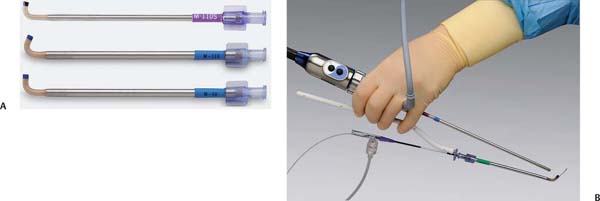
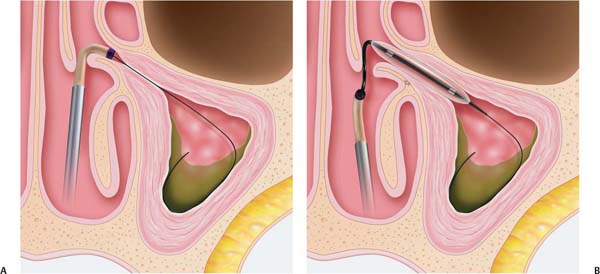
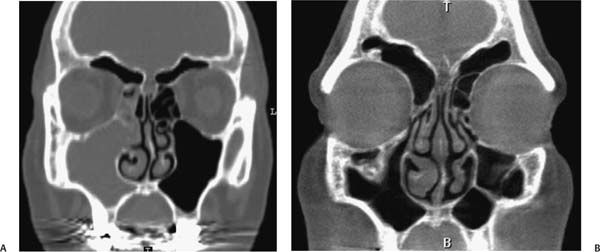
14 Balloon Sinuplasty for the Maxillary Sinus Chronic rhinosinusitis affects 31 million adults in the United States each year, resulting in direct annual health care costs reaching $5.8 billion, with indirect costs higher due to lost productivity.1,2 Current treatment options include medical therapy and management of allergies, with surgery reserved for those who fail medical treatment. Candidates for surgery are determined based on clinical and endoscopic exam findings, symptoms, and evidence of obstruction of the sinus on computed tomography (CT) scans. Although an estimated 500,000 sinus procedures are performed annually,3 many other patients decline surgery due to risks and morbidity involved, or are deemed to be poor surgical candidates owing to comorbid conditions. The goal of modern endoscopic surgery is to open the ostium of the sinus and to restore normal mucociliary clearance. When considering the maxillary sinus, this commonly involves removal of the uncinate process and creation of an antrostomy, which includes the natural ostium of the sinus. Of course, tissue removal introduces bleeding and potential for scarring, as well as recirculation phenomenon if the maxillary ostium is not included in the antrostomy. Recently, new techniques have been introduced that may have less morbidity than traditional dissection methods. This technology uses dilatational balloon catheter systems similar to those used in the fields of interventional cardiology, gastroenterology, vascular and urologic surgery. Two sets of Food and Drug Administration- (FDA-) approved devices utilize balloon catheter technology to access the natural ostium of the maxillary sinus and dilate it without removal of tissue. This may result in a functional ostium without some of the morbidities encountered with traditional dissection. Balloon catheter technology may be used alone or in combination with standard dissection, as a hybrid technique. We describe the technique for maxillary sinuplasty with the Relieva sinus balloon catheter (Acclarent, Menlo Park, CA) and briefly review the FinESS sinus treatment (Entellus Medical, Maple Grove, MN). Sinus balloon dilation is indicated for many of the similar indications for FESS.4 We currently consider these devices in patients meeting the following criteria: • History of chronic or recurrent sinusitis and Balloon dilation may be contraindicated in patients with: • Sinonasal polyps involving the maxillary sinus or the middle meatus • Allergic fungal sinusitis • Sinonasal tumors • Extensive osteoneogenesis • Previous history of facial trauma involving the maxillary sinus • Mucopyocele Standard sinus surgery instrumentation including angled endoscopes (we routinely use 30 and 70 degree) are recommended to survey the lateral nasal wall during and after the procedure, to ensure cannulation and dilatation of the maxillary sinus ostium. In addition to standard instruments, maxillary sinuplasty requires guide catheters, flexible guide wires, balloon catheters, and an inflation device with manometer (Fig. 14.1). Guide catheters are available with multiple angulations, and balloon catheters are available in 3.5-mm, 5-mm (standard), 6-mm, and 7-mm sizes. Attachments are available to permit use with image guidance and have been found to be useful by some surgeons.5 Sinus lavage catheters are also available for use after dilatation. The balloon catheter dilation system is prepared according to the manufacturer’s instructions. If fluoroscopy is to be used to confirm placement of the guide wire and balloon, then contrast medium diluted in sterile saline/water is used to inflate the balloon so as to be visible across the ostium. The anteroposterior (AP) view is recommended during cannulation of the maxillary sinuses. In some states in the United States, use of the C-arm requires specialized training, testing, and licensing to allow its use. Maxillary sinuplasty may also be performed without use of the C-arm by means of an illuminated guide wire (Luma; Acclarent, Menlo Park, CA). This guide wire utilizes fiberoptic light transmission to allow confirmation of placement in the targeted sinus through sinus transillumination. In the event that the transillumination method is used, contrast medium is unnecessary and sterile saline or water is used. The maximum recommended pressure is 16 atmospheres (1.6 megapascal), although in practice, we have found that between 8 and 12 atmospheres (800–1200 kilopascal) is typically sufficient. The 90- and 110-degree guide catheters are recommended for dilatation of the maxillary sinus. Fig. 14.1 (A) Balloon sinuplasty (Acclarent, Inc., Menlo Park, CA) guide catheters for the maxillary sinus are available in 90- and 110-degree configurations with smaller guide size designated “s.” (B) Direct visualization system shown with guide catheter, guide wire, balloon, guide catheter handle, high pressure extension tubing and endoscope. Not shown: balloon inflation device. (Courtesy of Acclarent Inc., Menlo Park, CA) Surgical technique is demonstrated in Videos 14.1 and 14.2. The sinuplasty equipment is prepared and tested prior to use. The nasal cavity is then prepped for endoscopic sinus surgery. Oxymetazoline 0.05% is applied to the nasal cavities on cottonoid pledgets. After appropriate time for vasoconstriction, the nasal cavities are surveyed endoscopically. Local injections may be made with 1% xylocaine with 1:100,000 epinephrine at the axilla of the middle turbinate and uncinate process. We have found, however, that with sinuplasty for the maxillary sinus local injections are frequently not necessary. The 90- or 110-degree guiding catheter with guide wire is then advanced into the nasal cavity under endoscopic visualization, and passed posterior to the uncinate process. It is then rotated downward to the expected location of the maxillary ostium at approximately the level of the junction of the lower third and upper two thirds of the middle turbinate. The guide wire is then gently advanced under fluoroscopic guidance until placement in the maxillary sinus is confirmed (Fig. 14.2A). Alternatively, the illuminated guide wire may be used with the room lights dimmed to allow transillumination of the maxillary sinus. The guide wire should not meet resistance as it is advanced. The balloon is then gently advanced over the guide wire until the balloon is centered across the sinus ostium. Radiopaque markers at the leading and trailing ends of the balloon assure that the balloon is completely deployed and may be visualized endoscopically and radiographically. Fig. 14.2 (A) The guide catheter is placed at the maxillary ostium and the guide wire is advanced into the sinus. (B) The balloon is positioned across the ostium and inflated to dilate the sinus. (Courtesy of Acclarent Inc., Menlo Park, CA) After confirmation of correct placement of the balloon, the assistant slowly inflates the balloon while reading off the pressures to the surgeon (Fig. 14.2B). Pressures of 8 to 12 atmospheres (800–1200 kilopascal) are usually adequate. The uncinate process will be noted to be displaced anteriorly during inflation. Following dilation of the maxillary sinus ostium, the contrast medium or saline is slowly withdrawn into the device and the balloon is removed from the nasal cavity. Angled endoscopes are then used to view the lateral nasal wall and maxillary sinus. We recommend use of both the 30- and 70-degree scopes for this purpose to assure that the true ostium has been dilated and an accessory ostium has not been created. If this is the case, it should be joined to the natural ostium with standard endoscopic instrumentation, such as a seeker, 90-degree forceps or backbiter. If the uncinate process precludes endoscopic view of the maxillary sinus and dilation of the true ostium is in doubt, the inferior portion of the uncinate process may be removed with backbiting or angled through-cutting forceps. After the dilation has been performed, sinus lavage and biopsies may be performed as indicated. We use a 90-degree giraffe forceps with a 70-degree scope when biopsy or polyp removal may be indicated. Postoperative care is similar to traditional FESS. Standard postoperative instructions include no heavy lifting, no nose blowing, and sneezing or coughing with the mouth open. Saline rinses are begun the day following surgery. The patient may gradually resume normal routines. Narcotics and antibiotics are prescribed as necessary. Patients return for routine follow-up appointments as with traditional FESS and the middle meatus is debrided as needed, although this is frequently unnecessary. The maxillary ostium is visualized with an angled endoscope if possible, although an edematous or obstructive uncinate process may often obstruct the view. In this case, we rely on the patient’s symptoms and occasionally CT scans if necessary. We encourage use of a pediatric 70-degree scope or flexible scope for evaluation of the postdilation ostia. Potential complications for ostial dilation are similar to FESS. These include adhesions, stenosis of ostia, orbital, lacrimal, neurovascular, and intracranial injuries.6 Performing dilation, as with FESS, the surgeon must preoperatively review the patient’s CT scans, utilize his/her knowledge of paranasal sinus anatomy during surgery and be prepared to deal with complications if they arise. In practice, however, we have found dilatation of the maxillary sinus to be a very safe technique. The most common pitfall encountered is creation of an accessory ostium rather than dilating the natural ostium of the maxillary sinus. This is due to the location of the ostium and the need to pass the guide wire behind the uncinate, then anteroinferior and laterally to access the sinus. This is why we feel it is crucial to visualize the true ostium with angled endoscopes prior to termination of the procedure. In addition, inflation of the balloon may destabilize the uncinate process as it is displaced anteriorly. If the uncinate is felt to be at risk for scarring to the middle turbinate, it may be partially removed. Initial outcome data are now available for balloon dilation, confirming that it is a safe and effective technique, in selected patients (Figs. 14.3A,B). The multicenter prospective CLEAR (Clinical Evaluation to Confirm Safety and Efficacy in the Paranasal Sinuses) Study now has published 6-month, 1-, and 2-year follow-up data for its cohort.7–9 Of 142 maxillary ostia that were dilated with balloon catheters, 124 completed the 6-month follow-up with a 91% patency rate, 1% nonpatent, and 8% indeterminate due to inadequate visualization.7 At one year, 92 maxillary sinuses remained in the study: 90% were patent with 10% indeterminate.8 At 2 years, patency rates were not recapitulated; however, revision rates were reviewed, with seven sinuses in 65 patients followed for the entire 2 years needing revision. Of these seven sinuses, five were maxillary sinuses and two were frontal sinuses. These data seem to confirm that the maxillary sinus is more difficult to dilate successfully due to its anatomy. At 2 years, 51 of 60 patients (85%) reported improved sinusitis symptoms, with 77% of balloon-only patients reporting improvement, and 93% of hybrid patients reporting improvement. Lund–Mackay and SNOT-20 scores showed significant improvement in both sets of patients at 2 years as well.9 Fig. 14.3 (A) Preoperative computed tomography (CT) scan showing obstruction of the right maxillary sinus with anterior ethmoid disease.(B) Postoperative CT scan 2 years following dilation showing long-term patency of the maxillary sinus and resolution of the ethmoid disease. The FinESS sinus treatment (Entellus Medical, Maple Grove, MN) was approved for human use by the FDA in April 2008 (Fig. 14.4). This sinus treatment accesses the maxillary sinus via an antral puncture. A dual lumen catheter is then passed into the maxillary sinus. The double lumen allows use of a microendoscope to visualize the ostiomeatal complex while a balloon catheter is passed into the ostium. This is then inflated to dilate the ostium and ethmoid infundibulum. This procedure can be performed under local anesthesia. The BREATHE I clinical study is collecting long-term follow-up data, which may help establish its effectiveness and allow comparison with other sinus dilation techniques and standard FESS. Balloon catheter dilatation of the maxillary sinus is a safe, effective, and minimally invasive technique available to the sinus surgeon for a selected subset of patients. The surgeon must always be willing to convert to a traditional approach if so indicated. Due to the position of the maxillary ostium, it is recommended that it be viewed with angled endoscopes to ensure that an accessory ostium is not created that could lead to mucus recirculation. If visualization is not possible, the lower portion of the uncinate may be removed for this purpose. Fig. 14.4 (A) FinESS(Entellus Medical, Maple Grove, MN) sinus treatment system includes trocar, dual lumen cannula, balloon inflation device, and balloon catheter.(B) Dual lumen cannula allows visualization of placement of balloon catheter with a microendoscope across the maxillary sinus ostium prior to inflation. (Courtesy of Entellus Medical, Maple Grove, MN) • Patients with isolated maxillary sinus disease with failure of medical management may be candidates for balloon dilatation. • Patients with comorbid conditions may benefit from a less invasive procedure such as balloon catheter dilation. • Dilation of the maxillary sinus may be technically challenging due to the position of the ostium and uncinate process. • Correct placement of the guide wire may be confirmed either fluoroscopically or via transillumination. • Confirmation of dilation of the true maxillary sinus ostium is recommended through use of angled endoscopes, preferably 30 and 70 degree. • Balloon catheter dilatation may be combined with traditional FESS techniques. • A portion of the uncinate process may be removed to help with access in the office and surveillance. Potential complications are similar to FESS. • Long-term patency is similar to FESS.
 Indications and Contraindications for Sinus Balloon Dilation
Indications and Contraindications for Sinus Balloon Dilation
 Failure of extended medical therapy to include oral and topical steroids, as well as evaluation and treatment of allergic conditions
Failure of extended medical therapy to include oral and topical steroids, as well as evaluation and treatment of allergic conditions
 A persistently abnormal CT scan, after at least 4 weeks of appropriate (preferably culture-directed) antibiotic therapy
A persistently abnormal CT scan, after at least 4 weeks of appropriate (preferably culture-directed) antibiotic therapy
 Four or more documented episodes (data: symptoms with positive CT or endoscopic exam) of acute maxillary rhinosinusitis yearly
Four or more documented episodes (data: symptoms with positive CT or endoscopic exam) of acute maxillary rhinosinusitis yearly
 Instruments
Instruments
 Surgical Technique
Surgical Technique
 Postoperative Care
Postoperative Care
 Complications
Complications
 Outcomes
Outcomes
 Other Available Technology
Other Available Technology
 Conclusion
Conclusion

Balloon Sinuplasty for the Maxillary Sinus
Pearls
< div class='tao-gold-member'>Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


