig. 972 Side view of the obliteration with autogenous tragal and conchal cartilage and Palva flap behind an intact bony ear canal wall. The cartilage obliterates the medial part of the cavity; the lateral part is obliterated with a Palva flap. A piece of cortex is shaped and placed between the stapes and malleus handle. The posterior perforation is closed with an underlay fascia graft, continuing over the bony ear canal wall. The resected parts of the cartilage are indicated by arrows
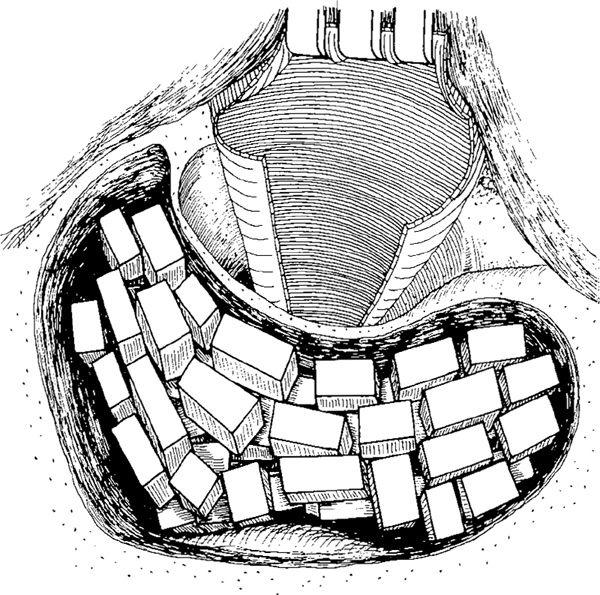
Fig. 973 Obliteration, using allogenous costal cartilage (Meuser), of the mastoid cavity behind an intact canal wall. Many small rectangular pieces of costal cartilage are placed in the cavity to completely fill it
Autogenous cartilage has also been used for reconstruction of the ear canal wall in many other situations:
A. Scutumplasty in classic intact canal wall mastoidectomy (Figs. 349–359) (McCleve 1969, 1985, Fleury 1974, Adkins and Osguthorpe 1984, Hildmann 1991, Kinney 1982, Honda 1992, Sheehy 1990, Portmann 1979, Choissone 1985, Linde 1973, Eviatar 1978).
B. Reconstruction of atticotomies in the modified intact canal wall technique (Chapter 7), either with an intact bridge (Fig. 440), a defective bridge, or a displaced and missing bridge (Fig. 478).
C. Ear canal wall reconstruction in Wigand’s technique (Chapter 9), with cartilage covering the atticotomy and antrotomy openings (Figs. 546, 548 to 551).
D. Closure of the aditus ad antrum in “antrum exclusion, attic elimination on demand techniques” (Olaizola 1988) (Fig. 563, 565, 567).
E. Reconstruction of the entire ear canal wall with autogenous cartilage in order to ventilate the cavity (Chapter 17, Figs. 824–831).
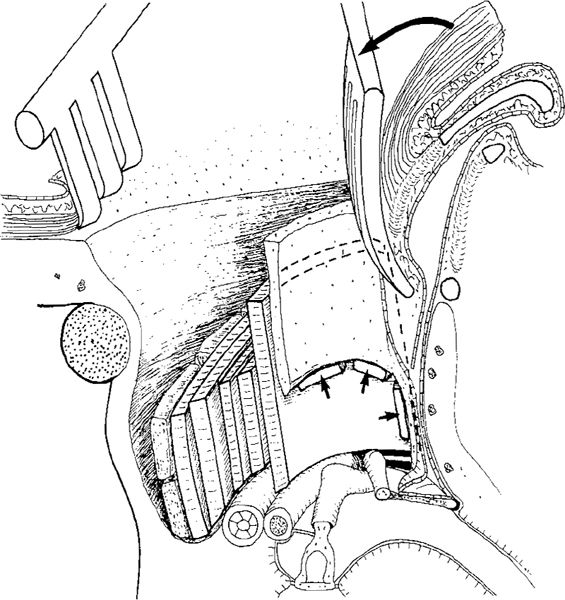
Fig. 974 Side view, with some perspective, of combined-graft obliteration of a cavity after modified intact canal wall mastoidectomy with a large defect in the bony ear canal wall. A large plate of cartilage is placed on the medial wall of the attic, behind the bony ear canal wall. Several small pieces of cartilage support the tragal cartilage and obliterate the attic and aditus. Pieces of bone or bone chips are placed behind the cartilage, and the lateral part is obliterated with a Palva flap, which is ready to be placed in the cavity after removal of the selfretaining retractor (large arrow). At the border between the ear canal and the cartilage, additional small pieces of cartilage are placed to tighten the fissures between the bone and cartilage (small arrows)
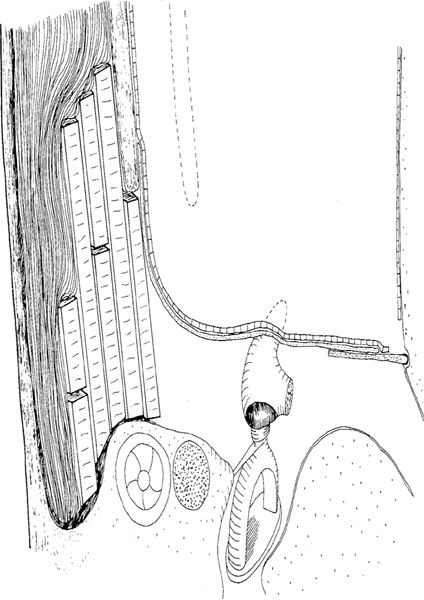
Fig. 975 Obliteration of the posterior part of the cavity behind a displaced bony ear canal wall, following Farrior’s technique. The original position of the ear canal wall is indicated with cashed lines. The attic is ventilated, and is covered with a large fascia. Behind the preserved and displaced bony ear canal wall, the cavity is obliterated with pieces of autogenous cartilage and muscle
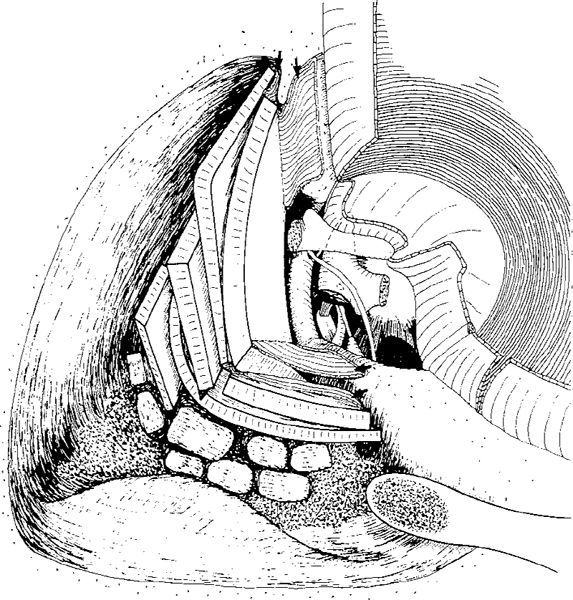
Fig. 976 Combined-graft obliteration (Tos) in a canal wall–down mastoidectomy cavity with reconstruction of the ear canal wall with tragal cartilage. A large piece of tragal cartilage is placed on the medial wall of the attic as a compound graft. The attached perichondrium is piaced on the zygomatic root and facial ridge (arrows) to secure the position of the cartilage and tighten the new ear canal wall. Further pieces of tragal or conchal cartilage are placed behind the tragal cartilage. The deepest part of the cavity is covered with pieces of bone, bone chips, and bone paté. The lateral part of the cavity will be filled with muscle
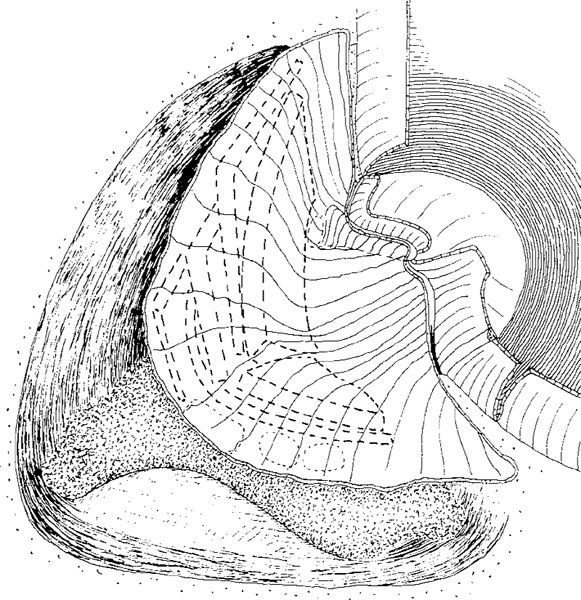
Fig. 977 The fascia covers the posterior perforation as an underlay graft, as well as the entire reconstructed ear canal wall. Bone paté is visible in the sinodural angle and the mastoid tip
Obliteration in Canal Wall–Down Mastoidectomy
As mentioned above, autogenous tragal and conchal cartilage do not totally obliterate a large cavity. They form either 1) part of a combined-graft total obliteration in large cavities; 2) obliterate only part of the cavity, in combination with an adequate meatoplasty (Heermann 1992); or 3) obliterate parts of the cavity, which basically remains an open one.
Autogenous Cartilage in Combined-Graft Obliteration
As in obliteration with combined grafts in canal wall–up techniques (Figs. 971–975), the plates of autogenous cartilage are used for the most medial part of the ear canal wall reconstruction, simply because the tragal cartilage fits into the attic well and provides a smooth and firm medial boundary to the new ear canal wall.
The author has performed reconstruction of the ear canal using autogenous tragal cartilage in combined-graft obliteration (Tos 1977, Siim and Tos 1987, 1989). After a canal wall–down mastoidectomy with preservation of as many ear canal skin flaps as possible, ossiculoplasty is performed (Fig. 976). A large piece of tragal cartilage with attached perichondrium is placed on the medial wall of the attic at the border between the facial nerve eminence and the lateral semicircular canal. The tragal cartilage forms the posterosuperior ear canal wall, and adjacent conchal and tragal cartilage fixes it to the anterior cavity wall. All remaining tragal and conchal cartilage is placed in smaller pieces behind the large tragal cartilage graft, thus obliterating the attic and closing all the fissures between the cartilage and the cavity walls. Behind the autogenous cartilage, bone paté is placed in the deepest part of the cavity, e. g., into the sinodural angle or into the mastoid tip, or both, and pieces of autogenous cortical bone and bone chips are then placed behind the cartilage (Fig. 976). Once the cavity has been partly obliterated, the remaining reconstruction of the ear canal and the myringoplasty are completed by placing a large, specially tailored piece of “semidry” temporalis muscle fascia as an underlay graft, closing the ear drum perforation, and covering the interposed ossicle and the entire meatal surface of the tragal cartilage. Superiorly, the fascia is placed on the zygomatic root, and inferiorly onto the facial ridge (Fig. 977). The medial ear canal skin flaps are replaced and fixed using Gelfoam balls (Fig. 978) or small pieces of gauze, or both.
The obliteration of the lateral part of the cavity (Fig. 978) is performed using a superiorly-based bipartite subcutis–muscle flap (Tos 1969) (Figs. 881–890). In reconstruction of the lateral part of the cavity, a small Palva flap is also used (Figs. 821, 831, 974). The bipartite temporalis muscle can be placed in the lateral part of the cavity without loosening the selfretaining retractor (Fig. 978). The small Palva flap is used at the very end of the operation, after widening of the ear canal with an intercartilaginous incision at the 12-o’clock position, and extending 1–2 cm vertically, anterior to the helix (Fig. 979).
The small Palva flap ensures a tight connection between the epithelial flap (the Kroner flap) and the fascia, which is often shorter than desired.
Another type of obliteration uses a large Palva subcutis–muscle flap (Fig. 980). The Palva flap is brought deep into the cavity. In obliteration with a Palva flap, the following sequence is important: 1) Reconstruction of the ear canal wall with cartilage and fascia, as well as obliteration of the medial part of the cavity (Fig. 977). 2) Placing a strip of gauze in the cavity in order to prevent accumulation of blood within it during preparation of the Palva flap and during meatoplasty. 3) Removal of the gauze just prior to placement of the Palva flap, which completes the obliteration and canal wall reconstruction (Fig. 980).
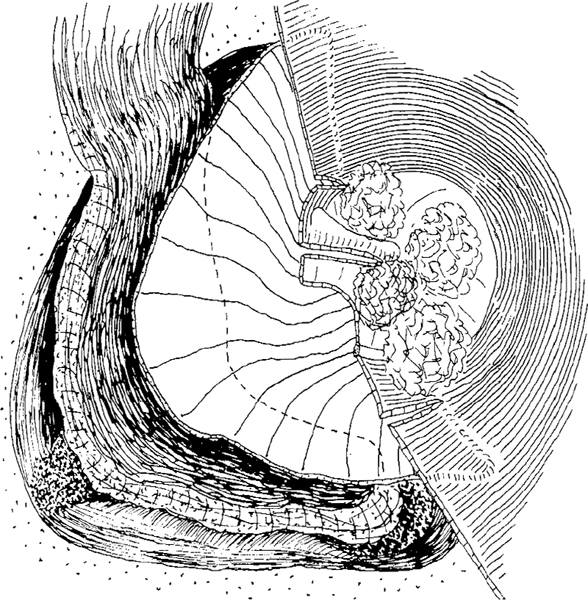
Fig. 978 The replaced ear canal skin flaps are fixed with Gelfoam balls. The lateral part of the cavity is filled with a superiorly-based bipartite subcutis–muscle flap (Figs. 881–890)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


