CHAPTER 87 Benign Neoplasms of the Salivary Glands
Better understanding of the histogenesis of neoplasms of the salivary glands, however, has allowed a more consistent and rational classification of these tumors. Recent advances in molecular biology and tumor genomics have shed some light on the genetic basis of certain types of tumors of the salivary glands.1 The role of fine-needle aspiration biopsy and high-resolution imaging in the management of patients with salivary neoplasms continues to evolve. This chapter discusses some of the advances made in understanding the etiology and histogenesis of salivary tumors and describes a contemporary approach to the diagnosis and management of patients with benign neoplasms of the salivary glands.
Embryology
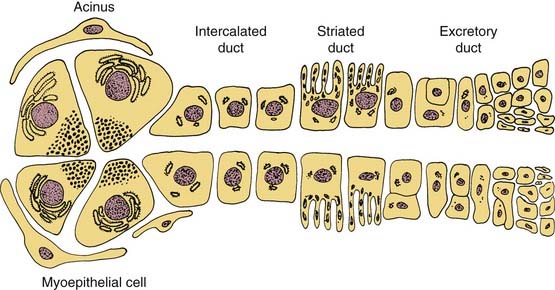
Understanding the origin of benign salivary gland tumors requires knowledge of the embryology and ultrastructure of the normal salivary gland. The major salivary glands originate from ectoderm and begin their development during the sixth week of gestation as solid, ridgelike ingrowths of the oral epithelium.2 These ingrowths continue to develop into tubules that later become the ductal system of the salivary glands. In the major salivary glands both serous and mucous cells are arranged into acini that are drained by a series of ducts. An intercalated duct drains into a striated duct, which empties into an excretory duct. Contractile myoepithelial cells surround the acini and intercalated ducts and help in draining saliva through the ductal system (Fig. 87-1). The parotid gland consists of predominately serous acini. The submandibular gland is composed of a mixture of serous and mucinous acini, whereas sublingual gland and minor salivary glands scattered throughout the upper aerodigestive tract contain predominantly mucinous acini.
Histogenesis of Salivary Neoplasms
At least two theories of tumorigenesis have been proposed for salivary gland neoplasms.3 In the multicellular theory, each type of neoplasm is thought to originate from a distinctive cell type within the salivary gland unit. According to this theory, Warthin’s and oncocytic tumors are thought to arise from striated ductal cells, acinic cell tumors from acinar cells, and mixed tumors from intercalated duct and myoepithelial cells.4 This theory is supported by the observation that all differentiated salivary cell types retain the ability to undergo mitosis and regenerate.5,6 An alternative theory, the bicellular reserve cell theory, assumes that the origin of the various types of salivary neoplasms can be traced to the basal cells of either the excretory or the intercalated duct. According to this theory, either of these two cells can act as a reserve cell with the potential for differentiation into a variety of epithelial cells.7 Hence despite the seeming heterogeneity of salivary tumors, all of them are thought to arise from one of two pluripotential cell populations. In this model, adenomatoid tumors including pleomorphic adenoma and oncocytic tumors are derived from the reserve cell of the intercalated duct, whereas epidermoid tumors, such as squamous cell carcinoma and mucoepidermoid carcinomas, are derived from the reserve cell of the excretory duct.8 Some reports provide molecular evidence to support the reserve cell theory of salivary gland tumorigenesis.9
Recent efforts to identify biomarkers of salivary neoplasia have focused on methylation patterns. Williams and colleagues10 investigated methylations status and protein expression of four tumor suppressor genes (DAPK, MGMT, RARB2, and RASSF1) in the largest cohort study of benign and malignant salivary neoplasms to date. The authors found benign and malignant salivary tumor differed in the frequency and pattern of gene methylation. They postulate methylation may aid in diagnosis and targeted therapy for salivary neoplasms.10 Maruya and colleagues analyzed the gene expression profile of 18 primary tumors representing the major benign subtypes using a membrane-based DNA microarray platform. Of the 5000 genes arrayed, S-100 beta, galectin-9 isoform, vimentin, and tyrosine kinase receptor were more highly expressed in adenomas than in carcinomas.11
Etiology
Radiation
There is increasing evidence to suggest that exposure to ionizing radiation may increase the risk of developing tumors of the salivary glands. In 1996 the Radiation Epidemiology Branch of the National Cancer Institute published a study on the risk of developing salivary gland tumors among atomic bomb survivors.12 The study indicated a higher radiation-related risk of developing both benign and malignant salivary gland tumors, as compared with the general population. Dose-response analyses found statistically significant increases in risk with increasing A-bomb dose for both cancer and benign tumors. The risk was higher for malignant tumors, especially mucoepidermoid carcinoma. Among those with benign neoplasms, Warthin’s tumor showed the highest dose-response–related risk.
Radiation therapy to the head and neck, especially if it encompassed the salivary glands, may also be a risk factor in the development of salivary gland tumors.13 A recent study found a 4.5-fold increase in the incidence of salivary gland cancer and a 2.6-fold increase of benign tumors among persons exposed to scalp irradiation compared with matched controls.14 The mean length of latency period until tumor development was 11 years for malignant tumors and 21.5 years for benign. The study also demonstrated a clear dose response effect for cancer and benign tumors, suggesting that ionizing radiation may play an important role in salivary gland tumorigenesis.
Viral
Although Epstein-Barr virus (EBV) has been consistently associated with lymphoepithelial carcinoma of the salivary gland in the Asian population, there is no evidence of a causal role of EBV in other primary salivary gland neoplasms.15 Pollock and colleagues16 failed to demonstrate any positive signal by in situ hybridization for EBV RNA in 42 benign salivary gland neoplasms. Other viruses including human papillomavirus, human herpesvirus-8, and cytomegalovirus do not appear to have any etiologic role in salivary gland neoplasms.17
Other Factors
Although tobacco use was not associated with a higher incidence of malignant salivary neoplasms, Warthin’s tumor is strongly associated with cigarette smoking.18 Occupational exposure to silica dust was linked to a 2.5-fold increased risk of cancer of the salivary gland.19 The risk was also elevated among rubber workers exposed to nitrosamines.20 Dietary analyses revealed a possible protective effect for a diet high in polyunsaturated fatty acids.19,21 Similar to breast cancer, women with history of early menarche and nulliparity had an increased risk of cancer of the salivary gland, which may be due to a hormonal effect.22 Whether these occupational, dietary, or hormonal factors have any association with the risk of developing benign tumors of the salivary glands remains unknown.
Genetic Factors
Recent developments in the field of molecular biology and human genomics have shed light on the genetic basis of developing several types of neoplasms including tumors of salivary gland origin. A study of several types of salivary gland tumors using comparative genomic hybridization found specific genetic alterations in different types of salivary gland tumors and involvement of several chromosomes in the alterations.23 Genetic aberrations associated with the salivary gland neoplasia include allelic loss and point mutation, structural rearrangement of chromosomal units (most commonly translocations), the absence of one chromosome (monosomy), and the presence of an extra chromosome (polysomy). Any of these genetic aberrations may be the only karyotypic anomaly indicating an early event in tumor initiation, or several genetic alterations may coexist, which are more likely to be associated with tumor progression and more aggressive biologic behavior.9,24
Incidence
Salivary gland tumors are relatively rare and constitute 3% to 4% of all head and neck neoplasms. The majority (70%) of salivary gland tumors arise in the parotid gland (Fig. 87-2). Although the majority of minor salivary gland tumors are malignant, three fourths of parotid tumors are benign (Fig. 87-3). Spiro25 reviewed the Memorial Sloan-Kettering experience with salivary neoplasms over a 35-year period. The distribution of these 2807 patients is shown in Table 87-1. Benign neoplasms constituted 54% (1529 patients) of all tumors. Pleomorphic adenoma (1280 patients) constituted 84% of benign tumors and 45% of all salivary gland neoplasms. Warthin’s tumor was the second most benign tumor and comprised 12% (183 patients) of all benign tumors.
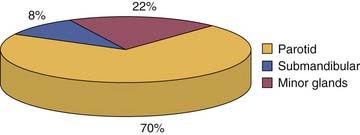
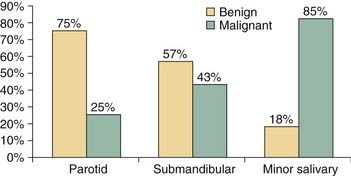
Figure 87-3. The incidence of benign and malignant salivary neoplasms according to the site of origin.
Table 87-1 Distribution of 2807 Salivary Neoplasms
| Histology | Number of Patients | Percent |
|---|---|---|
| Pleomorphic adenoma | 1274 | 45.4 |
| Warthin’s tumor | 183 | 6.5 |
| Benign cyst | 29 | 1.0 |
| Lymphoepithelial lesion | 17 | 0.6 |
| Oncocytoma | 20 | 0.7 |
| Monomorphic adenoma | 6 | 0.2 |
| Mucoepidermoid carcinoma | 439 | 15.7 |
| Adenoid cystic carcinoma | 281 | 10.0 |
| Adenocarcinoma | 225 | 8.0 |
| Malignant mixed tumor | 161 | 5.7 |
| Acinic cell carcinoma | 84 | 3.0 |
| Epidermoid carcinoma | 53 | 1.9 |
| Other (anaplastic) | 35 | 1.3 |
| Total | 2807 | 100 |
From Spiro RH. Salivary neoplasms: overview of a 35-year experience with 2,807 patients. Head Neck Surg. 1986;8:177-84. © 1986 John Wiley & Sons.
Patient Evaluation
Clinical Features
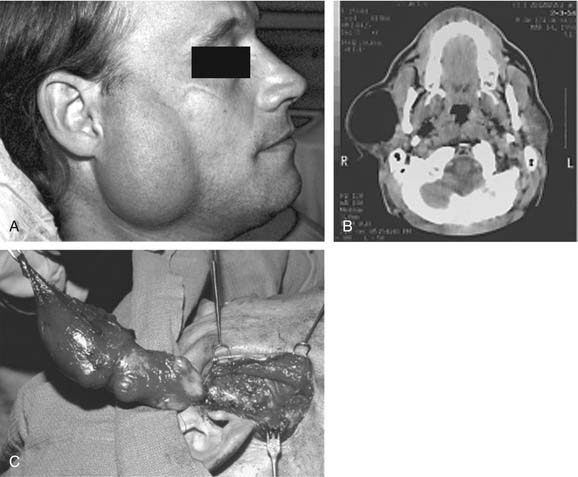
On examination, benign tumors of the parotid gland are usually well defined, nontender, and freely mobile. They are commonly located in the “tail” of the parotid gland but may be present anywhere in the superficial or deep lobe. Tumors may originate entirely from the deep lobe (Fig. 87-4) or extend from the superficial to the deep lobe through the relatively narrow stylomandibular tunnel, giving the appearance of a dumbbell tumor (Fig. 87-5). In either case, the tumor may extend to the parapharyngeal space and displace the oropharyngeal wall medially (Fig. 87-6). The presence of facial nerve paresis or paralysis, pain, fixation of the mass to the overlying skin or underlying structures, and associated cervical adenopathy usually indicate the presence of malignancy. It should be noted, however, that these findings usually indicate local or regional extension of the tumor, and the diagnosis of parotid malignancy should not await the development of these signs and symptoms. The possibility of malignancy should be ruled out in patients presenting with any mass in the parotid gland. This will usually require cytologic or histologic evaluation with a fine-needle biopsy, or parotidectomy, respectively.
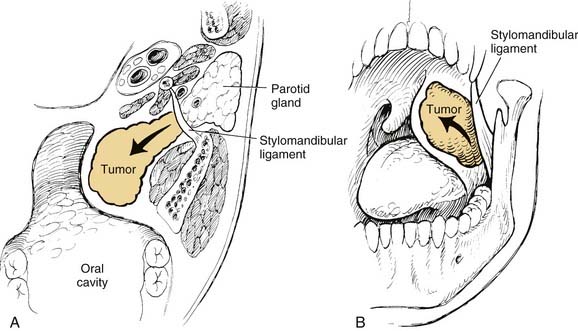
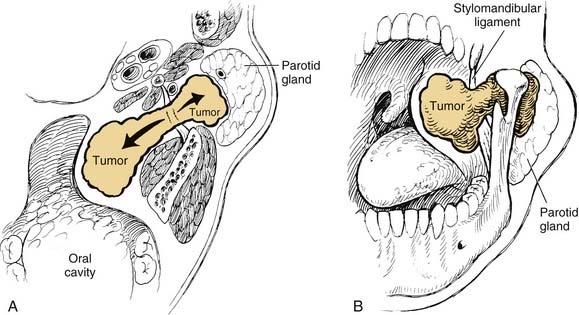

Figure 87-6. Pleomorphic adenoma of the deep lobe of a parotid gland, causing medial displacement of the palate and tonsil.
Benign tumors of the minor salivary glands are rare. Most tumors arising from the minor salivary glands are malignant (see Fig. 87-3). However, similar to the major salivary glands, pleomorphic adenoma is the most frequent benign tumor of the minor salivary glands. The clinical presentation depends on the site of origin, and the most common sites include the palate, parapharyngeal space, and the lacrimal gland.
Fine-Needle Aspiration Biopsy
Fine-needle aspiration biopsy (FNAB) has been widely recognized and well established as an accurate technique in the diagnosis of salivary gland neoplasms. Numerous studies have reported an exceptionally high degree of sensitivity, specificity, and predictive value for FNAB. The overall sensitivity ranges from 85.5% to 99%, and the overall specificity ranges from 96.3% to 100%.26–28 In general, diagnostic accuracy is higher for benign than for malignant salivary gland tumors.29,30 The accuracy of FNAB, however, depends greatly on the experience of the cytopathologist, as well as the overall volume of patients with salivary neoplasms evaluated in any given institution. The most common source of diagnostic error of FNAB is inadequate sampling.31 The use of ultrasound-guided FNAB may be of help in cases in which it is difficult to obtain a representative sample, and it enhances the overall diagnostic accuracy of the technique.32,33 Despite its overall high accuracy, several significant but uncommon areas can lead to diagnostic difficulties, with the potential for clinically important diagnostic errors.29 The most frequent problems involve variations in the expected cytology of pleomorphic adenoma. Also, there are several benign-malignant “look-alike” pairs of lesions. The first of these is related to small-cell epithelial neoplasms of low nuclear grade; the most frequent problem is between basal cell adenomas and adenoid cystic carcinoma, particularly the solid (anaplastic) type. The next area contrasts mucoepidermoid carcinoma with its cytologic mimic, benign salivary gland duct obstruction. The final difficulty in salivary gland aspiration contrasts large-cell epithelial lesions of low nuclear grade: oncocytic proliferations and acinic cell carcinoma.34
In addition to being accurate, FNAB is safe, simple to perform, and relatively inexpensive. However, one essential question is worth asking. Is FNAB really necessary in the evaluation of salivary gland masses? Would it change the course of management on the basis of clinical assessment? In an attempt to answer this question, Heller and colleagues35 performed a study to determine the impact of FNAB on patient management. One hundred patients underwent FNAB of major salivary gland masses. The physician’s initial clinical impression was compared with the FNAB diagnosis and the final diagnosis in each case. Overall, FNAB resulted in a change in the clinical approach to 35% of the patients. Examples of such changes in the planned management included avoiding surgical resection for lymphomas and inflammatory masses and adopting a more conservative approach with benign tumors in elderly and high-surgical-risk patients. FNAB also allows better preoperative counseling of patients regarding the nature of the tumor, the likely extent of resection, management of the facial nerve, and the likelihood of a neck dissection. Such information is not only important in treatment planning but also helps alleviate an already high level of anxiety among patients and their families.
The possibility of tumor seeding is a commonly cited argument against the routine use of FNAB in patients with salivary gland tumors. To address these issues, Mukunyadzi and colleagues36 recently reviewed 94 resected salivary gland masses for infarction, hemorrhage, and needle track tumor seeding, as well as fibrosis after FNAB. They concluded FNAB with a 25-gauge needle is safe and does not significantly alter the histologic diagnosis because tissue effects did not preclude accurate diagnostic interpretation in any case.36
Imaging
The routine use of imaging in patients with small, well-defined masses of the superficial lobe of the parotid gland is probably not warranted because the results of imaging are not likely to change the treatment plan. However, tumors that present with clinical findings suggestive of malignancy, tumors arising from the deep lobe of the parotid gland or the parapharyngeal space, and, tumors of the submandibular and minor salivary gland should be evaluated with high-resolution imaging. In such cases, imaging provides accurate delineation of the location and extent of tumor, its relation to major neurovascular structures, perineural spread, skull base invasion, and intracranial extension.37
Computed Tomography and Magnetic Resonance Imaging
In evaluating patients with tumors of the salivary glands, both computed tomography (CT) and magnetic resonance imaging (MRI) provide information that is superior to that provided by other imaging techniques or by physical examination.38 The normal parotid gland has a high fat content and is easily visualized on both CT and MRI. Therefore both techniques can demonstrate whether a mass in that region is intraglandular or extraglandular. Generally, neither CT nor MRI provides information regarding the specific histologic diagnosis, except rarely.39 An example of such a rare scenario is with lipoma of the parotid gland (Fig. 87-7). The MRI signal characteristics of parotid masses, however, may be suggestive of certain diagnosis.40 For example, if a parotid gland mass is bilateral, it is more likely to be Warthin’s tumor, especially if it does not enhance. Less likely, it could be lymphoepithelial cyst or necrotic lymph node. A unilateral, nonenhancing mass with a high T2 signal is more likely to be a Warthin’s tumor and less likely a necrotic lymph node or first branchial cleft cyst. If the mass is unilateral, shows postcontrast enhancement, has a high T2 signal, and does not invade surrounding tissue planes, it is more likely to be a pleomorphic adenoma (Fig. 87-8). An intermediate to low T2 signal mass, with or without invasion of surrounding tissue planes, is more likely to be a malignant mass such as adenoid cystic or mucoepidermoid carcinoma.41
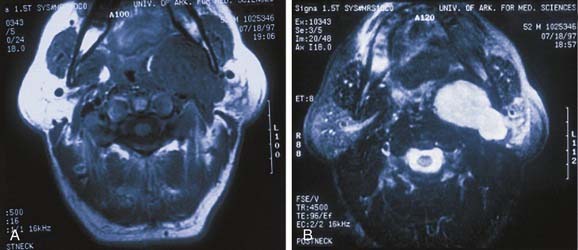
MRI is also superior to CT in demonstrating the internal architecture of salivary gland tumors in a multiplanar fashion and in delineating the interface between tumor and normal salivary gland.42 In contrast to benign tumors, which invariably have well-defined margins (see Fig. 87-8), malignant tumors may exhibit irregular margins (Fig. 87-9). Extension of the tumor beyond the fascial confines of the gland can be adequately seen on both CT and MRI and should raise the suspicion of malignancy.43 Bone destruction of the mandible or skull base is best visualized on CT, whereas bone marrow involvement is better demonstrated on MRI. Both studies can adequately evaluate the neck for metastatic adenopathy. CT has the advantage of being less expensive and more available than MRI.
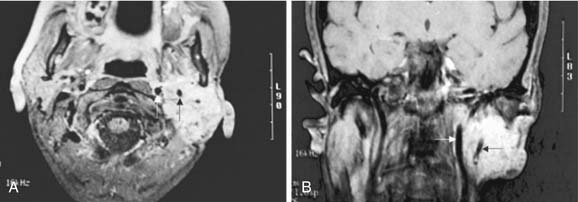
Although parapharyngeal space masses are well visualized by both techniques, they are better delineated with MRI than CT. This is because of the different signal intensity of tumor, fat, and muscle on MRI. The differential diagnosis of parapharyngeal masses includes deep lobe parotid tumors, minor salivary gland tumors, and neurogenic and vascular tumors. Most salivary tumors have low-to-intermediate T1 signal intensities and intermediate-to-high T2 signal intensities. Deep lobe parotid tumors and minor salivary gland tumors of the parapharyngeal space lie in the prestyloid compartment, anterior to the carotid artery, and displace the parapharyngeal fat medially (Figs. 87-10 and 87-11). Deep lobe tumors are connected to the parotid gland at least in one imaging section, whereas minor salivary gland tumors are completely surrounded by fat (see Fig. 87-11). By contrast, neurogenic tumors and glomus tumors lie in the poststyloid compartment, posterior to the carotid artery, which is displaced anteriorly (Fig. 87-12). Neurogenic tumors usually enhance intensely with gadolinium, whereas glomus tumors have characteristic serpiginous flow voids (salt and pepper appearance) on MRI.
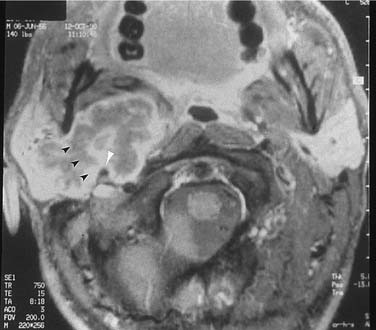

Figure 87-11. In contrast to the dumbbell tumor depicted in Figure 87-10, this pleomorphic adenoma originates entirely from the deep lobe of the parotid gland (black arrow) and lies entirely medial to the stylomandibular tunnel. Pleomorphic adenomas originating from the minor salivary glands of the parapharyngeal space have a similar appearance on high-resolution imaging but are not connected to the parotid gland. Regardless of their origin, salivary gland tumors of the parapharyngeal space will occupy the prestyloid compartment and displace the carotid artery posteriorly (white arrow).

Recently, new MR technologies such as dynamic contrast-enhanced MRI, diffusion-weighted MRI, and proton MR spectroscopy have shown promising results in the differentiation between benign and malignant salivary gland tumors.44 Further research with larger-scale studies on these particular MR methods is necessary.
Ultrasonography
Ultrasonography has the advantage of being inexpensive, noninvasive, simple to perform, and is virtually free of complications. It can be used to differentiate solid from cystic masses in the salivary glands, and most salivary gland diseases can be diagnosed sonographically.32
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


